Novel coronavirus disease is a very infectious respiratory infection transmitted from person-to-person and manifest commonly with fever, dry cough, difficulty breathing, fatigue, myalgia and dyspnea. The World Health Organization (WHO) used the term 2019 novel coronavirus to refer to a coronavirus that affected the lower respiratory tract of patients with pneumonia in Wuhan, China on 29 December 2019. Persons with comorbidities and the aged are most vulnerable to severe disease and accounted for over 40% of deaths globally.
A cross-sectional study involving 320 adult males and females above the age of 18 years was conducted across all seven sub-districts of the Kintampo North Municipal. A total of 21 communities were selected by random sampling and 15 individuals interviewed. Systematic sampling was used to select 15 houses in each community and one household selected by simple random sampling if more than one household in a house. Simple random sampling was used to select one participant for inclusion in the study. Stata version15 software was used for the analysis and reported in frequencies and percentages. Bivariate and multivariate analysis was further conducted to find associations between adherence to COVID-19 safety protocols and the demographic and main variables of the study.
About 98% of the study participants demonstrated high level of awareness regarding COVID-19. Even though about 82% of participants reported to be practicing hand washing under running water, almost of all (81.9%) do not satisfy the correct hand washing procedure. The study found significant association between education and adherence to COVID-19 safety protocols. Even though the level of awareness was very high, the study revealed that about 94% of the participants are not adhering to the various preventive measures recommended by the Ministry of Health. About 28.3% of the study participants do not know any sign or symptom of COVID-19. About 95% of the participants are worried about getting infected with COVID-19 and 96% knows the importance of wearing nose mask even though only 24.2% used a nose mask.
There is high level of awareness about COVID-19 in the public mostly through the media but most of the people do not adhere to the preventive measures to prevent themselves from infection. Intensified education and enforcement of the preventive measures will be required to interrupt the chain of transmission since the level of awareness seems not to translate to actual practice of preventing infection.
Knowledge, Attitude, Practices, COVID-19, Pandemic
Coronaviruses belongs to a large family of zoonotic viruses that usually cause illness ranging from common cold to severe respiratory diseases. They often results in a very infectious respiratory disease which is transmitted from person-to-person and manifest most often with fever, dry cough, difficulty in breathing, fatigue, myalgia and dyspnea [1]. There are several coronaviruses known to be circulating in different animal populations that have not yet infected humans. Novel coronavirus disease 19 is the most recent to make the jump to human infection. The coronavirus disease 19 infection is spread from one person to others via droplets produced from the respiratory system of infected people, often during coughing or sneezing.
The World Health Organization (WHO) used the term 2019 novel coronavirus to refer to a coronavirus that affected the lower respiratory tract of patients with pneumonia in Wuhan, China on 29 December 2019. The WHO announced that the official name of the 2019 novel coronavirus is coronavirus disease [2].
Robust estimates for coronavirus disease 19 case fatality rate are still lacking and potentially biased by incomplete outcome data and differences in testing policies. The absolute number of deaths was higher among those aged over 65 years. Persons aged 65-79 years accounted for 44% of all deaths and those aged 80 years and above for 46%. Evidence of the case fatality rate of the disease as reported in China is about 2.3% which is much lower than that of the earlier family of viruses such as SARS (9.5%), MERS (34.4%), and H7N9 (39.0%) [1].
Ventilatory assistance is required in about 10% of the hospitalized patients, and the mortality rate in patients requiring ventilator assistance, younger than 75 years of age, without major co morbidities, is minimal [3].
Globally, the World Health Organization's report as of 16th August, 2021 when this article was been written, estimated the number of confirmed cases of coronavirus disease 19 to be 207,784,507 with an estimated 4,370,424 confirmed deaths [4].
Even with the rollout of vaccines in most parts of the world the third wave of the pandemic seems to be more devastating than anticipated and some countries have so far gone back to total lockdown as the only intervention to reduce spread of the virus. The WHO has estimated that about 4,452,111,864 doses of COVID-19 vaccines have so far been administered globally [4] to eligible populations as of 16th August, 2021 but the issue of equity between countries and regional balance remains a major challenge in achieving global success. This continues requires a collective effort by all nations to ensure that no nation or eligible person is left behind in fighting the pandemic.
