Systemic sclerosis, Paraneoplastic, Malignancy
Malignant neoplasms have been associated with various paraneoplastic rheumatic syndromes [1]. These syndromes are rare manifestations of cancer resulting from an autoimmune response to cancer cells and can be linked to particular types of cancer, such as lung or breast cancer. They may also be present with a broad range of clinical features, including neurological, hematological, and rheumatological symptoms [2].
Paraneoplastic syndromes involving rheumatological disorders, such as systemic sclerosis, have been reported. While the exact mechanism behind paraneoplastic rheumatic syndromes is not fully understood, it has been hypothesized that there may be shared triggers between neoplasia and rheumatic disease, inflammation triggered by toxins produced by the tumor, hypersensitivity reactions against intracellular antigens eliminated by apoptotic cancer cells, or successful tumor immunosurveillance [3,4].
This case series reports two cases of paraneoplastic rheumatic syndrome of systemic sclerosis presentation and underscores the importance of early recognition and treatment of the underlying malignancy for the successful management of these conditions. To identify and manage paraneoplastic syndromes, it is critical that rheumatologists, oncologists, and primary care practitioners collaborate effectively.
The patient was a 63-year-old woman of Asian descent who was a non-smoker and non-alcoholic with underlying diabetes mellitus, hypertension, dyslipidemia, and hyperthyroidism. She worked as a chef and was on chronic prescriptions of the following medications: metformin 1g twice daily, biphasic insulin subcutaneous injection 20 units in the morning, then 14 units in the evening, perindopril 8 mg once daily, simvastatin 40 mg once daily and carbimazole 5 mg once daily. Her