Background: Ventriculoperitoneal shunting (VPS) is a neurosurgical procedure used to treat hydrocephalus. However, after this procedure, the surgical site infection rates and associated risk factors remain unclear. Most studies do not apply clear criteria for the definition of surgical site infection (SSI), hindering its clinical applicability.
Methods: We conducted a retrospective, case-control study to evaluate the risk factors for SSI after VPS. The National Healthcare Safety Network (NHSN) criteria were used to define SSI. A case was defined as any case of VPS with confirmation of SSI, and the control was defined as patient who underwent VPS without SSI after the procedure. Data were collected from patients undergoing VPS admitted to a hospital in Brazil between January 2007 and December 2011.
Results: SSI occurred in 15.7% of patients, with organ/space SSIs being the most common (89.8%). Staphylococcus epidermidis was the most frequent (30.4%) of the positive cultures. Of the total patients, 39.5% were under the age of 1 year and had an increased risk of infection at the surgical site after VPS. Preoperative bath was associated with a lower number of SSIs.
Conclusions: This study provides important information about SSI rates, risk, and protective factors in patients who underwent VPS in Brazil.
Ventriculoperitoneal shunt, Surgical wound infection, Neurosurgical, Hydrocephalus, Infection
Ventriculoperitoneal shunting (VPS) is a neurosurgical procedure used to treat hydrocephalus [1-3]. After this procedure, some mechanical or infectious complications require repeated care [4], leading to severe conditions and higher mortality rates [5,6].
In general, VPS-related infection rates range from 3% to 12% when the procedure is performed under ideal conditions, such as in internationally recognised neurosurgery institutes in developed countries [7-10]. However, in some circumstances, surgical site infection (SSI) rates may occur in up to 20% of all surgical procedures [5,11].
Factors associated with the risk of VPS infection include hydrocephalus, age, primary shunt insertion, meningitis, inadequate surgical technique, prolonged operative time, presence of cerebrospinal fluid fistulae, scalp necrosis, and abdominal perforation [12]. Other less frequently mentioned factors are premature birth, chemotherapy, number of manual contacts between the surgeon and the drainage system, experience of the surgical team [13], sex, birth weight, catheter blockage, and infection at other neurological sites [14,15]. However, the data are not comparable because, in most studies, the definition criteria for SSI are unclear. This study aimed to determine the frequency of infectious complications and the risk factors associated with VPS at our institute.
To the best of our knowledge, this is the first study to use an internationally validated methodology, such as the National Healthcare Safety Network (NHSN) criteria, to compare SSI rates regardless of the institution and the case's complexity. Furthermore, this study describes the risk factors associated with infection following VPS procedures, highlighting possible interventions to prevent such events.
We used a retrospective case-control study design to assess the risk factors for SSIs after VPS. We followed the NHSN criteria to define SSIs (Table S1). A case was defined as any case of VPS with confirmation of SSI, and the control was defined as a patient who underwent VPS without SSI after the procedure. Patients who underwent VPS between January 2007 and December 2011 were included in the analysis. Patients were followed up for 1 year after the procedure. The study was conducted at the Hospital das Clínicas of the Federal University of Minas Gerais (HC-UFMG) in Belo Horizonte, Minas Gerais, Brazil.
Collected data included demographics (sex and age), surgery characteristics (potential contamination wound, hospitalization/preoperative > 24 h, trichotomy, preoperative bathing, antimicrobial prophylaxis, and indication for VPS surgery), previous infection (previous neurological infection, colonisation by multidrug-resistant microorganisms, concomitant infection, urinary tract infection, pneumonia, sepsis, gastrointestinal infection, and meningitis), comorbidities, and lifestyle (diabetes mellitus, use of immunosuppressants, corticoids > 1 week, smoking, alcoholism, and elective procedure).
The procedure-related variables included first VPS implantation (when the patient first underwent valve implantation), VPS revision (when the previous valve was maintained but manipulated during the procedure to correct liquor drainage flaws), and VPS reimplantation (when the patient previously had a VPS implant that needed to be replaced for some reason).
Regarding the potential for wound contamination, the following classifications were considered as established by the Center for Disease Control and Prevention (CDC): Clean (uninfected operative wound in which no inflammation is encountered and the respiratory, alimentary, genital, or uninfected urinary tracts are not entered), potentially contaminated (operative wounds in which the respiratory, alimentary, genital, or urinary tracts are entered under controlled conditions and without unusual contamination), contaminated (open, fresh, accidental wounds, and operations with significant breaks or use of unsterile technique), and infected wounds (including old traumatic wounds with retained devitalized tissue and those that involved existing clinical infection or perforated viscera).
This study also evaluated data related to the microbiological examination of liquor, blood, and secretion of the surgical wound (microbiological data were obtained from reports issued in the institution's laboratory), and the presence of potential non-infectious complications after VPS (subdural hematoma, deep vein thrombosis, neurological sequelae, and VPS dysfunction).