In Ghana, the first two cases of coronavirus disease were reported on 12 March, 2020 and since then cases of the disease have been reported in all the 16 regions of the country. Since the pandemic, Ghana recorded 111,232 confirmed cases with 930 confirmed deaths. The Ghanaian government has vaccinated about 1,271,393 of the population with at least one dose of AstraZeneca vaccine. Notwithstanding, majority of the Ghanaian population are still vulnerable since they are either not vaccinated or partially vaccinated. Only about 405,971 out of the estimated 20 million Ghanaians targeted to be vaccinated against coronavirus has received the two recommended doses of the vaccine as at the time of writing this article.
With the upsurge of the new delta variant, many countries including Ghana have witness high incidence of cases which and requires strict adherence to the safety protocols such as wearing of nose mask, constant hand washing with soap under running water, avoidance of crowded places and funerals. It is however observed that many people have relaxed the safety protocols with over ¾ of the population not wearing mask during their daily activities. These attitudes and practices have very debilitating consequences on the general public as the new wave is believed to be more severe and results in high fatalities.
This study was conducted to provide additional information on Knowledge, Attitudes and Practices towards COVID-19 pandemic preventive protocols in the Kintampo North Municipality of Ghana.
A community-based cross-sectional study was conducted to among a sample of adults 18 years and above in the Kintampo North Municipality of Ghana between April and May, 2020 to assess knowledge, attitudes and practices regarding coronavirus disease 2019. The adult population was targeted due to the perceived high risk of COVID-19 infection among them and also their high affinity of exposure to high risk areas during travel and social gatherings.
The study was conducted in the Kintampo North Municipality situated in the Bono East Region of Ghana. The Kintampo North Municipal which shares boundaries with five districts in Ghana including Central Gonja District to the North, Bole District to the West, East Gonja District to the North-East, Kintampo South District to the South, and Pru District to the South- East was established by a legislative instrument 1480 as Kintampo North District and upgraded to a Municipality status in 2003 after the creation of the Kintampo South District. The Municipality currently has an estimated projected population of 119,797 (KNMHD, 2020). The capital of the Municipality (Kintampo) widely known as the centre of Ghana serves as a major transit point for commuters from the Southern sector of Ghana to the Northern sector of Ghana. As a major transit center between the northern parts of Ghana including Burkina Faso makes keeps the town at high risk of COVID-19 transmission since travellers continues to interact with traders and restaurants to buy foodstuff or during eating. The Municipality is also noted for its tourist attraction including the Kintampo waterfalls and the Kintampo fuller falls. These tourist sites attract visitors from various parts of the country and outside of Ghana. The Kintampo waterfall which was recently upgraded with a canopy walkway attracts more tourists from all parts of the country and beyond. The tourism activities coupled with the non-adherence to the COVID-19 preventive protocols possess an additional risk of transmission of the disease in the community as many residents troop the waterfalls on daily basis for recreation. In the midst of all these risks the Municipality has only one government Hospital which serves as the major referral health facility which sometimes could be over stretched especially during the rampant road accidents that are witnessed along the Tamale-Techiman highway.
The study was conducted among male and female adults of 18 years and above residing in randomly selected communities in the Kintampo North Municipality at the time of the study. This population has constitutional right to voluntarily consent to participate in a study of this nature per the constitution of Ghana. Any person below the age of 18 years was excluded from the study.
The sample size was estimated based on 95% confidence interval and 25% prevalence as reported in a similar study by [5]. The sample size was estimated using Cochran's formula (n = z2 p (1-p)/e2). A sample size of 320 was used for the study with an estimated 10% non-response rate.
Cluster sampling technique was used to select communities from each sub-district for the study. The seven administrative sub-districts defined by the Municipal Health Directorate of the Ghana Health Service were used as clusters for the study. In each cluster (sub-district) three communities were randomly selected and 15 participants interviewed. Systematic sampling with interval of 2 was used to select the subsequent houses for the study. In each house simple random sampling was used to select a household in a situation where there were more than one household in a house. Simple random sampling was again used to select one participant from a household until the 15 participants interviewed by consent.