family history was notable for lymphoma and hepatocellular carcinoma among her first-degree relatives. She presented with a 3-month history of bilateral symmetrical polyarthritis involving small joints of both hands associated with progressive skin tightening of her hands and Raynaud's phenomenon. She also lost her appetite and weight. There were no respiratory symptoms. Physical examination revealed swollen and tender joints involving her right first to third metacarpophalangeal joints (MCPJ), left first to second MCPJ, and all proximal interphalangeal joints (PIPJ) of both hands (Figure 1a, Figure 1b and Figure 1c). Sclerodactyly of fingers and both hands were observed extending proximal to both elbows, with flexion deformities noted in both middle and ring fingers (Figure 1b and Figure 1c). The calculated modified Rodnan Skin Score was 17. There were telangiectasias over the dorsum of her right hand. Raynaud's phenomenon was present over both hands. Lung auscultation disclosed diminished breath sounds at the lung bases. An enlarged right supraclavicular lymph node was palpable. Otherwise, there were no other significant physical findings on examination.
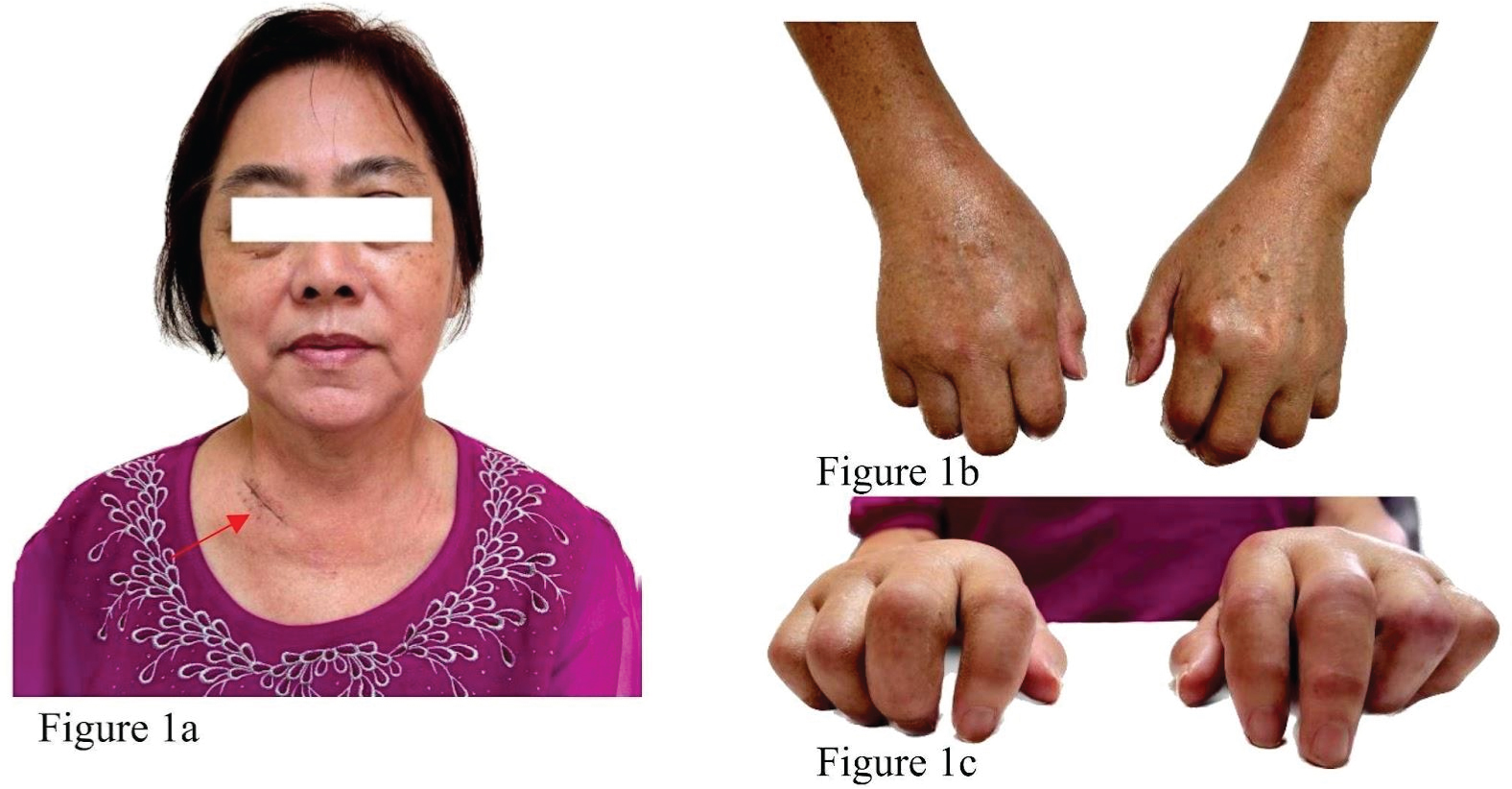 Figure 1: Patient No 1 with skin tightening of the face (a) and sclerodactyly (b) as well as polyarthritis of the MCP and PIPJ (c). Small telangiectasias were noted over the right-hand dorsum (Figure 1b). There is an incisional biopsy scar over the right supraclavicular lymph node (red arrow in Figure 1a).
View Figure 1
Figure 1: Patient No 1 with skin tightening of the face (a) and sclerodactyly (b) as well as polyarthritis of the MCP and PIPJ (c). Small telangiectasias were noted over the right-hand dorsum (Figure 1b). There is an incisional biopsy scar over the right supraclavicular lymph node (red arrow in Figure 1a).