The data were analysed using the Statistical Package for the Social Sciences (SPSS®, version 19). Chi-square tests (Pearson and Fisher's Exact) were used for the analysis of categorical data and Mann-Whitney U for the analysis of the medians. A stepwise logistic regression model was adjusted with a significance level of p < 0.05 with the associated risk factors. To test which risk factors contributed to the event's occurrence, a p < 0.20, was considered for each variable tested to adjust the model. This study was analysed and approved by the Research Ethics Committee of the Federal University of Minas Gerais (UFMG) and was submitted to Resolution 196/96 and the supplementary rules of Resolution 347/05, under opinion number 965116.
The patients' demographic and clinical characteristics are shown in Table 1. Of the 438 patients, 225 (51.4%) were men and 213 (48.6%) were women. Most patients were aged less than 1 year or older than 16 years. The percentage of subjects who underwent the first implantation of VPS was predominantly higher (211, 48.2%), compared to those who underwent revision (114, 26.0%) and reimplantation (113, 25.8%). Of the total patients, 69 (15.7%) had SSIs, 37 (53.6%) had a positive culture, and 32 (46.4%) were diagnosed with SSIs based on clinical criteria. Infections were classified as meningitis/ventriculitis (89.8%), superficial infection (5.8%), and deep infection (4.3%).
Table 1: Ventriculoperitoneal shunt (VPS): Demographic data and clinical characteristics. View Table 1
The aetiology of hydrocephalus was diverse, with congenital malformations in 210 (47.9%), tumour in 63 (14.4%), and brain stroke in 30 patients (6.8%). In patients with SSIs, the predominant aetiologies for hydrocephalus were congenital malformations in 41 (9.36), tumour in 8 (1.82%), and prematurity in 7 patients (1.59%). Patients without SSIs had a higher frequency of mortality (29, 7.9%) than those with SSIs (4, 5.8%) (Table 2). However, the presence of SSIs significantly increased the length of hospital stay (Figure 1).
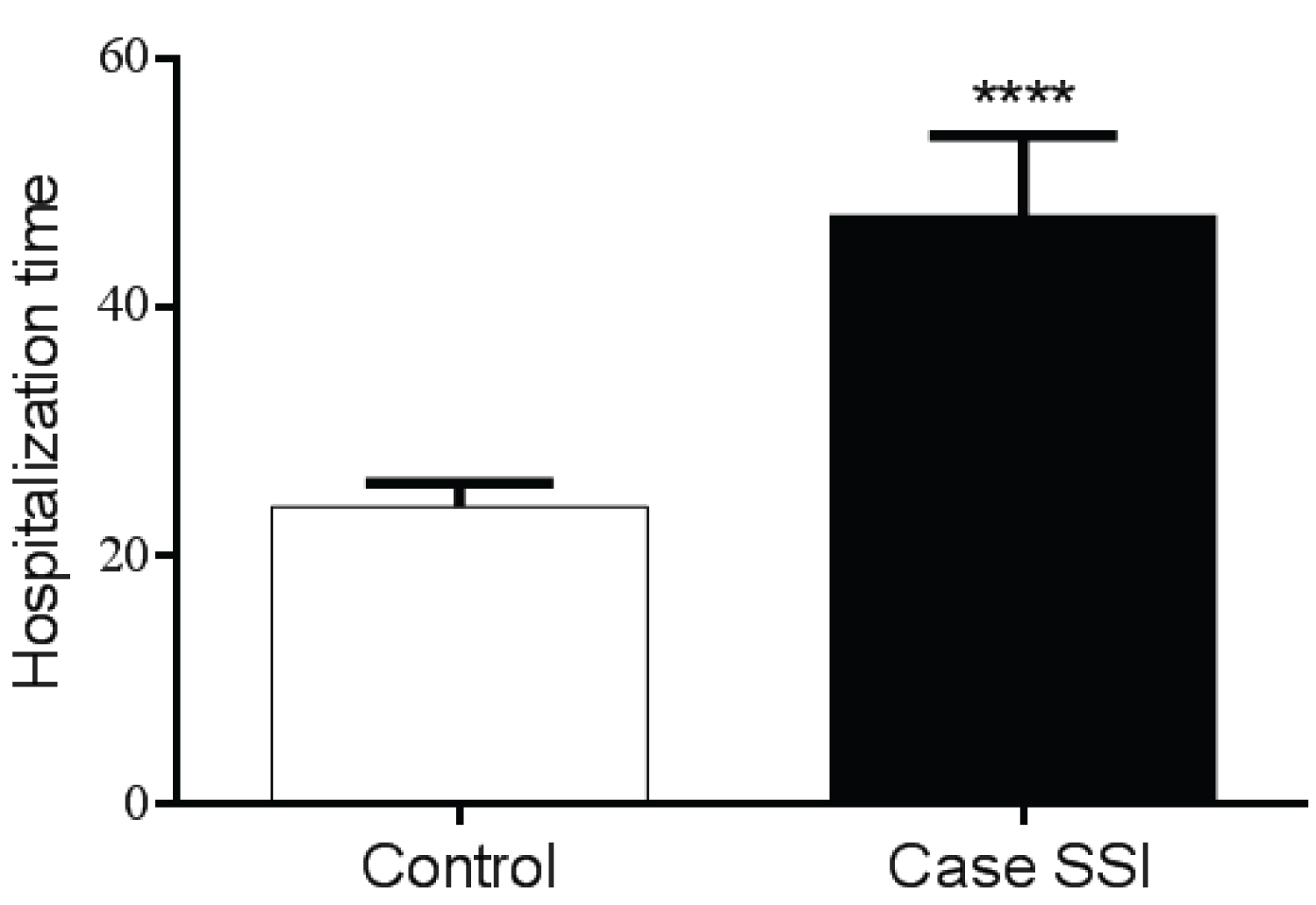 Figure 1: Length of hospital stay for patients who received ventriculoperitoneal shunt (VPS), and did or did not have surgical site infection (SSI).