A semi-structured questionnaire was used to collect the data. The questionnaire was divided into three sections: demographic, knowledge, attitudes and practices regarding the preventive measures of COVID-19. The instrument was developed by the investigators using the variables studied. The data collection tool was pretested in three different communities, Jema, Nante and Nante Zongo in Kintampo South district and analyzed and a Cronbach's alpha of 0.84 was achieved as acceptable coefficient for reliability and validity.
Research assistants were enrolled and trained on the instrument to estimate the time that will be taken to complete one questionnaire and for translation into Akan, Bono and Mo languages during administration. The interviews were conducted by the research assistants and directly supervised by the principal investigators for a period of 1 week. Interviews were done face-face while ensuring that participant's confidentiality and privacy were respected. The study recorded a 100% response rate.
The data was first manually validated for completeness and clarity and coded for entry into statistical software. The data was entered and analyzed using Stata® Statistics/Data Analysis software, (College Station, Texas 77845 USA) version 15. Descriptive analysis was done and presented in tables and figures with frequencies and percentages. Logistic regression analysis was performed on the demographic variables and the main variables to establish statistical associations. Adherence to COVID-19 protocols was the dependent variable used in this study. The study reported unadjusted odd ratios, p-values and confidence intervals for the bivariate analysis. The significant statistical level was set at (p = 0.05). Variables with statistical significance (p = 0.05) were further analyzed in a multivariate model and the adjusted odds ratio, p-values and 95% confidence intervals reported.
The investigators sought consent from all the participants prior to the interview. The objectives of the study were explained to each participant to make an informed decision to participate. Written approval was also received from the Kintampo North Municipal Health Directorate (Reference No: KNMHD 05/20). Only participants who signed/thumb printed the consent form were interviewed. Participants were also made to understand that participation in the study was voluntary and that every participant had the right to withdraw at any time during the study. Confidentiality of data collected was ensured by using identifiers rather than names of participants and the participants were equally assured that the data collected will only be used for the benefits of informing decisions on how to interrupt transmission of COVID-19 in the Municipality. The participants were equally assured of the safety and confidentiality of the information collected by ensuring that it would be stored in an electronic format on different personal computers and as hard copies under key and lock in fire-proof cabinets. Apart from those involved in this study such as the data collectors and principal investigators no other party was given access to the raw data collected.
The study involved only the administration of questionnaires with no risk to the participants. Therefore, no compensation package was given to the participants. The administration of the questionnaire lasted about 30 minutes per participant and they were told before the start of each interview session. Even though participants in the study did not receive any material benefits from the study, their participation in the study helped them acquire some understanding on the preventive measures regarding COVID-19 to protect themselves and their communities.
The study was conducted among adults aged 18 years and above. Majority (38.1%) of the participants were 18-28 years while the least (16.6%) age group was above 50 years. Almost equal proportions of males (50.3%) and females (49.7%) participated in the study. Majority of the study participants were farmers (54.7%), married (58.8%) and Christians (52.2%) respectively. Majority (42.2%) also had no formal education while few (4.1%) had attained tertiary level of education (Table 1).
Table 1: Background characteristics of study participants. View Table 1
The study revealed that 314 (98.1%) of the participants had heard about the COVID-19 pandemic (95% CI = 96%-99%). Notwithstanding, out of the total participants aware of COVID-19, 93.9% did not fully adhere to the COVID-19 protocols (Figure 1).