View Figure 1
Laboratory results revealed a total white cell count of 11.8 × 10^3/uL and platelet count of 458 × 10^3/uL. The absolute eosinophil count of 300 cells per microliter was normal. Erythrocyte sedimentation rate (ESR) was raised at 41 mm/hr. Liver and renal function tests were unremarkable. Immunological workup was positive for anti-Ro-52 antibodies and antinuclear antibodies (ANA) at a titer of 1:1280 (nucleolar pattern). Anti-centromere and anti-topoisomerase I were negative, while Anti-RNA polymerase III was not available at our center. Musculoskeletal ultrasound demonstrated active synovitis with corresponding doppler activity (grade 3 synovitis and grade 3 doppler) and tenosynovitis of her right first to third MCPJ, left first to second MCPJ, and all the PIPJ of both hands. Capillaroscopy was not performed. Transthoracic echocardiography revealed no evidence of pulmonary hypertension. A chest radiography performed for the lungs auscultatory findings revealed a suspicious right lower lobe nodule (Figure 2a). Follow-up contrast-enhanced computed tomography of the thorax demonstrated a right lower lobe ill-defined heterogeneously enhancing lung mass measuring 2.2 × 4.6 × 2.4 cm with mediastinal and right supraclavicular lymphadenopathy (Figure 2b, Figure 2c and Figure 2d) as well as right pleural effusion. Right supraclavicular lymph node incisional biopsy was performed, and the histopathological examination revealed metastatic adenocarcinoma with immunohistochemistry studies suggesting a lung primary tumor (positive for CK7 and TTF-1, negative for CK20 and p40). Further testing for EGFR mutation and ALK was negative.
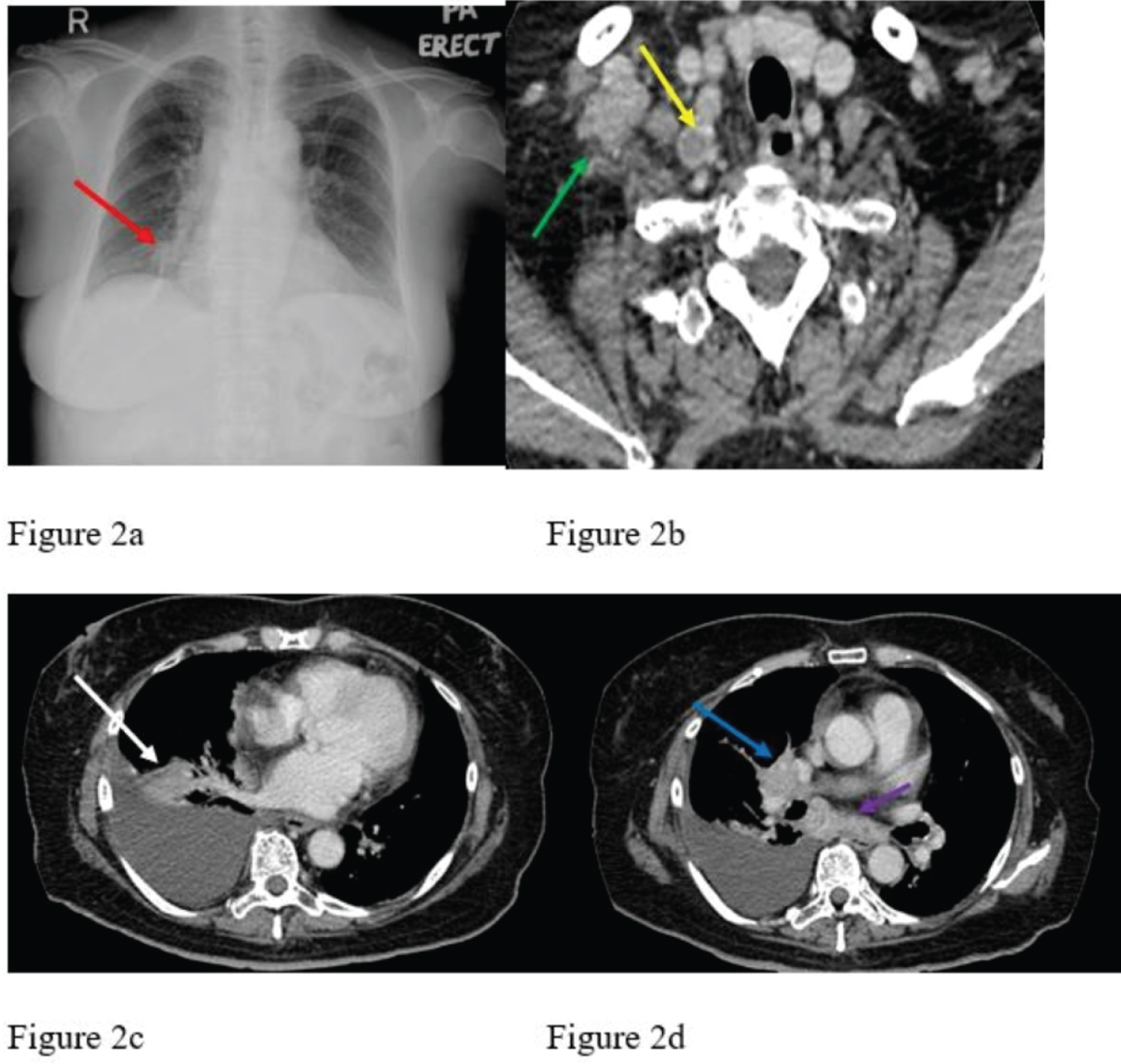 Figure 2: Initial chest radiograph (Figure 2a) revealed a suspicious right lower zone lung nodule (red arrow) adjacent to the right heart border. Subsequent contrast-enhanced computed tomography of the thorax confirmed the finding of a right lower lobe enhancing lung mass (white arrow in Figure 2c) as well as right pleural effusion with associated right hilar (blue arrow) as well as subcarinal lymphadenopathies (purple arrow) in Figure 2d. The image at the upper thoracic level (Figure 2b) also showed enlarged right supraclavicular lymph nodes, some with necrotic centers (green and yellow arrows).
View Figure 2
