Background: Viral hepatitis B is a major public health problem worldwide. Their magnitude stems from their frequency and their short- and long-term health impact due to their evolutionary potential and therefore their complications.
The objective of our work is to establish the epidemiological profile of viral hepatitis B in western Algeria and to identify the main prognostic factors associated with the progression of liver fibrosis.
Methods: A cross-sectional descriptive study was carried out in Western Algeria. Information on patients with viral hepatitis B (VHB) was collected prospectively from January 2013 to December 2016. Cox's model was used to model the instant risk logarithm based on a set of predictors predicting the progression of fibrosis over time. The student's t-test and Analysis of variance (ANOVA) were used for the comparison of continuous variables.
Results: A population of 271 patients was collected. The sex ratio was 1.22. Metabolic syndrome was found in 3.0%. Severe fibrosis (F3-F4) accounts for 12.2% of VHB cases. The discovery of viral infection was clinical (asthenia and jaundice) in 40.2% of cases. The patterns of contamination reported in our study population are represented mainly by care (68.6%) and the use of traditional practices (8.9%) such as hijama, scarification and tattooing. Cirrhosis is found in 14.8% of VHB cases with an average age of 55.4 years. More than 25% of cirrhotics are diabetic. According to Cox's modelling, Hepatocellular Carcinoma is the prognostic factor of mortality in viral hepatitis B associated with HBe Antigen.
Conclusion: The most documented mode of contamination in our population, after that related to care, is the use of traditional practices; which could direct us to a population that should not be overlooked in terms of screening and awareness. Our study confirms that the rate of progression of fibrosis is not linear over time but rather an exponential phenomenon with age-dependent acceleration.
Hepatitis B virus, Fibrosis, Cirrhosis, Hepatocellular carcinoma, Contamination
The viral hepatitis pandemic is weighing heavily on human lives, populations and health systems. World Health Organisation (WHO) estimates that in 2015, 257 million people were living with chronic hepatitis B infection (defined as hepatitis B surface antigen positive) and hepatitis B resulted in an estimated 887 000 deaths, mostly from cirrhosis and hepatocellular carcinoma [1].
Viral hepatitis B is a debilitating disease (cirrhosis and hepatocellular carcinoma). It has been a notifiable disease since 1990 (Order 179/MS of 17 November 1990 setting out the list of notifiable diseases and notification procedures) and occupational, indemnifiable and listed in the table under number 45. The cost of treatment is high and complex.
Algeria is a country of average endemicity for HBV, its prevalence is estimated at 2.15% in the general population (86,000 Ag HBs positive out of 40 million inhabitants or 215 cas/100,000 inhabitants) according to a national seroprevalence study that dates back to 1998 involving a sample of 8126 people [2]. According to the National Blood Agency, the prevalence of HBs Ag among blood donors was 1.09 in 2007 [3]. The extent of the problem of viral hepatitis B stems not only from its frequency, but also from its short- and long-term health impact due to their evolutionary potential and therefore their complications. A better understanding of the analytical epidemiology of viral hepatitis B will help to better elucidate the profile of a target population for screening specific to our western Algerian region. Predictive modeling is a useful approach when there is insufficient data available. It contributes to a better understanding of the mechanisms of transmission, an earlier alert to the risk factors associated with viral hepatitis B.
Identify and estimate the effect of the main prognostic factors associated with the progression of liver fibrosis by the Cox model.
This is a descriptive and analytical cross-sectional study. The study population was comprehensively collected at the gastroenterology department of the Oran University Hospital. Information on patients with viral hepatitis B was collected prospectively from 2013 to 2016.
Were included in our study, all patients with:
◾ A chronic portage of the Ag HBs
◾ With or without histological damage to the liver.
Were excluded from the study population, with subjects presenting:
◾ Co-infections with HIV and/or HBV-HCV co-infections
◾ Non-viral hepatitis
◾ Other viral hepatitis A, C, D or E
◾ NCEP ATP III was used to define metabolic syndrome.
Data are collected on standardized sheets compiled from a questionnaire and then entered on standardized sheets with information on the different variables of the study, and used as a support for the processing and subsequent exploitation of the results.
Descriptive and analytical analysis of the data was done using SPSS20 software.
The tests used are: the Pearson 2 test for statistical association research between two qualitative variables, the Sudent's test for two independent samples and the variance analysis (ANOVA) were used for the comparison of continuous variables. A relationship is considered significant if the threshold was p < 0.05. Cox's model, or "proportional risk semi-parametric continuous model," is a continuous-time regression model. The goal is to model the instant risk logarithm based on a set of x explanatory variables that may vary in value over time. Cox regression predictive modeling is the model for estimating from our observations the effect of a variable on the occurrence of complications such as cirrhosis, hepatocellular carcinoma or death, after adjusting to other explanatory variables. This is a multiplicative risk model, the presence of an identified factor increases the risk of complication occurrence according to an estimated regression coefficient (Hazard ratio).
The viral hepatitis B study involved 271 patients during the study period (2013-2016) with a male predominance (Sex-Ratio of 1.22, which corresponds to 5 men for 4 women) (Table 1). At the professional level, more than half of hepatitic subjects B are active with a frequency of 59.0% and a clear male predominance (sex ratio-2.14 which means 214 men per 100 women; p < 0.0001). Alcoholism is noted in 3.3% of cases. Among all patients with viral hepatitis B, 20 subjects in occupations at risk of viral infection B are reported at 7.4%. Half of these high-risk cases are represented by the paramedics. The other half is shared equally between the medical and security forces, including 4 police officers and a gendarme. More than half of the population gathered is young (51.3%) between the ages of 20 and 39 (Figure 1) with an average age of 40.8 ± 15.3 years with no statistically significant difference between the two sexes (p = 0.23) and a median of 37.0 years. The age distribution of hepatitic patients B shows a modal class between 30 and 39 years. Half of the cases are in the 20-39 age group.