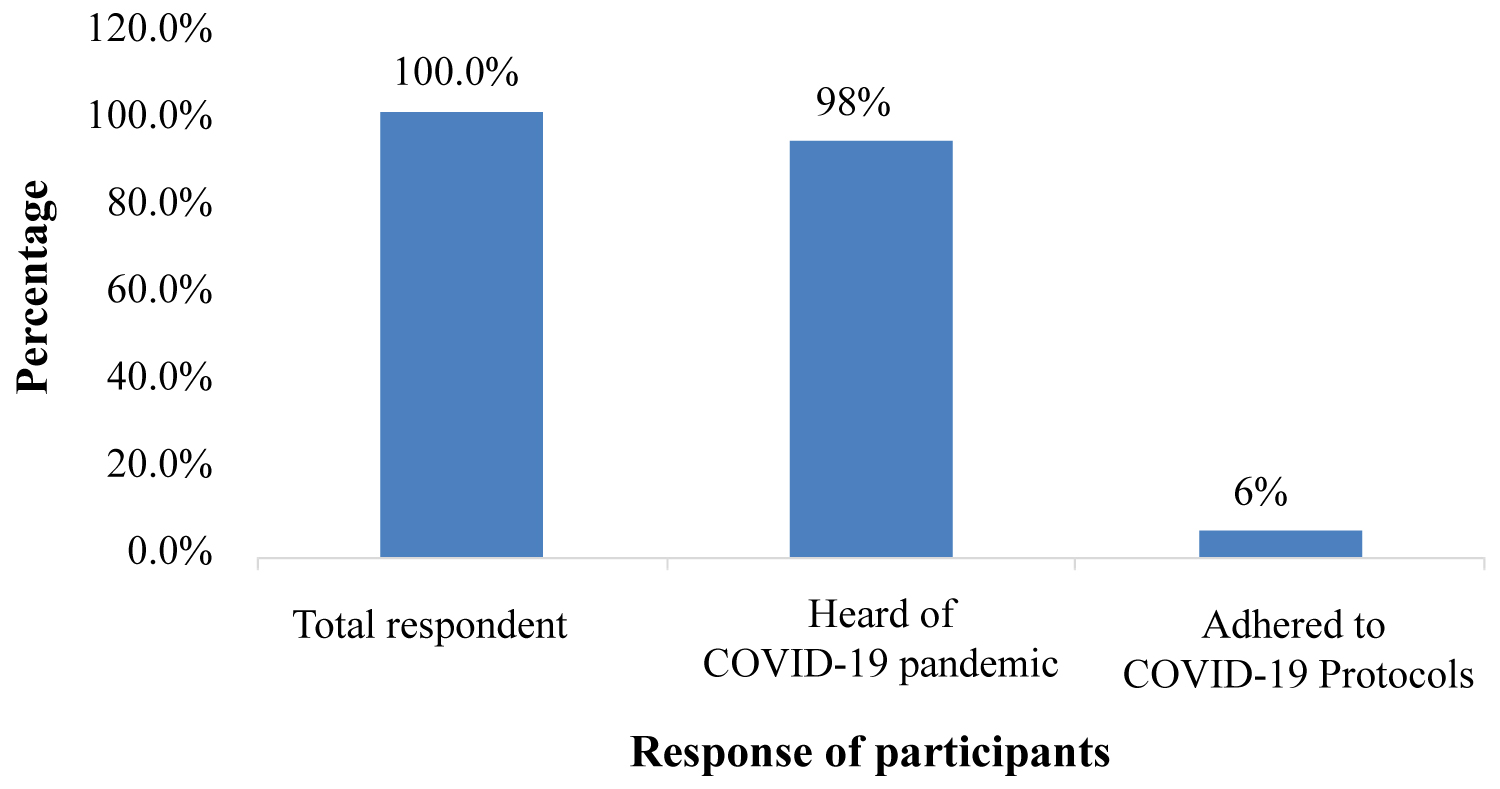 Figure 1: Comparison between COVID-19 awareness and adherence to protocols.
View Figure 1
Figure 1: Comparison between COVID-19 awareness and adherence to protocols.
View Figure 1
The bivariate analysis presented in Table 2 showed that participants' level of education was the only variable significantly associated with adherence to the COVID-19 protocols (p < 0.016).
Table 2: Bivariate analysis of the association between background characteristics and adherence to COVID-19 protocols. View Table 2
Interesting among the findings of this study was that only 24.2% of the study participants used alcohol-based hand sanitizer and nose masks when going out of home, 92% of the participants did not observe good cough etiquette (coughed without using tissue or did not cough into their elbow), 70% did not observe social distance, 82.2% of the participants washed their hands under running water but most (81.9%) did not follow the correct hand washing procedure and more than half (53%) said they will visit the health facility rather than calling the COVID-19 hotlines for medical attention when suspect COVID-19 infection.
Commendable among the findings was that most (81.53%) of the participants observed the recommended COVID-19 greeting protocols, thus stayed at a distance to greet other people verbally, wave hands or bow to prevent COVID-19 transmission. Establishing the link between adherence to COVID-19 protocols and knowledge, attitude and practices, five variables were found to be statistically significant.