Figure 2: Initial chest radiograph (Figure 2a) revealed a suspicious right lower zone lung nodule (red arrow) adjacent to the right heart border. Subsequent contrast-enhanced computed tomography of the thorax confirmed the finding of a right lower lobe enhancing lung mass (white arrow in Figure 2c) as well as right pleural effusion with associated right hilar (blue arrow) as well as subcarinal lymphadenopathies (purple arrow) in Figure 2d. The image at the upper thoracic level (Figure 2b) also showed enlarged right supraclavicular lymph nodes, some with necrotic centers (green and yellow arrows).
View Figure 2
She was referred to the oncologist for further management of the lung malignancy and planned for gemcitabine and cisplatin chemotherapy. She fulfilled the 2013 American College of Rheumatology and European League against Rheumatism classification criteria for systemic sclerosis with a total score of 14 (Table 1). Hence, she was started on low-dose prednisolone to control her active arthritis and tenosynovitis without disease-modifying anti-rheumatic drugs.
Table 1: Scleroderma/systemic sclerosis (2013 EULAR/ACR Criteria). View Table 1
The patient was a 55-years-old woman of Asian descent who was a non-smoker and non-alcoholic with underlying ischemic heart disease, hypertension, diabetes mellitus, and dyslipidemia. Her usual medications consisted of isosorbide mononitrate 120 mg once daily, trimetazidine MR 35 mg twice daily, pantoprazole 40 mg once daily, atorvastatin 40 mg daily, perindopril 8 mg daily, metformin 1g twice daily and vildagliptin 50 mg once daily. There was a family history of colon cancer but none for blood malignancy. She presented with a 2-month history of generalized progressive skin tightening involving her chest, face, and peripheral limbs, Raynaud's phenomenon, weight loss and appetite, dry eyes, and dry mouth with difficulty swallowing. There was reduced effort tolerance with intermittent palpitation as well. She denied any joint pain or swelling and had no bleeding tendency. A general physical examination revealed a cachexic patient with pallor but no jaundice, lymphadenopathy, or hepatosplenomegaly. There was sclerodactyly of all her fingers and skin tightening of her hands (Figure 3b), sclerodermic facies with microstomia, and a beaked nose (Figure 3a). There was also skin thickening over her chest wall and both lower limbs (Figure 3c). The modified Rodnan skin thickness score was 29.