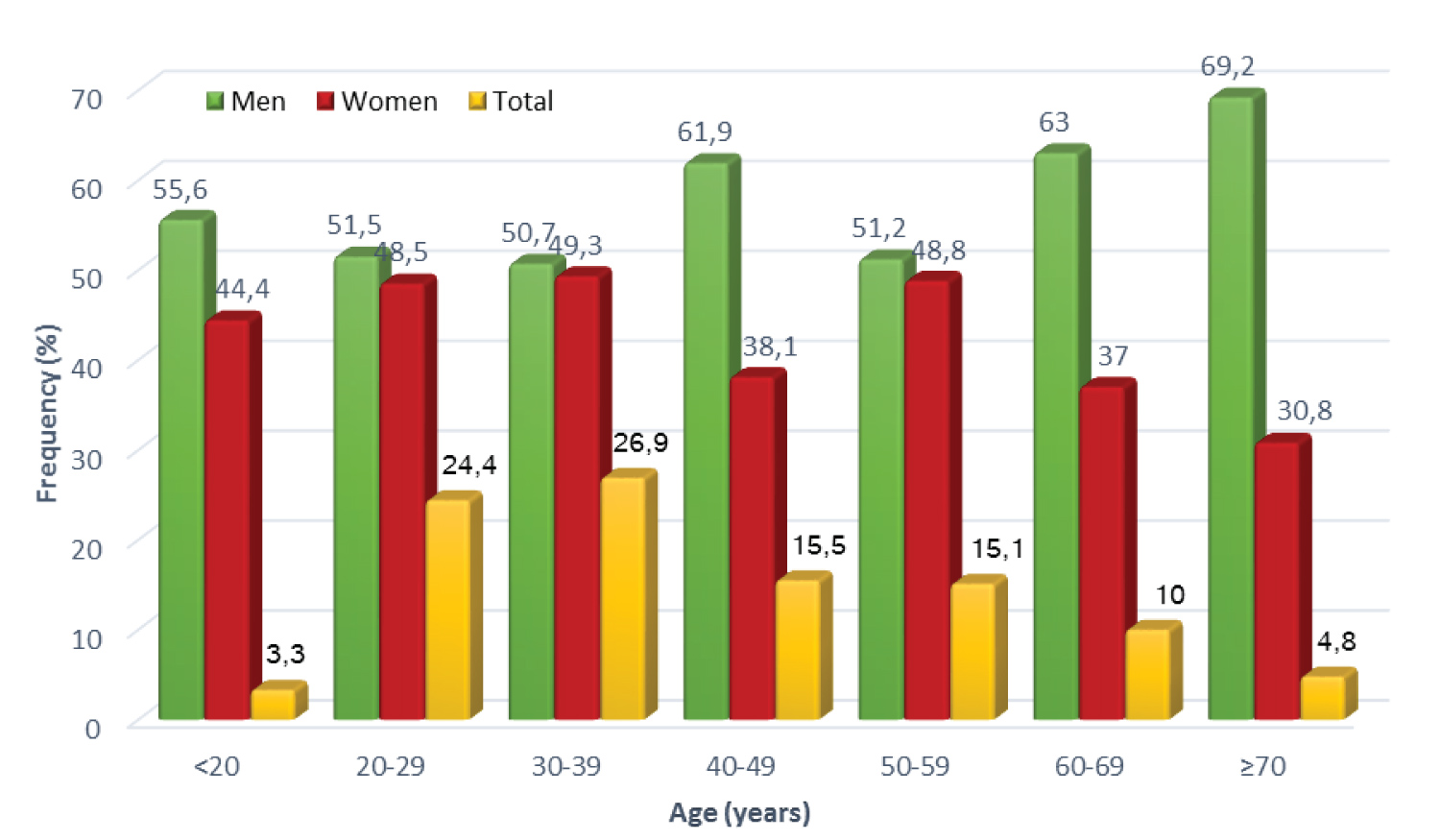 Figure 1: Distribution of Viral Hepatitis B Cases by Age and Sex.
View Figure 1
Figure 1: Distribution of Viral Hepatitis B Cases by Age and Sex.
View Figure 1
Table 1: Characteristics of Viral Hepatitis B Cases. View Table 1
In our study population, cirrhosis is diagnosed in 14.8% of cases of which 50% are over 54.5 years old with a clear male predominance (sex ratio = 2.3). A quarter of cirrhotics are diabetic. Metabolic factors are found in 15.0% of cirrhotic cases. Care-related contamination is the most common mode found in cirrhotic subjects in 82.5%. Traditional practices such as scarification, hijama and tattooing were reported in only 17.5% of subjects with advanced fibrosis F4 (Table 2).
Table 2: Characteristics of VHB Cirrhotics. View Table 2
Care-related contamination is the most common mode found in cirrhotic subjects in 82.5% multiplying the risk of developing cirrhosis at 2.4 times, predominated by dental care in 70.0% of cases (Table 3). Contamination during blood transfusion is present in a quarter (25.0%) cirrhotics thus multiplying the risk of developing cirrhosis by 4. Traditional practices such as scarification, hijama and tattooing were only reported in 17.5% of subjects with advanced fibrosis F4, their presence multiplied the risk by 3.
Table 3: Distribution of VHB Cirrhotics (N = 40) based on likely patterns of contamination. View Table 3
Hepatocellular carcinoma (HCC) developed in 6 male subjects, half of whom were in the advanced fibrosis stage F3-F4 and the other half with unidentified fibrosis (Table 4). The mode of care-related contamination is reported in 66.7% of carcinomatous and 33.3% are related to traditional practices. The causes of axtra-hepatic death are dominated by haemorrhage and other malignant tumours with frequencies of 1.9% and 1.2% of all VHB cases, respectively.
Table 4: VHB Patient Characteristics by Morbi-mortality. View Table 4
According to Cox's regression, the progression of the stages of fibrosis to cirrhosis is earlier in men than in women with an increasing probability from 50 years (Figure 2).