Sources of information on COVID-19 and participants' knowledge on the vulnerable population of COVID-19 were the significant variables under knowledge with p-value < 0.02 and < 0.041 respectively. Drinking lemon/ginger/garlic was the only significant variable under attitude with p-value < 0.001. Observation of COVID-19 greetings protocol and the action by participants upon suspicion of COVID-19 infection were also significantly associated with adherence to the COVID-19 protocols with p-value < 0.001 and < 0.017 respectively (Table 3a and Table 3b).
Table 3a: Bivariate analysis of the association between adherences to COVID-19 protocols and knowledge, attitude, and COVID-19 practices. View Table 3a
Table 3b: Bivariate analysis of the association between adherences to COVID-19 protocols and knowledge, attitude, and COVID-19 practices. View Table 3b
The study found a statistically significant association between variables such as educational level of the participants, knowledge of vulnerable population to COVID-19 and action of participants when they suspect COVID-19 infection and adherence to COVID-19 protocols, with the crude odds > 1 and p < 0.05. After adjusting for confounders (Table 4), participants with tertiary level of education had 7.6 odds of adhering to the COVID-19 protocols compared to those without formal education (p < 0.05).
Table 4: Multivariate analysis of factors associated with adherence to COVID-19 protocols View Table 4
The outbreak of COVID-19 since December, 2019 the whole world has been at the centre of emergency and some countries have implemented repeated lockdowns as measures to curb the spread of the virus. Public education continues to be one of the main tools to influence knowledge and change attitudes and behaviours to end the pandemic. While cases continue to shoot up and all countries working towards procuring vaccines to protect the citizenry against the virus, our knowledge, attitudes and practices towards the preventive protocols remains fundamental in ending the spread of the virus. There is also an ongoing controversy in the public about the safety of the vaccine and an anticipated high vaccine hesitancy rate especially in Africa due to the ongoing controversy. This comes to buttress the important role education of the public to increase knowledge, attitude and practices on all aspects of COVID-19 may play for the world to succeed. The study was conducted among adults 18 years and above residing in all the seven Sub-districts of the Kintampo Municipality to ascertain their knowledge, attitude and practices regarding the COVID-19 preventive protocols.
The study revealed almost all ages had heard about COVID-19 indicating high level of awareness irrespective of age. There was no variation in the male to female representation in the study participants. However, in a similar studies in Africa and Asia, females were found to have adequate knowledge than their male counterparts contrary to the finding of this recent study in Ghana [6,7]. While most of the participants were reported no to have had formal education and farmers they was no significant awareness gap among the other categories in the study. The study was dominated by people of the Christian religion. Meanwhile over three-quarters of the participants across occupation, educational level, marital status and religion had heard about the coronavirus pandemic. However, been a driver, public servant, JHS level education, SHS level education, tertiary education, divorced, separated or widowed and traditional religion suggest increasing ones level of awareness of the coronavirus pandemic.
The study investigated the level of knowledge of the participants on coronavirus disease to ascertain whether mere been aware of the disease indicates ones knowledge about the signs and symptoms, mode of transmission, preventive measures and risk factors of complications from the disease. The study reported almost all participants were aware of the disease through the various media platforms in the Municipality. This was also reported by [8-10] in similar studies in Africa where almost ninety percent of participants were aware and demonstrated knowledge of coronavirus disease.
Also, [11] in assessing the knowledge, attitudes and practices of dentists regarding COVID-19 reported almost all the participants had ever heard about the coronavirus disease. Contrary to these findings however, [12] reported an average level of awareness in their study among Arabic speaking Middle East countries (Jordan, Kuwait and Saudi Arabia). Awareness about the coronavirus disease alone should not be basis to conclude that people have adequate knowledge about the causes, signs and symptoms, prevention and control measures as well as adapting positive attitudes towards prevention against the disease. While the study revealed the most source of information was the media, health workers were found to play a very significant role in media broadcasting in technical discussions and education of the public. The media, especially the electronic was also cited in the study by [9] among government employees studied in Ethiopia.