 Figure 3: Patient No 2 with shiny skin tightening of the face, microstomia, perioral furrowing, and beaked nose (Figure 3a). There are sclerodactyly (Figure 3b) and also skin tightening of bilateral lower limbs (Figure 3c).
View Figure 3
Figure 3: Patient No 2 with shiny skin tightening of the face, microstomia, perioral furrowing, and beaked nose (Figure 3a). There are sclerodactyly (Figure 3b) and also skin tightening of bilateral lower limbs (Figure 3c).
View Figure 3
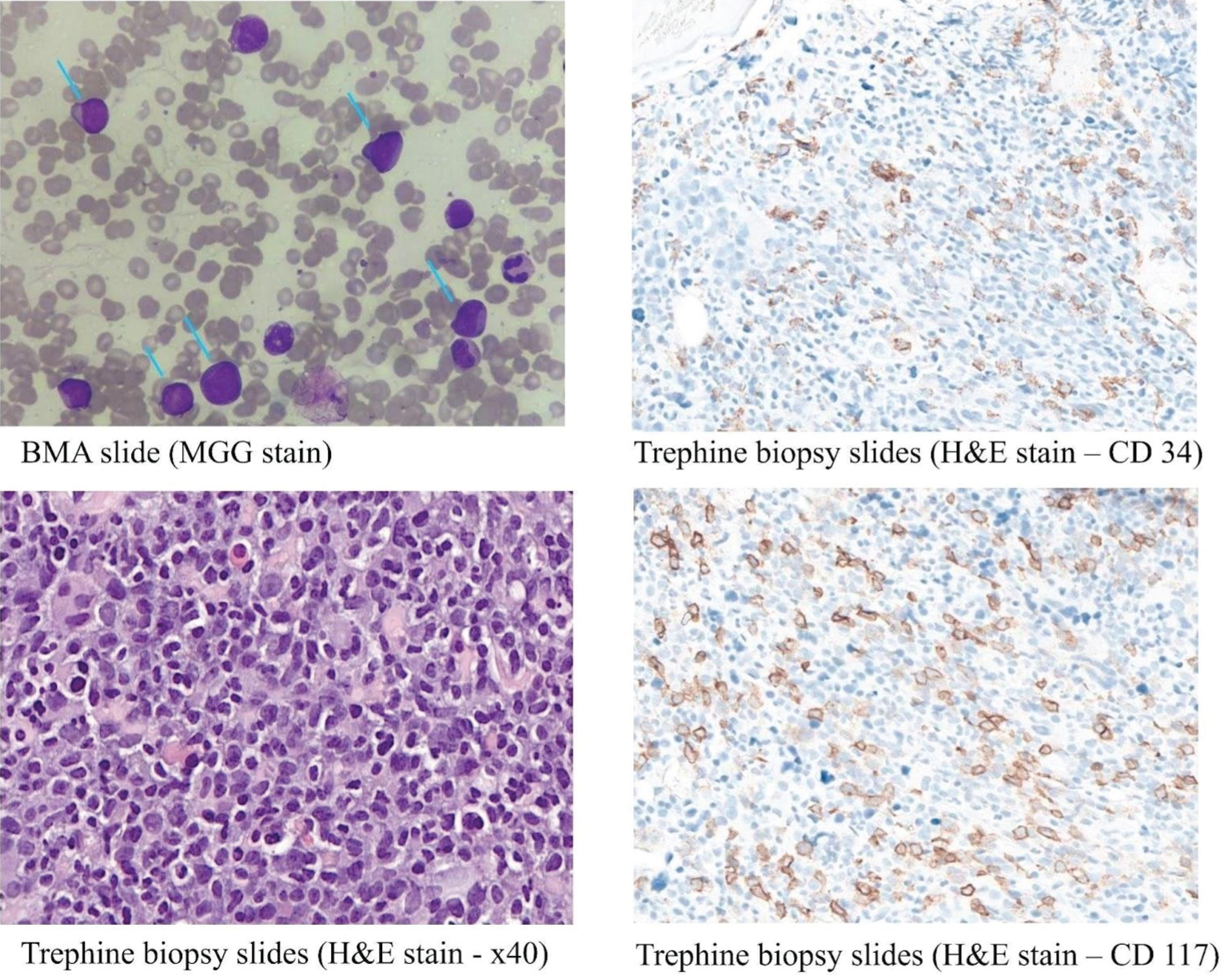 Figure 4: BMA slide (MGG stain) shows the presence of blast cells (blue arrow), which are small to medium in size, with round to oval nuclei, exhibit open chromatin pattern, prominent nucleoli, and scanty to moderate amount of cytoplasm. Trephine biopsy slides (H&E stain - x40; CD 117; CD 34) show the presence of many blast cells scattered singly and in small clusters throughout the marrow spaces. They are positive for CD34 and CD117.