Figure 1: Length of hospital stay for patients who received ventriculoperitoneal shunt (VPS), and did or did not have surgical site infection (SSI).
Control: Patients who underwent VPS and did not develop SSI. **** p < 0.0001 in relation to the control.
View Figure 1
Table 2: Distribution of hydrocephalus aetiology among patients with VPS according to the SSI. View Table 2
According to the present study, 69 (15.7%) patients presented with clinical signs of SSI according to the NHSN criteria (Table 1). Of these, only 37 (53.6%) had a positive culture from different clinical specimens (liquor, blood, and wound secretions), 11 were positive for (22%) Staphylococcus epidermidis, 6 (12%) Staphylococcus aureus, 6 (12%) Pseudomonas aeruginosa, 6 (12%) Escherichia coli, 3 (6%) Klebisiella pneumoniae, 3 (6%) unidentified Gram-positive cocci, 3 (6%) Candida sp., 2 (4%) Acinetobacter baumannii, 2 (4%) Staphylococcus sp., 2 (4) Cryptococcus sp., 1 (2%) Staphylococcus warneri, and 1 (2%) Stenotrophomonas maltophilia (Table 3).
Table 3: According to the clinical specimen, the distribution of microorganisms isolated from patients with SSI after ventriculoperitoneal shunting. View Table 3
Total 69 (15.7%) SSIs occurred, 43 (62.3%) in clean wounds, 15 (21.7%) in potentially contaminated wounds, 6 (8.7%) in contaminated wounds, and 5 (7.2%) in infected wounds. However, there was no statistical association between the contamination potential and the SSIs (Table 4).
Table 4: Association of surgery characteristics with SSI in patients with VPS. View Table 4
The infection risk was lower in 199 (87.3%) patients who took bath with antiseptics before the procedure (p = 0.005). However, logistic regression did not confirm this as a protective factor in this series of cases (Table 4). The hospital has an SSI prevention protocol that recommends an antiseptic bath before the procedure; however, this recommendation is not implemented in all cases.
According to the definition, 344 (78.5%) patients received antimicrobial prophylaxis in the operating room, and 94 (21.5%) were administered some antibiotics on the day of surgery (Table 4). Therefore, it is possible to infer that all patients had antimicrobial coverage at the time of surgery.
For the adjustment of the logistic regression model, variables that showed statistical significance with p < 0.20 in the univariate analysis were considered. The possible risk factors selected were: age < 1 year, concomitant infection, colonisation by multidrug-resistant microorganisms, preoperative bath, VPS dysfunction, antimicrobial prophylaxis, and alcoholism.
A logistic regression model was adjusted and the factors that contributed to the occurrence of SSIs in the VPS were patients younger than 1 year of age (p < 0.001; odds ratio [OR] 9.6; OR 95% 2.8 - 32.6) (Table 5), which increased the chance of occurrence by 9.6 times and preoperative bath (p = 0.044; OR 0.3; OR 95 1.1-35.0) (Table 4), which resulted in a 1.1 fold reduction in the chance of occurrence.
Table 5: Association of sex and age with SSI in patients who received ventriculoperitoneal shunt. View Table 5
Other factors were also analysed in this study, such as sex (Table 5), previous infection (Table S2), comorbidities, and lifestyle (Table 6), but without any association with SSI occurrence.
