The odontogenic keratocyst (OKC) is a benign pathology that presents characteristics of aggression and local recurrence. The WHO considered it as an odontogenic tumor in 2005, but in the most recent classification in 2017 it was once again considered as an odontogenic developmental cyst. Most of the time it presents a symptomatically, but the patient can report the pain symptomatology. The aim of this article is to report a clinical case of OKC on maxilla describing its characteristics and forms of treatment. Male patient, 15-years-old, referred to the bucomaxillofacial surgery service of Hospital do Oeste/Barreiras/BA complaining of increased volume in the maxillary region, diagnosed as possible cyst on routine panoramic radiography. A multi-slice computed tomography was performed, in which a multilocular radiolucent image was observed in the right maxilla. Histopathology confirmed to bean OKC. Surgical treatment was performed with curettage and patient's follow-up. OKC is a very common lesion in the literature, because of this it is very important to know the clinical, radiographic and histopathological characteristics, as well as professional experience, for diagnostic and therapeutic closure for this pathology.
Odontogeniccyst, Keratocysts, Diagnosis
The odontogenic keratocyst (OKC) is a developmental odontogenic cyst that shows local aggressiveness and high relapse rate [1-7]. Due to these characteristics, in 2005 the WHO classified it as an odontogenic keratocyst tumor [3,5,8]. However, the most recent classification, which was published in 2017, considered it as a developmental odontogenic cyst again [4].
Clinically, OKC presents itself asymptomatically, usually with a medullary growth pattern, which causes minimal expansion of the cortical bone, but sometimes it may be related to pain and aggressive growth. It mainly affects posterior region of mandible with common involvement of mandibular angle and third molar [2,3,5-7] and has predilection for male gender [5]. Radiographically, it appears as a well-defined radiolucent area, presenting marginal delimitation, which can be uni or multilocular [2,3,5,7,9]. The multilocular form resembles ameloblastoma, especially when it affects the mandible. Also, it may or may not be associated with an included tooth, which can sometimes be confused with dentigerous cyst [2,3,5,7]. There are two theories in literature that explains the keratocyst etiology. One of them says that the keratocyst etiology is from the remnants of dental lamina [2,5,6]. The other theory describes its origin through the basal cells proliferation of an epithelium [6]. Histologically, OKC has a stratified squamous epithelium composed of 6 to 10 cells. The cells of the basal layer of this epithelium most often appear hyper-stained and arranged in a stockade pattern [6,9]. The interface between epithelium and connective tissue is usually flat and the keratin of the most superficial layer is parakeratinized and presented in a corrugated shape [2,5,6,9]. The indicated treatment is enucleation and curettage, but clinical resection is necessary in some cases [1,5,6]. The aim of this paper is to report a case of maxillary OKC associated with tooth displacement on orbit floor in a 15-year-old boy describing its characteristics and treatment.
A 15-years-old, ASA 1, male patient, referred to the Bucomaxillofacial Surgery Service of the Hospital do Oeste/Barreiras/BA, complaining of increased volume in the maxillary region, diagnosed as possible cyst on routine panoramic radiography for orthodontic treatment (Figure 1 and Figure 2). A multi-slice computed tomography was performed where a radiolucent and multilocular (Figure 3) image was observed in the right maxilla, with tooth displacement in proximity to the floor of the right orbit. An incision al biopsy was performed, and it confirmed the OKC diagnosis.
 Figure 1: Preoperative images: A) Extra oral image evidencing volume increase in right hemiface, with discrete loss of nasolabial fold; B) Intraoral image showing discrete volume increase in vestibulare sulcus of right upper molar region.
View Figure 1
Figure 1: Preoperative images: A) Extra oral image evidencing volume increase in right hemiface, with discrete loss of nasolabial fold; B) Intraoral image showing discrete volume increase in vestibulare sulcus of right upper molar region.
View Figure 1
 Figure 2: Panoramic radiograph showing the presence of a tooth displaced to the orbital floor and presence of radiolucent lesion in the right maxilla.
View Figure 2
Figure 2: Panoramic radiograph showing the presence of a tooth displaced to the orbital floor and presence of radiolucent lesion in the right maxilla.
View Figure 2
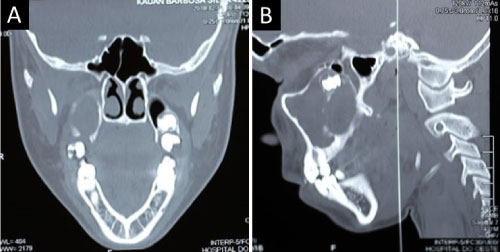 Figure 3: Computed tomography with multiple cuts, where a radiolucent and multilocular image was observed. A) Coronal section; B) Sagittal cut.