View Figure 4
Figure 4: BMA slide (MGG stain) shows the presence of blast cells (blue arrow), which are small to medium in size, with round to oval nuclei, exhibit open chromatin pattern, prominent nucleoli, and scanty to moderate amount of cytoplasm. Trephine biopsy slides (H&E stain - x40; CD 117; CD 34) show the presence of many blast cells scattered singly and in small clusters throughout the marrow spaces. They are positive for CD34 and CD117.
View Figure 4
Her liver and renal function tests were unremarkable. Full blood count showed anemia with a hemoglobin level of 8.3 g/dL and thrombocytopenia with a platelet count of 54 × 10^3/uL. A subsequent full blood picture revealed the presence of 39% blast cells suspicious of acute myeloid leukemia (AML); no Auer rod was seen. An urgent bone marrow aspiration examination with immunophenotyping confirmed AML FAB classification M4. Further tests were negative for common leukemia translocations, FLT3, NPM1, and CEBPA mutations. Her autoimmune workups revealed a positive ANA with a titer of more than 200 and positive Anti-Ro-52 using chemiluminescent immunoassay. Anti-centromere and anti-topoisomerase I were negative, while Anti-RNA polymerase III was not available at our center. Capillaroscopy was not performed. Transthoracic echocardiography revealed left ventricle ejection fraction of 69%, and there was no evidence of pulmonary hypertension. The routine chest radiography performed was normal. Computed tomography of the thorax showed no evidence of interstitial lung disease.
She was referred to the hematologist for initiation of chemotherapy and planned for subcutaneous azacytidine and tablet venetoclax. She fulfilled the 2013 American College of Rheumatology and European Alliance of Associations for Rheumatology classification criteria for systemic sclerosis with a total score of 12 (Table 1). She was treated symptomatically with low doses of calcium channel blocker to alleviate the symptoms of Raynaud's phenomenon and proton pump inhibitors with itopride to ease her dysphagia.
Both patients are currently still being closely monitored for the concomitant amelioration of their paraneoplastic systemic sclerosis condition while undergoing treatment for their primary cancers.
Autoimmune diseases triggered by tumor development, known as paraneoplastic rheumatic syndromes, are a well-established clinical phenomenon [5]. These syndromes can emerge at various stages of the tumor or metastases, either simultaneously with the cancer diagnosis or as an early manifestation. Since the initial report of paraneoplastic rheumatic syndrome in 1916, there has been a rise in the number of documented cases in the literature. Incidence rates ranging from 2.65% to 23.1% have been reported for paraneoplastic rheumatic syndromes [6,7]. The most commonly diagnosed paraneoplastic rheumatic syndromes include hypertrophic osteoarthropathy, polyarthritis, dermatomyositis/polymyositis, and paraneoplastic vasculitis. However, rare syndromes such as fasciitis, panniculitis, erythema nodosum, lupus-like syndrome, systemic sclerosis, and Raynaud's syndrome have also been reported. Recognizing the underlying tumor early is crucial, as treatment for rheumatic diseases may be more challenging and less effective. We shall not delay cancer diagnosis and management.