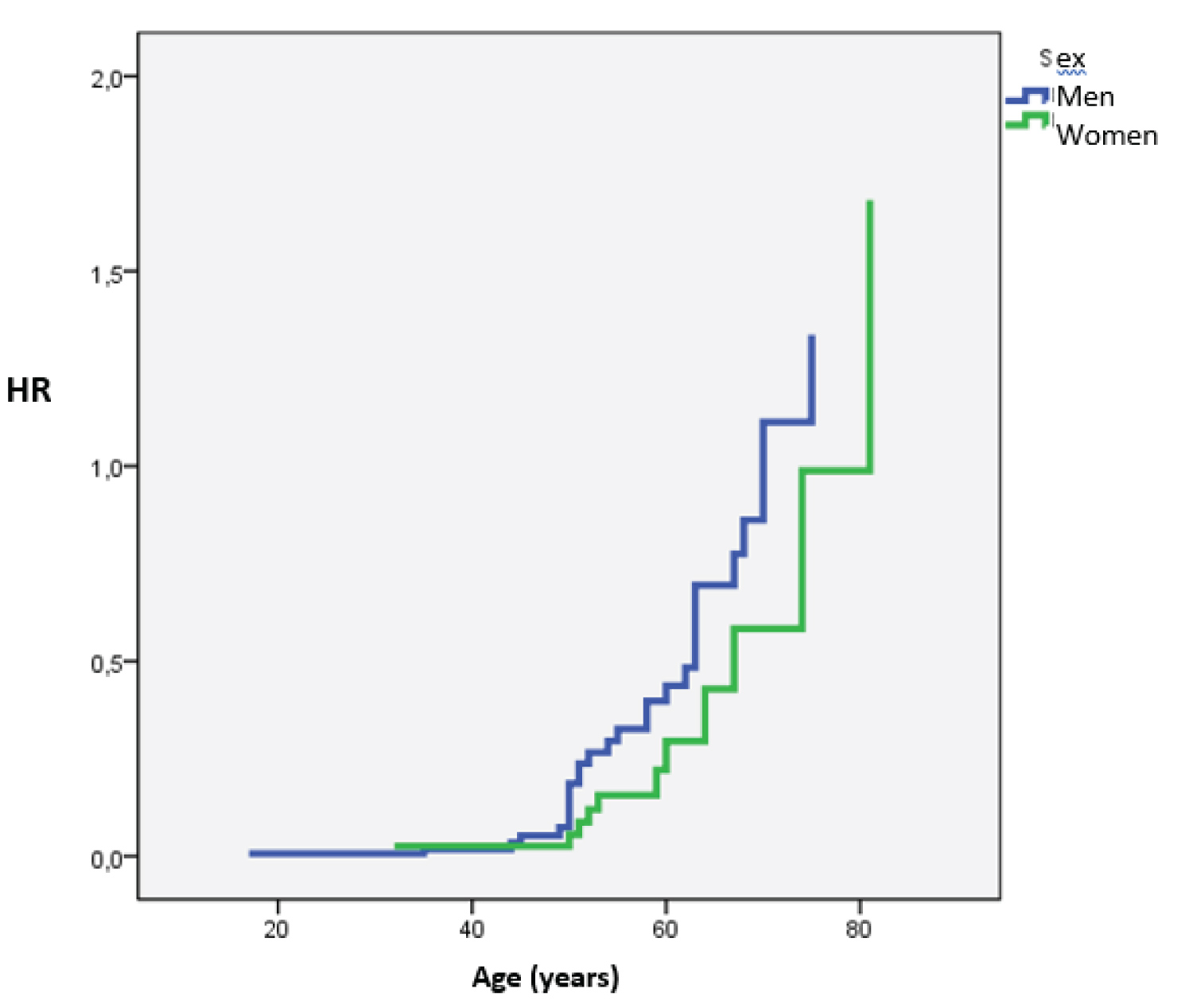 Figure 2: Risk of cirrhosis in HVB cases by sex.
View Figure 2
Figure 2: Risk of cirrhosis in HVB cases by sex.
View Figure 2
According to Cox's regression, the progression of the stages of fibrosis to cirrhosis is earlier in subjects positive to HBeAg with an instantaneous risk increasing from 25 years of age (Figure 3).
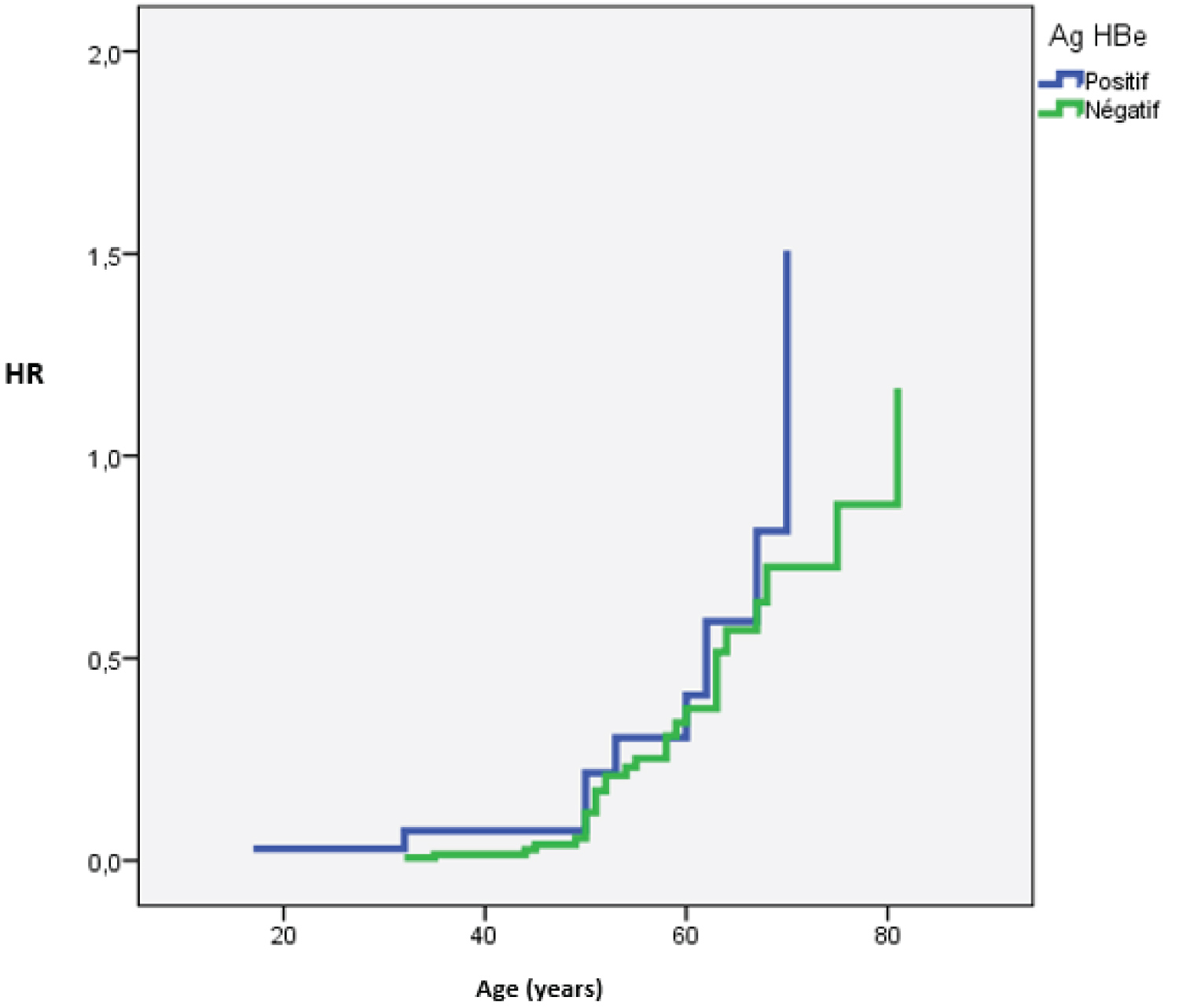 Figure 3: Risk of cirrhosis in cases of HVB according to HBeAg status.
View Figure 3
Figure 3: Risk of cirrhosis in cases of HVB according to HBeAg status.