View Figure 3
Figure 3: Computed tomography with multiple cuts, where a radiolucent and multilocular image was observed. A) Coronal section; B) Sagittal cut.
View Figure 3
The patient underwent surgery under general anesthesia with access at the vestibule floor of the right maxilla. Maxillary osteotomy was performed at the maxillary sinus level to expose the lesion. After the curettage of the lesion, the tooth that had been moved to the orbital cavity was removed (Figure 4).
 Figure 4: Transoperative images: A) Access and exposure of the cystic lesion; B) Cavity after removal of the cystic capsule; C) The extracted tooth.
View Figure 4
Figure 4: Transoperative images: A) Access and exposure of the cystic lesion; B) Cavity after removal of the cystic capsule; C) The extracted tooth.
View Figure 4
Analgesic, non-steroidal anti-inflammatory and mouth wash with chlorhexidine were prescribed in the post-operative period.
After 7 post-operative days, the patient evolved with preserved visual acuity, post-operative compatible edema, and sutures in position without infection and/or dehiscence (Figure 5). After 1 postoperative month (Figure 6), he presented with no complaint sand with excellent evolution. The result of the excision al biopsy confirmed OKC diagnosis. Patient and his responsible person were oriented to maintain annual follow-up for 5 years, due to injury recurrence potential.
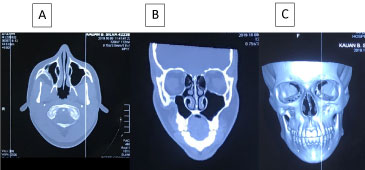 Figure 5: Postoperative computed tomography with multiple cuts. A) Axial cut; B) Coronal cut; C) 3D section.
View Figure 5
Figure 5: Postoperative computed tomography with multiple cuts. A) Axial cut; B) Coronal cut; C) 3D section.
View Figure 5
 Figure 6: Postoperative panoramic radiograph of control, 30 days after the removal of the lesion, showing discrete signs of ossification and absence of the unit in intimate communication with the floor of the right orbital cavity.
View Figure 6
Figure 6: Postoperative panoramic radiograph of control, 30 days after the removal of the lesion, showing discrete signs of ossification and absence of the unit in intimate communication with the floor of the right orbital cavity.
View Figure 6
OKC is a developmental odontogenic cyst that presents high index of reported cases in literature. It is considered as the second most common non-inflammatory cyst of development, second only to the dentigerous cyst that is the most prevalent [10,11].
Al though most cases indicate that OKC is more predominant in posterior region of the mandible [5,6], it is not discarded its existence in other regions such as in this case where the OKC was found in anterior region of maxilla. In relation to the gender, the present study corroborated with the study of Sousa, et al. [5], bringing the male gender as the most affected.
Most of reported cases in literature affirmed that OKC's presence is variable in relation to age, which can affect infants to older individuals. However, the highest prevalence is between the second and fifth decade of life [5,12] corroborating with this report.
Most of times OKC is discovered through routine radiological examination [5], due to its absence of symptoms. It was described in this report, which the patient was diagnosed in a panoramic radiograph to start orthodontic treatment. Nonetheless, in some cases OKC can be symptomatic and may cause tooth displacement, which corroborates with this study in which the tooth was moved to the right orbital floor.
The most used therapeutic forms to treat OKC are enucleation and curettage [1,5,6]. Because it has a thin and friable capsule, it is difficult to remove completely by enucleation, so an aggressive curettage was performed aiming to decrease a recurrence probability.
Sousa, et al. [5] and Boyne, et al. [13] in their study affirmed that in some cases are necessary auxiliary therapeutic techniques aiming to decrease those index assigning chemical and physical methods such as cryotherapy and the Carnoy solution that promote cellular and chemical necrosis, respectively, and may significantly decrease this recurrence.
Studies in the literature have shown that OKC can present recurrence in 5 years after the first therapy [12], but there are cases in which recurrence was evidenced even after 10 years of follow-up [12,14].
Balmic, et al. [15] showed in their studied cases and that had recurrence, an average time of 2.2 year after the initial treatment (ranging from 1 to 2.5 years). They justify that relapse is more related to the nature of the pathology than the chosen therapy [15].
The morphological findings are very important to the final diagnosis of the lesion [2,6,9]. Even though clinical and radiographic examinations are suggestive, they often present similarity other pathologies, which makes difficult the diagnosis. Thus, incisional biopsy is indispensable to surgical planning and diagnosis.
Although OKC is a lesion with high incidence in literature, it is clear that it may present variations on its clinical characteristics. The rare location of this case, in anterior region of maxilla causing tooth displacement to orbit floor, which is a few found in literature, is an example of that. This highlights the importance of joining the clinical, radiographic and histopathologic features for conclusive closure and establishment of apropriate therapy for the pathology.