Health workers particularly used the media to educate the public on the signs and symptoms, causes, measures of prevention, sources of infection, mode of transmission and where to seek health care due to the fact that social gatherings were banned by the government and community education and durbars could not be organized. This finding was supported by a study by [13] in Iran where a higher proportion of the population reported the media as the main source of information for COVID-19. While the media might be very significant in disseminating information about COVID-19 to increase awareness and knowledge, the public should also be very cautious of some misleading information from other sources circulating in the media. One must rely on information from very prominent sources such as the Ministry of Health, Ghana Health Service, World Health Organization and other related organization of international repute for information regarding COVID-19. Health authority should also take conscious steps clear misconceptions about faults information that might find its way into the public domain through the media landscape. All the study participants who have ever heard about COVID-19 could mention at least one mode of transmission of the disease.
Despite the high level of awareness reported in this study only 1 in 10 had knowledge about COVID-19 safety protocols outlined by the Ministry of Health compared to about 3 in 10 in a similar study conducted in Iran. Poor knowledge about the safety protocols increases the risk of getting infected with the virus. The study further established about 7 in 10 of the participants knew the signs and symptoms of coronavirus disease. This report is in contradiction with the study conducted among government workers in Ethiopia where over ninety percent were reported to have knowledge on the signs and symptoms and other preventive measures of COVID-19 [9]. Similarly, a study in the United Arab Emirates also reported participants had high knowledge regarding COVID-19 [14,15]. Understanding the signs and symptoms of COVID 19 can empower the public to seek early medical care to ensure early treatment, reduce complications and death of affected persons and limit transmission close relations. Knowledge of the signs and symptoms may also ensure early isolation and quarantine to interrupt transmission among households and closely related persons in the public. Subsequently, the cases can be contained and the public will be well informed about the disease.
There is an urgent need to intensify public education on the various preventive measures to increase knowledge interrupt transmission of the infection in the community. About a quarter of the participants do not have knowledge about the most vulnerable population at risk of the complications of COVID-19 and should be extra vigilant to avoid getting infected. Knowledge of the vulnerable population might increase the public's level of consciousness to observe the restrictions and other preventive measures.
The study indicated that almost all the participants were concerned about the COVID-19 pandemic and leaving with some fear in the Kintampo Municipality. Similarly, [16] reported in their study that majority of the respondents perceived COVID-19 risks and impacts seriously and worried about themselves and loved ones getting sick with COVID-19, worried about spreading COVID-19 to others and worried about the impact of COVID-19 on their work livelihood and the economy.
The study found very good attitude towards the use of face mask among the participants consistent with a similar study by [17] where they also report majority of the respondents strongly agreed that transmission of COVID-19 could be prevented by following universal precautions given by World Health Organization. The finding was also in agreement with a study conducted by [18] which indicated that majority of participants shows a positive attitude towards the COVID-19 pandemic.
About half of the participants did not show good attitude in observing good cough etiquette. Few of the participants believed that alcohol consumption and regular sexual intercourse reduces one risk of contracting coronavirus infection. About 7 in 10 participants' believe that consumption of a combination of lemon/ginger/garlic drink can prevent people from COVID-19 infection. This was also cited in a study by [19] where they reported 4 in 10 persons agreed eating garlic can be an effective measure against COVID-19.
The study reported that 8 out of 10 practice hand washing under running water, similar to the findings of [19] that about 9 out of 10 respondents washed their hands under running water. Adherence to hand washing under running water was reported in other studies across the world to be high [20]. This indicates a generally acceptable practice of hand washing under water among the participants to prevent infection with the coronavirus disease. While hand washing under running water was highly practiced among the participants, the procedure was observed to be wrong among majority of those who reported practicing hand washing under running water. Only 2 out of 10 of those who reported to wash their hands under running water adhere to the WHO recommended hand washing procedure. Similar reports were achieved in other studies [21,22].
The study observed majority of the participants do not practice proper cough etiquette. Only 1 out of 10 participants cover their mouth and noses with tissue when coughing or sneezing, or cough into their elbow as against 9 out of 10 observed by [19]. Since good cough etiquette reduces the risk of spread of the virus in the environment much attention should be focused in educating the public on proper cough/sneeze etiquette in Kintampo North Municipality.