View Figure 3
Cox's model identifies age as a prognostic factor associated with the onset of cirrhosis in VHB patients (Figure 4). The Instant Risk Report (HR) represents the gradual increase in the risk of cirrhosis in VHBs. In our study, the HR of age represents the gradual increase in the risk of cirrhosis in each unit of age increase, i.e. HR 1.05 increases by 5% for a one-year increase. For subjects aged 37 and over, HR is 12.34 with an IC95% confidence interval [4.29 - 35.52] and a p < 0.0001 which means that for an age ≥ 37 years, the instantaneous risk of developing cirrhosis is multiplied by 12 (Table 5). The model identifies other prognostic factors for the onset of cirrhosis:
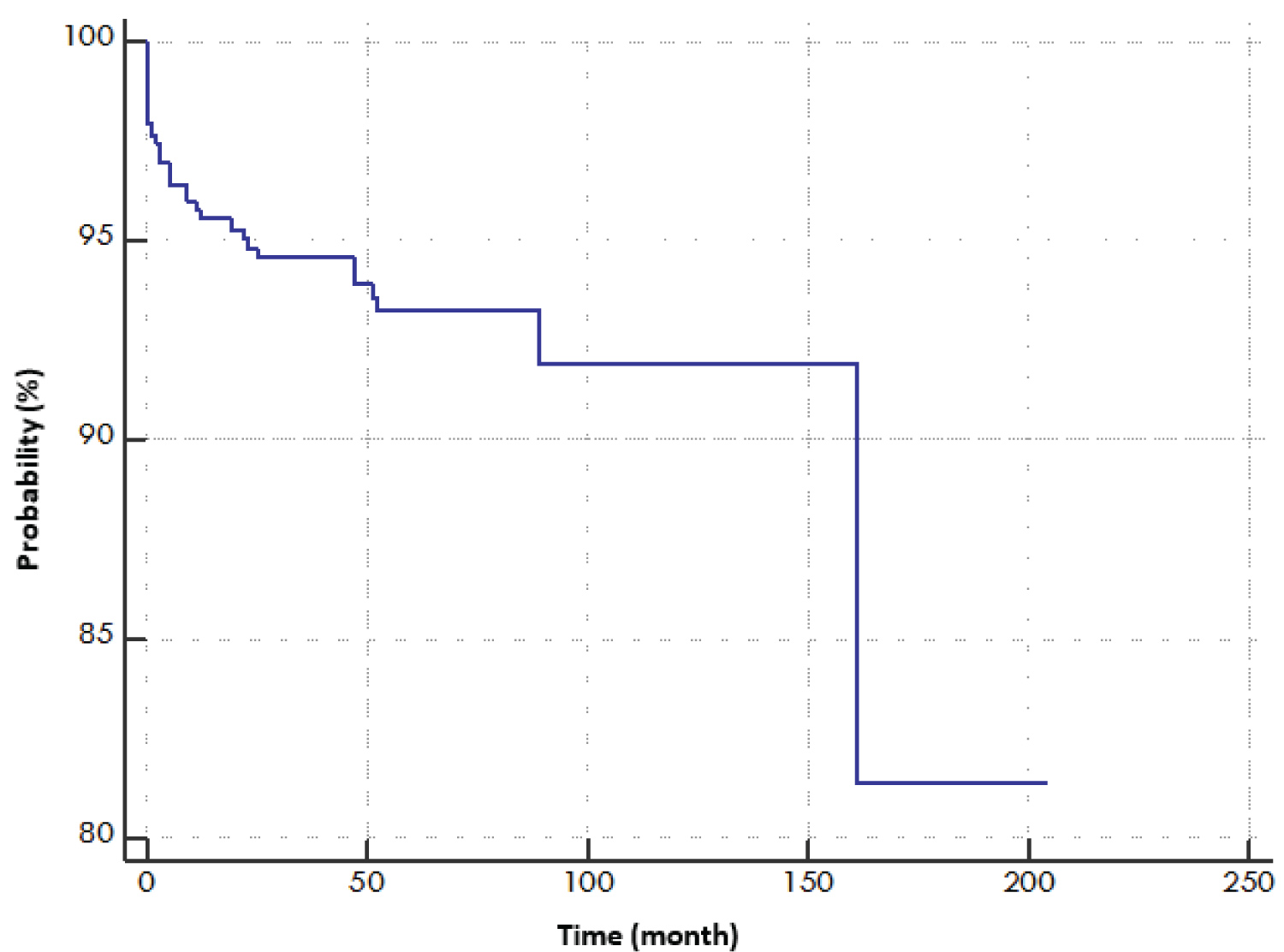 Figure 4: Probability curve of cirrhosis in VHB cases using Cox's model.
View Figure 4
Figure 4: Probability curve of cirrhosis in VHB cases using Cox's model.
View Figure 4
Table 5: Covariables included in Cox's Model: Stepwise Procedure. View Table 5
- Viral load > 20000 UI/ml multiplies the risk by 4.6.
- The negative sustained virological response multiplies the risk by 2.3.
For a subject i, if we introduce the 6 variables into the model, the function of instantaneous risk is such that:
The ROC curve (Figure 5) helps us make a decision to determine the threshold (inflection point) of the values of the "age" variable, which in this case is estimated at 48 years, from which the risk of cirrhosis is at most. This finding is illustrated in the dot diagram (Figure 6) which shows that from this age (48 years), the risk of cirrhosis is increased. The test shows a statically significant ROC curve with a p < 0.0001. The negative likelihood ratio is very low (0.2) confirming the acru risk of cirrhosis in patients with VHB from 48 years of age.