The development of systemic sclerosis is attributed to a combination of immunological dysregulation, vasculopathy, and hyperproduction of extracellular matrix by fibroblasts, resulting in skin fibrosis. Numerous epidemiological studies have consistently shown an increased age- and gender-adjusted risk of cancer in patients with systemic sclerosis compared to the general population [8,9]. Furthermore, it has been observed that patients who develop new-onset systemic sclerosis at an advanced age also face an elevated risk of cancer [10]. The existence of unique patient subsets displaying a temporal clustering of cancer diagnosis coinciding with the onset of systemic sclerosis raises the intriguing possibility that systemic sclerosis may be a paraneoplastic disease. Systemic sclerosis as a paraneoplastic syndrome has been reported in various literature. In previous reports, the neoplasms associated with paraneoplastic systemic sclerosis include breast, lung, ovarian, oral cavity, and pharynx cancer, non-Hodgkin lymphoma, and colorectal cancer [11-16]. In this case series, we present two cases of paraneoplastic systemic sclerosis associated with adenocarcinoma of the lung and acute myeloid leukemia, highlighting the importance of considering an underlying malignancy in patients presenting with sclerodermic clinical features.
There are no definite criteria to differentiate between primary autoimmune and paraneoplastic systemic sclerosis. Risk factors for paraneoplastic rheumatic syndrome include a personal or family history of cancer, carcinogen exposure, and advanced age of onset above 50. Constitutional symptoms such as fever, weight loss, and malaise may be prominent. The onset of paraneoplastic symptoms often closely follows the diagnosis of cancer. Our paraneoplastic systemic sclerosis case series featured two patients above the age of 50 with a strong family history of malignancy and a close temporal relationship between the onset of systemic sclerosis and the discovery of the associated cancers.
An increased incidence of ANA in malignancies has been documented in the literature. Moreover, the prevalence of paraneoplastic syndromes is significantly higher among neoplastic patients with positive ANA than those with negative ANA or healthy individuals [17]. Notably, one study reported an association between anti-Ro-52 antibodies and a higher prevalence of malignancy [18]. It is worth noting that our patients in this case series exhibited high levels of ANA titers and positive anti-Ro-52. Anticentromere, anti-topoisomerase I, and anti-RNA polymerase I-III are three major systemic sclerosis-specific antibodies. Various international systemic sclerosis cohorts have observed that systemic sclerosis patients with positive RNA polymerase III had malignancy diagnosed within a short interval of systemic sclerosis onset. However, antibodies against polymerase tests were not available in our center. Patients with negative antibodies against centromere, topoisomerase-1, and polymerase also had a higher risk of malignancy after the sclerodermic presentation [10].
Conventional standard-of-care medical therapy is often ineffective, but treatment of the underlying malignancy may improve the rheumatic symptoms. Recurrence of paraneoplastic symptoms with tumor recurrence is common [19].
In summary, paraneoplastic rheumatic syndrome can present rapidly, often with atypical symptoms, making it challenging to diagnose. The potential resolution or improvement of paraneoplastic systemic sclerosis with the treatment of an underlying neoplasm emphasizes the importance of considering the paraneoplastic hypothesis in patients with systemic sclerosis. Moreover, it highlights the necessity for more research into classifying this phenomenon to determine the true prevalence of paraneoplastic systemic sclerosis and further expand understanding of the complex bidirectional relationship between systemic sclerosis and malignancy. Increasing awareness through case reports and reviews can aid rheumatologists and oncologists in diagnosing and managing these cases collaboratively. To achieve the best patient outcome, interdisciplinary and timely management is crucial for the suspected paraneoplastic rheumatic syndrome.
Not applicable.
Written informed consent was obtained from the patient for publication of this case report and accompanying images and videos. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Not applicable.
The authors declare that they have no competing interests.
The authors declare that no funding was received for the publication of this case report.
SKI and SLC initiated the idea for case reporting and prepared the final copy of the manuscript with YHL and GRL. SLC is the managing rheumatologist. All authors had read and approved the manuscript.
Nil.
The authors declare that they have no competing interests.