Table 6: Association of comorbidities and lifestyle with SSI in patients with ventriculoperitoneal shunt. View Table 6
Of the patients with SSIs after VPS, 33 (47.82%) were maintained, and subsequent replacement of the VPS system was performed; 12 (17.39%) required externalisation and subsequent exchange; 11 (15.94%) underwent external ventricular drainage (EVD) withdrawal and re-insertion with DVP; and 10 (14.49) did not require changing the system. Of the total patients with SSIs after VPS, 58 (84.0%) were cured and 8 (16.0%) needed a treatment change (Table 7).
Table 7: Treatment of SSIs and clinical prognosis. View Table 7
In this study, the SSI rate after VPS was higher than the NHSN reference rate. The most recently published studies report an SSI rate between 3% and 13.6%, performed under ideal conditions [6-8,10,16]. In scenarios similar to our reality, the SSI rates have been reported to be higher, reaching up to 50%, with an average of 25% [3,12,17]. This study considered the follow-up of 1 year after the procedure, as recommended by the NHSN [18]. Most publications use a shorter follow-up period in the literature, which may explain the higher infection rates. In 2013, after completing this study's analysis, a new NHSN criterion (2015) was published, and new analyses were carried out following this criterion.
Quality of care and socioeconomic conditions play essential roles in developing an infection. However, our study did not assess the socioeconomic status of the patients.
Approximately 89.8% of infections were organ/space infections (meningitis/ventriculitis), contrary to the findings of other studies [12]. We believe that these differences occurred because both infections of the VPS tract and skin reactions were considered, contributing to the increase in superficial infections. In this study, we chose not to assess skin reactions because of the difficulty in differentiating small hyperaemic areas from tract infections and the limitations of the records.
Some studies [8,12] reported that 81.3% to 91.4% of the first signs and symptoms of infection occurred up to 90 days after implanting the VPS system, similar to the results found in our evaluation. Based on this, we can conclude that in all studies, the signs and symptoms had an early onset, suggesting that the VPS system was contaminated at the time of implantation.
Generally, SSI rates are higher in paediatric patients [8,19]. In this study, age ≤ 1 year was a statistically significant risk factor for the occurrence of infection, and 39.5% of the patients were less than 1-year-old, contributing to an increased infection rate. Another observation was that approximately two-thirds of the patients were under 16 years of age (Table 1). We must highlight that the reduction in the age of patients tripled the risk of developing SSI in our results.
Postoperative care, including antiseptic bath is considered a protective factor against SSI. Although it showed statistical significance in the univariate analysis in the study, it did not remain in the regression model's adjustment. The bath's purpose is to render the skin clean by removing the transient microbiota and some resident microbiota [20,21]. In a recent study [17], preoperative bath was not statistically significant, but the reduction in patients' microbiota was shown to have some benefits.
System dysfunction often leads to an accumulation of cerebrospinal fluid in the ventricles, which causes greater dissemination of potentially infectious microorganisms. However, the SSI itself can cause dysfunction in the VPS system due to blockage by reduction in cerebrospinal fluid drainage or decrease in absorption by the peritoneum or pleura [22]. Therefore, it is impossible to identify whether this is a cause or effect of SSIs.
Coagulase-negative Staphylococcus was the most commonly isolated microorganism. Similar results have been observed in other studies [3,19,23].
The retrospective nature of data collection limits this study because it is linked to descriptions in medical records. Moreover, this was a single-centre study with a limited sample size (although quite representative compared to the number of cases reported in other studies). In several studies, the methodology used to diagnose infection was not standardised, and varying criteria were used. Standardising data collection and SSI diagnosis using the NHSN methodology could help compare infection rates and potential risk factors across different institutions.
Our study was retrospective, and the data collected mainly reflected the risk factors related to the patient. However, we know that some factors related to the environment, especially during the surgical procedure, such as keeping the operating room doors closed during the procedure, limiting the number of people in the surgery room [24], changing the intraoperative gloves [25,26], and maintaining the sterility of the catheter can benefit the reduction of SSIs [27].
In this study, the population evaluated was predominantly paediatric patients, and patients younger than 1 year of age were at a higher risk of developing SSIs (Table 1). The preoperative bath was considered a protective factor against the development of SSIs (Table 4). The SSI rate was 15.7% (n = 69) overall, and for clean surgeries was 15%, a rate higher than that expected for the procedure. In our study, the most prevalent topographies for SSIs were meningitis/ventriculitis according to the NHSN criteria. We suggest conducting a prospective multicentre study with age matching and application of the NHSN methodology, as it would increase the number of cases for evaluation, allow comparison with other reference centres, and possibly support further discussion.
We thank the members of the Infection Control Service and the Neurosurgery Department of Hospital das Clínicas, Federal University of Minas Gerais (UFMG), for their assistance with this study. We also thank the Graduate Program members at UFMG and the students who were always available to assist in data collection.
All co-authors have seen the manuscript and agree with its contents. There is no financial interest to report.
All co-authors have seen the manuscript and agree with its contents. There is no financial interest to report.