Also, only 3 out of 10 participants uses alcohol based hand sanitizer as a measure of preventing infection compared to 9 out of 10 in a study by [19]. Since majority of the participants were farmers and never had formal education, their financial capability to purchase and use alcohol based hand sanitizer might have contributed to the low practice. The study also observed that only 3 out of 10 participants practice social distancing. The study overall observed that majority of the participants do not practice the recommended COVID-19 preventive measures. Only 1 out of 10 the study observed practice the preventive measures compared to about 9 out of 10 in a similar study by [13]. This should be a worry to health authorities as the surge in incidence of the new delta variant have been reported in the Bono East Region of Ghana.
The study however observed that majority of the participants adhere to the practice of not shaking hands but either wave, use their elbow or greet their peers and neighbours verbally. The avoidance of handshakes was equally reported in other studies in Africa and Asia [15,23] among adult population. Only 2 out of 10 participants were however observed to still practice handshaking and hugging. This finding was also observed by [19] where they reported 9 out of 10 participants adhere to recommended greeting practices.
The study performed statistical analysis to establish associations between dependent and independent variables. The study found statistically significant association between education and adherence to COVID-19 safety protocols. Participants who had at least JHS education, practice Islamic region, married or being single to influence the practice of hand washing with soap under running water. Hand washing with soap under running water remains probably the cheapest yet most significant measure to interrupt transmission when done properly. Health authorities should therefore intensify education to encourage hand washing with soap under running water especially in schools, churches and other places where people gather.
While a population-based study in Iran by [13] reported factors such being male, having non-healthcare related professions, being single, and having lower level of education to be significantly associated with low knowledge on COVID-19, this study did not record any significant variation in level of knowledge across the demographic characteristics of the participants. The study however agrees with [13] that knowledge was higher among married people and those who had higher education. Our study also did not record statistical significant level between age and knowledge as reported in a study by [17] in Pakistan where they reported a significant association between age and knowledge of COVID-19. The findings of the recent study also contradicts the findings of a study among Arabic speaking Middle Eastern countries (Jordan, Kuwait and Saudi Arabian) by [12] where age was again found to be statistically significant to high knowledge regarding COVID-19.
The study however found statistical association between practicing recommended preventive measures and action taken when COVID-19 is suspected, knowledge on mode of transmission of COVID-19, observing prevention protocols at crowded places knowledge of signs and symptoms of COVID-19 and knowledge of vulnerable population of COVID-19. Univariate analysis in this study shows that level of education is significantly associated with adherence to COVID-19 preventive measures, consistent with the findings of [7,13]. Higher level of education was found to increase the odds of practicing COVID-19 preventive measures as reported in many other studies [20,24,25]. This observation was consistent with other studies conducted in Asia where education was cited to significantly influence adherence to COVID-19 preventive measures [26,27].
In the multivariate analysis however, the study established that only educational level of participants showed statistical significance. Health authorities and stakeholders should therefore intensify education to increase knowledge on the signs and symptoms of COVID-19 and the recommended preventive measures to prevent further spread of the virus.
The research team would like to express our gratitude to Paul Awuffor, Maclean Apoyongo, Moses Ayariga, Isaac Adjei, Abdulai Razak Anane and Ibrahim Najas for their support during the development of the survey and data collection.
Mukasa Kabiri conceptualized the study. Samuel Adusi-Poku, Augustine Baffoe & Mukasa Kabiri designed the survey and interpreted data; Mukasa Kabiri, Augustine Baffoe & Samuel Adusi-Poku drafted the manuscript; Mukasa Kabiri, Augustine Baffoe & Samuel Adusi-Poku performed the data analysis; Mukasa Kabiri, critically reviewed and improved the manuscript; Kwabena Opoku Adusei, Paapa Puplampu & Emmanuel Kwaku Ofori improved data interpretation and revised the manuscript. All the authors substantially contributed to the study and approved the final version of the manuscript.
This study was supported by the College of Health and Well-Being, Kintampo; the Ministry of Health, Ghana. The funders of this study did not play any role in the study design, data collection and analysis, or preparation of the manuscript.
On very reasonable request, the datasets used and analyzed in the recent study are available from the corresponding author.
The study and consent to participate were approved by the Kintampo North Municipal Health Directorate (KNMHD No. 05/20). All consents were voluntarily signed by participants who were all adults.
Not applicable.
The authors of this research have no potential conflict of interest financially or otherwise.