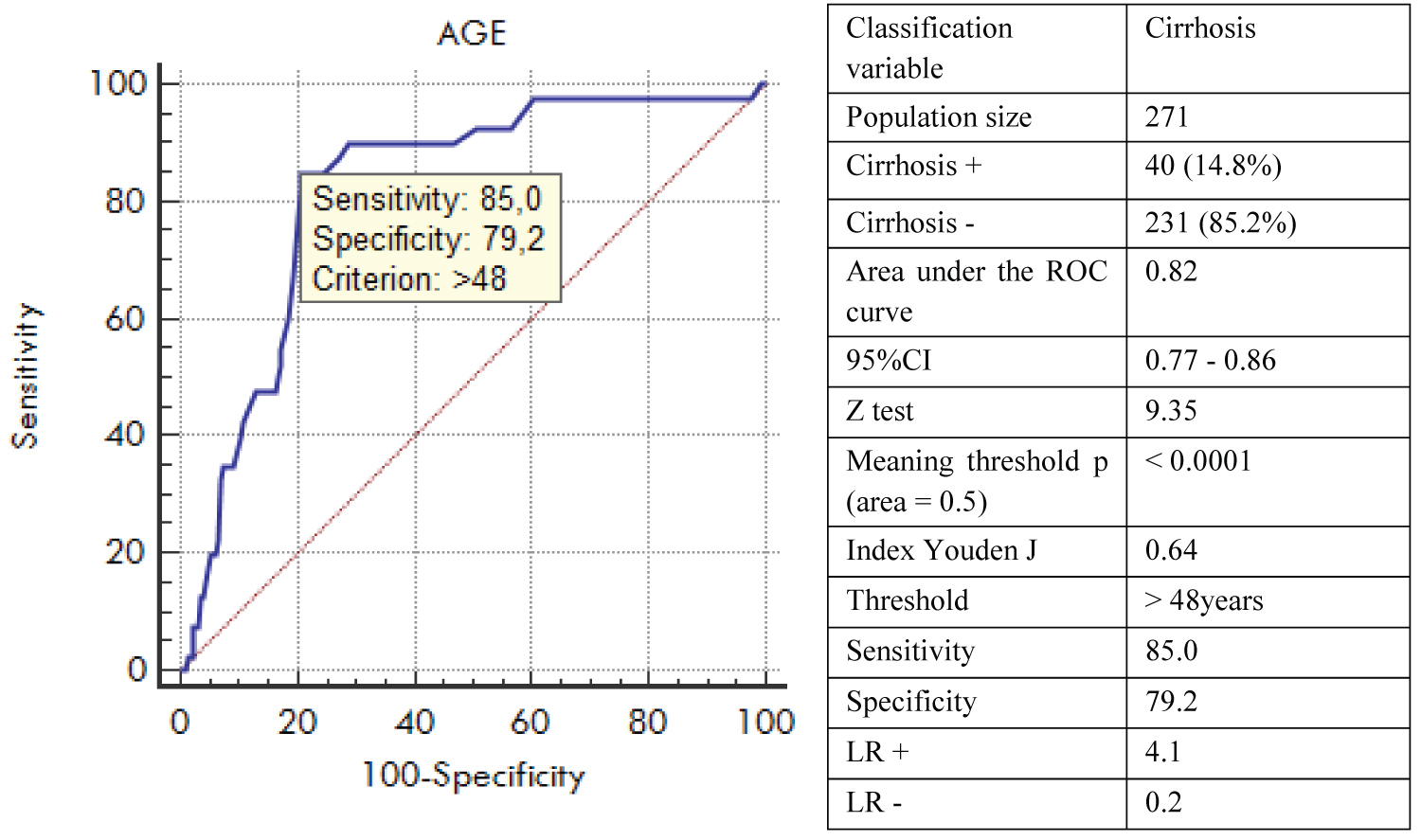 Figure 5: Age and Cirrhosis ROC Curve in VHB patients.
View Figure 5
Figure 5: Age and Cirrhosis ROC Curve in VHB patients.
View Figure 5
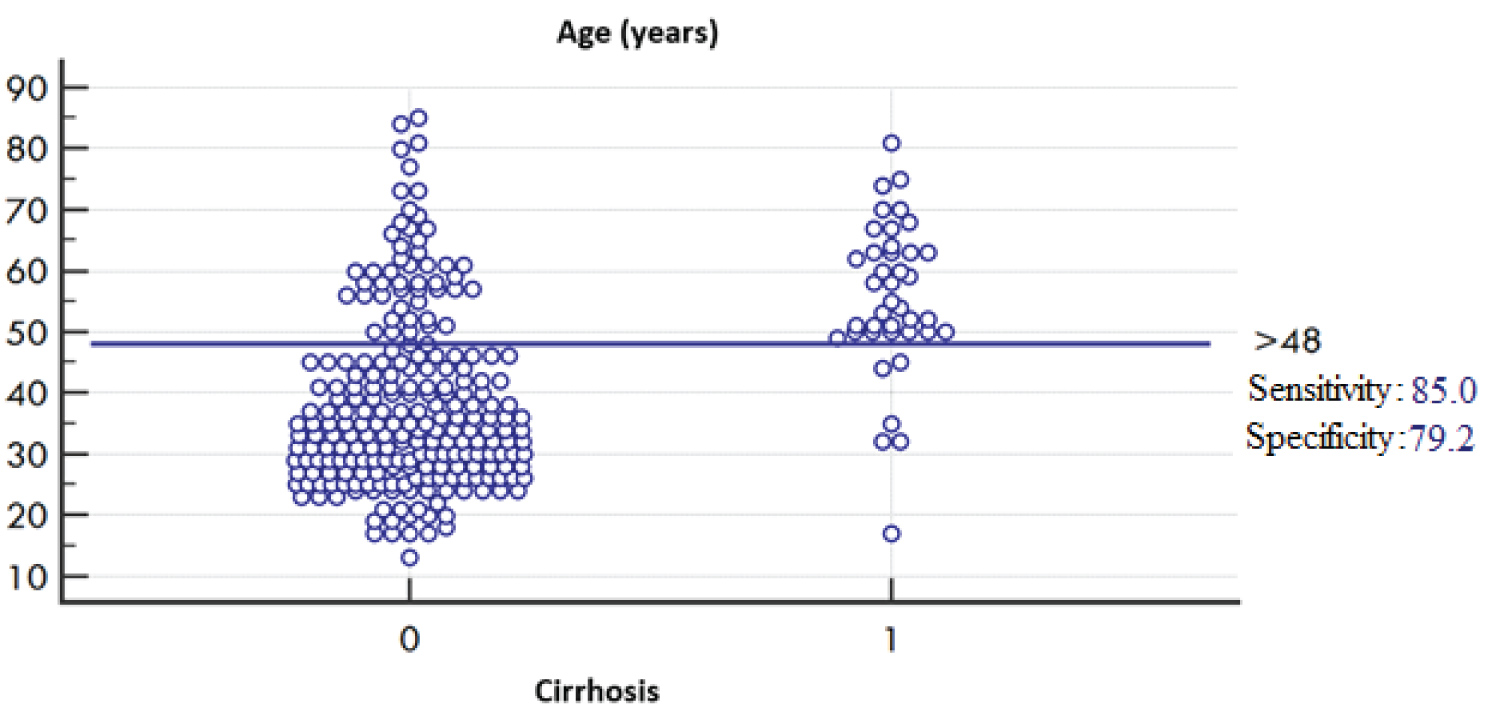 Figure 6: Interactive points diagram of age and cirrhosis in VHB patients.
View Figure 6
Figure 6: Interactive points diagram of age and cirrhosis in VHB patients.
View Figure 6
For the predictive modelling study of the occurrence of HCC in patients with viral hepatitis B and among the variables likely to be integrated into the model by the Stepwise procedure, only one variable was included being very strongly associated with the occurrence of HCC for hepatitic patients B (Figure 7), and that is:
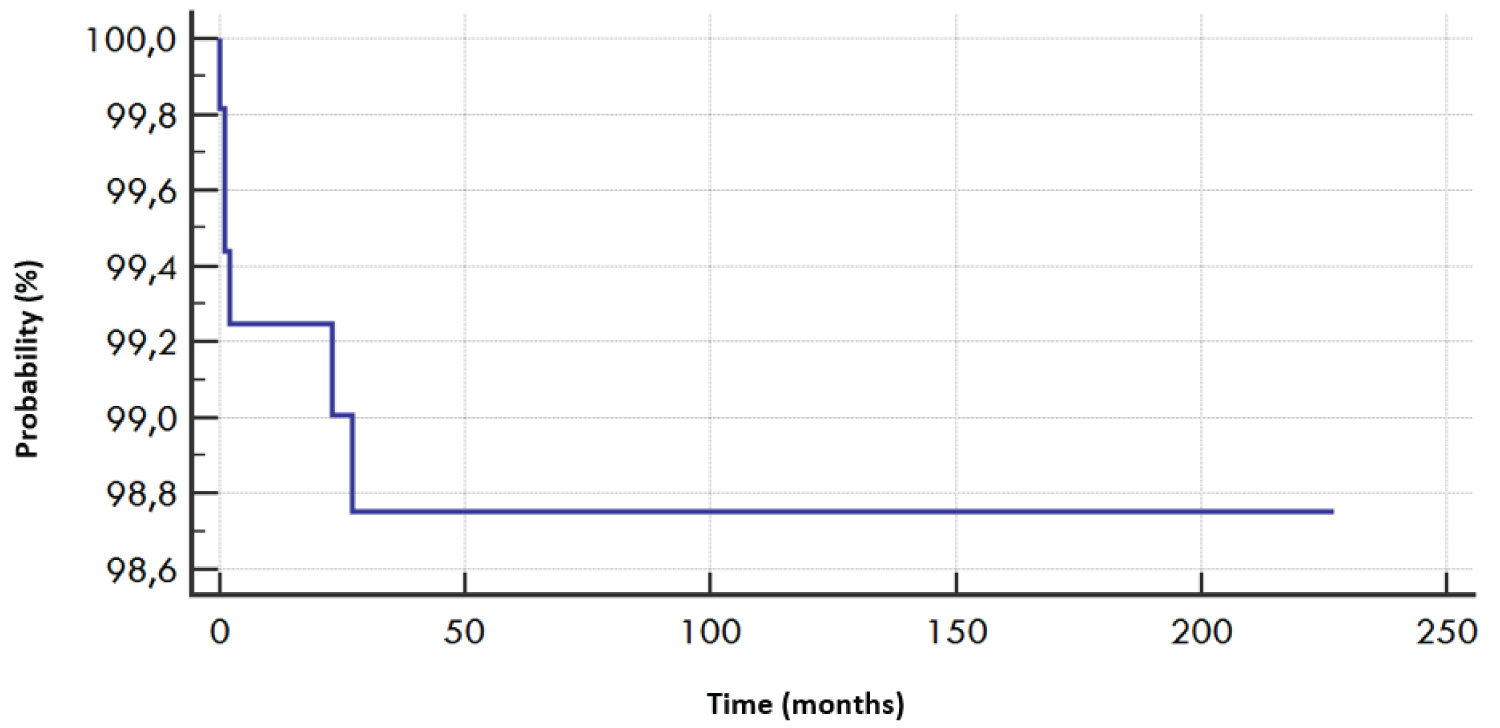 Figure 7: HCC Probability Curve in VHB Cases under Cox Model.
View Figure 7
Figure 7: HCC Probability Curve in VHB Cases under Cox Model.
View Figure 7
- Age increases the risk of HCC developing by 6% per unit increase (one year).
The presence of Ac anti-HBe would play a role in reducing the instantaneous risk of HCC occurrence quantified as follows: 1-0.1 = 0.9. So this reduction is estimated at 90%.
|
Covariable |
b |
SE |
Wald |
p |
HR |
95% CI HR |
|
Age (years) |
0.05380 |
0.02320 |
5.3788 |
0.0204 |
1.06 |
[1.01 - 1.10] |
|
Ac anti-HBe (+) |
-2.3391 |
1.1179 |
4.3783 |
0.0364 |
0.1 |
[0.01 - 0.9] |
For a subject i, if we introduce the variable into the model, the function of instantaneous risk is such that:
The inflection point of the ROC curve (Figure 8) is estimated at 44 years, from which the risk of HCC is at most. This result is illustrated in the dot diagram (Figure 9) which shows that all HCC cases are over 44 years old. The test shows a statically significant ROC curve with a p < 0.0001. The negative likelihood ratio is zero since the risk of HCC in our population of patients with VHB occurs from 44 years of age.
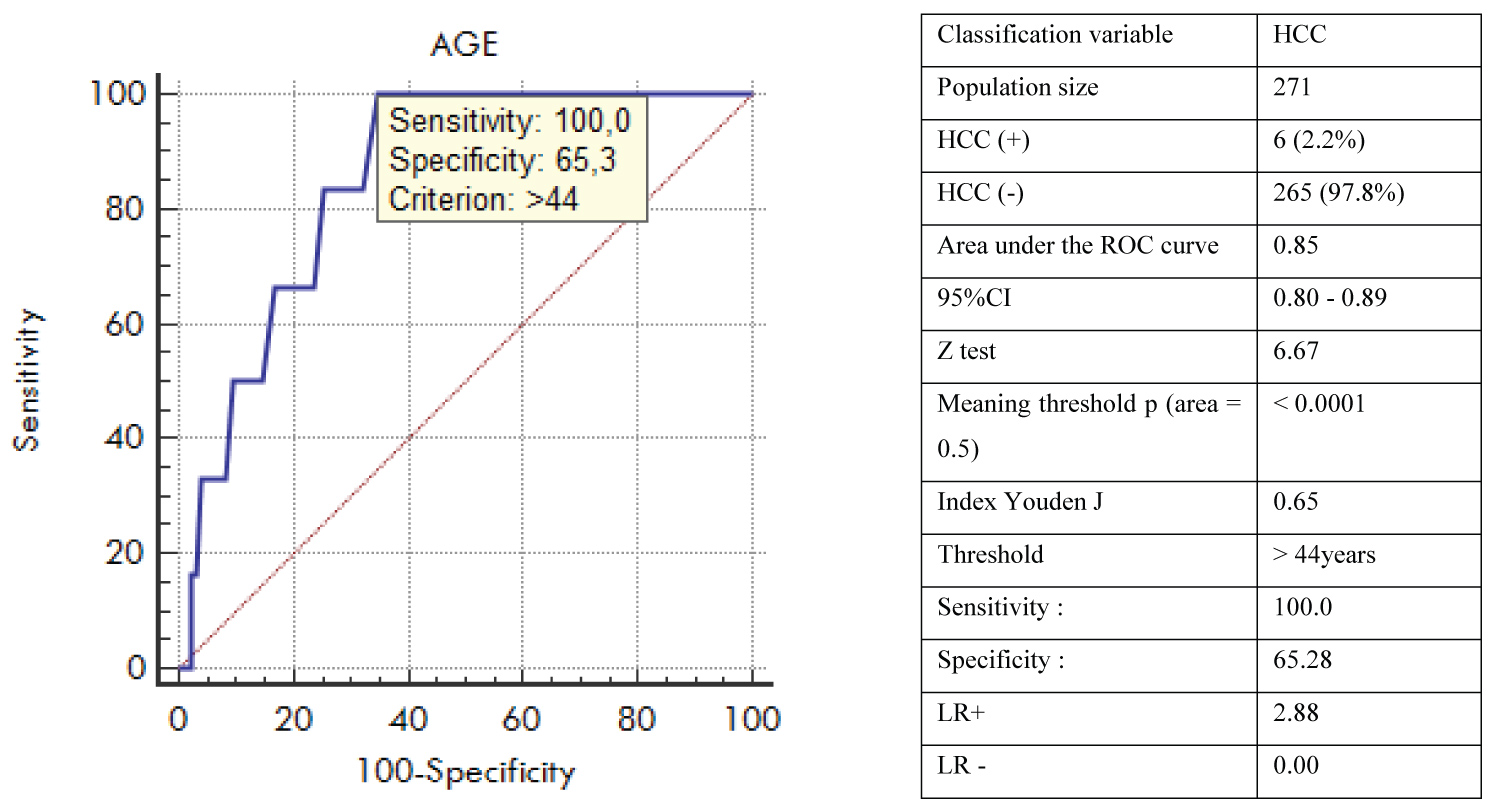 Figure 8: Age and HCC ROC Curve in VHB patients.
View Figure 8
Figure 8: Age and HCC ROC Curve in VHB patients.
View Figure 8
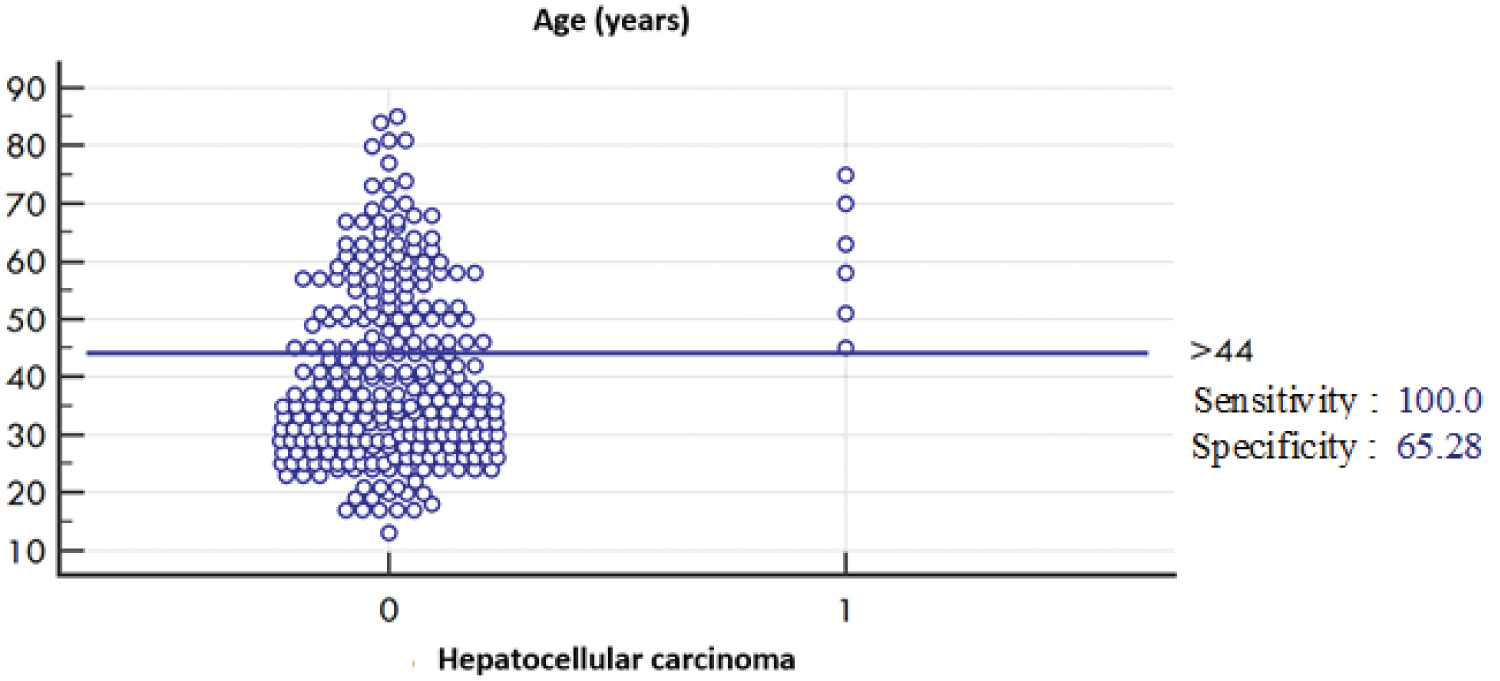 Figure 9: Interactive Age and HCC Chart in VHB Patients.
View Figure 9
Figure 9: Interactive Age and HCC Chart in VHB Patients.
View Figure 9
For the predictive mortality modelling study and among the variables likely to be incorporated into the model by the Stepwise procedure, two variables were included being very strongly associated with the occurrence of death for hepatitic B patients (Figure 10), which are:
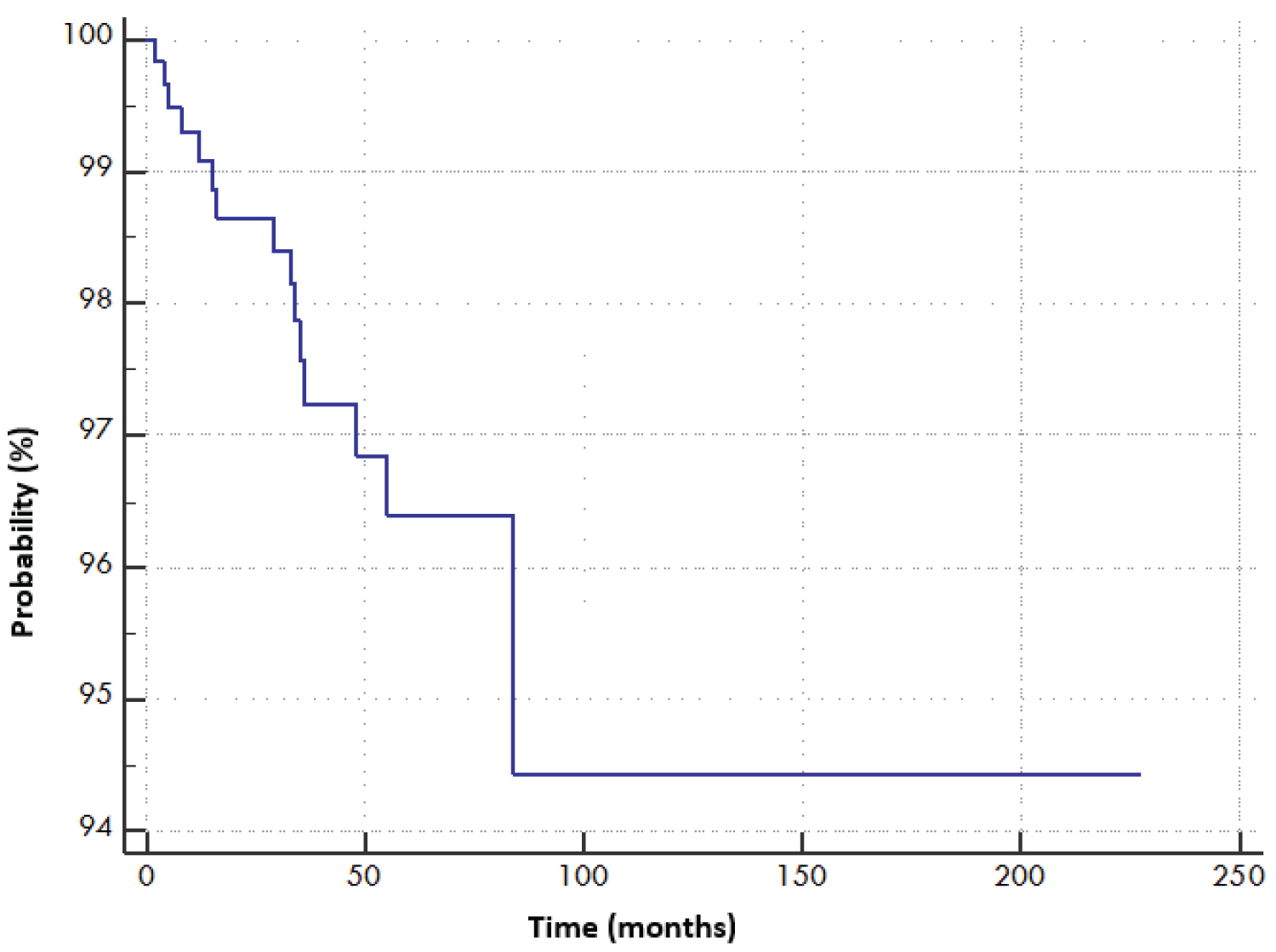 Figure 10: VHB Survival Curve according to Cox's Model.
View Figure 10
Figure 10: VHB Survival Curve according to Cox's Model.
View Figure 10
- The development of a HCC in an HVB patient means that death is almost certain.
- A positive HBeAg multiplies the instantaneous risk of survenue of death by 5.5.
|
Covariable |
b |
SE |
Wald |
p |
HR |
95% CI HR |
|
HBeAg + |
1.6973 |
0.5474 |
9.6150 |
0.0019 |
5.5 |
[1.9 - 15.9] |
|
Hepatocellular carcinoma |
3.2446 |
0.6909 |
22.0566 |
< 0.0001 |
25.7 |
[6.7 - 98.7] |
For a subject i, if we introduce the 2 variables into the model, the function of instantaneous risk is such that:
The results obtained in this study will give us the latitude to discuss epidemiological data on hepatitis B to better identify patterns of contamination and especially transmission in order to establish a profile of genotype distribution that prevails in our region and country. Predictive modeling explaining the risk of complication occurrence has identified several factors such as age, anemia, viremia, and some traditional practices. In our study population of 271 patients with HVB, there is a clear male predominance with a sex ratio of 1.22, which is consistent with all national and international studies. In Western Algeria, a sex ratio of 1.07 is reported in a 2015 study conducted by L. Mallem in Oran on a series of 151 cases [3]. Another study carried out in the centre of our country, on a series of 126 patients in Algiers in 2003 by S. Berkane reports a sex ratio of 2.07 [4].
In Tlemcen, retrospective work conducted by the epidemiology department from 2001 to 2009 found a sex ratio of 3.33 out of a population of 104 patients [5]. The same was true in a study conducted in the east of the country by S. Khelifa, which found a sex ratio of 1.7 [6]. In the Maghreb, this male predominance was also found by Benalaya [7] in Tunisia and Kitab [8] and Sbai [9] in Morocco with sex ratios of 2.48, 1.97 and 1.35 respectively.
In Europe, epidemiological data showed a male predominance in France (2008-2012) of 59% [10], in the United Kingdom by 60.9% [11] and in Italy by 76.2% [12]. Our HVB study population is young in 51.3% of cases, between 20 and 39 years with an average age of 40.8 ± 15.3 years without statistically significant difference between the two sexes. This early-age characteristic is also found in other Algerian studies previously cited, 35 years in the east, 39 years in Oran, 37 years in the center of the country. In Tlemcen, the population was older (46 years). Given the association of several likely modes of contamination in the same patient, an effective mode of transmission cannot be prejudged. Care-related contamination of all genders is predominant at 68.6%. Our results are in line with the Mallem and Berkane study of the majority mode of dental care. Surgery-related contamination (25.1%) is close to Berkane's in 2011 (26%) [13] compared to only 14.1% in the Mallem study.
In France, thanks to the viral genomic diagnosis B introduced since 2010 in blood donors, the risk of transfusion has increased from one infected donation /400000 donations between 2000-2002, to 1 infected donation out of 3 million donations in 2012. This reduced the risk of false negative results from the serological window. Care-related contamination affects all age groups, while it is in the adult population aged 20 and over that the use of traditional practices is reported. Hepatic cirrhosis was diagnosed in 14.8% of our series, half of whom are over 54.5 years old with a clear male predominance. Metabolic factors are found in 15% of cirrhotics compared to 0.9% in others (p < 0.001).
Cirrhosis is statistically linked to several likely modes of contamination. The risk of developing advanced fibrosis F4 is multiplied by 2.4, of which contamination during a blood transfusion multiplies it to 4. The use of traditional practices has a part to do with the risk of developing cirrhosis (OR = 2.7) whose tattoo multiplies it to 6.2.
The Cox model remains the most widely used model in biostatistics and in the medical field. It is used in the case of data for which the follow-up time varies according to the subjects but if the follow-up is fixed with no censored data, the logistic regression model is also suitable although Cox's model.
Viral hepatitis B is therefore a public health problem in our country. The epidemiology of this condition appears to be different in this country, and our results could lead us to think about new approaches to screening in our population that would have a very cost-effective economic impact given the very high cost of treatment. Our study showed that the target population for screening can be made up of the subjects: Male sex, Married, 3rd decade of life, Prison stay, Use of traditional practices, Care (dental, transfusion, surgery, ...). Continued epidemiological research into the natural history of these conditions must remain a public health priority in our country as the future increase in morbi-mortality associated with viral infection B would be associated with higher economic costs to our health system.
None declared.