Rheumatoid Arthritis is a very common entity, yet monoarticular presentation is very infrequent. We are reporting a case of sero negative rheumatoid arthritis affecting the knee joint.
32-year-old male presented to our department with pain and swelling of his right knee. There was no other joint pain, extra-articular manifestation or co morbid illness. His blood tests showed elevated inflammatory markers and negative autoantibodies. MRI showed effusion and extensive synovial hypertrophy. Arthroscopic synovial biopsy was done and histopathological examination was confirmative of rheumatoid arthritis. Patient was started on DMARDS and showed dramatic improvement.
Rheumatoid Arthritis should be suspected in patients with persistent pain and swelling and with poor response to treatment and surgical approach (arthroscopic debridement) should be offered as it is a useful tool for both confirming the diagnosis and as a treatment for the patient.
Rheumatoid arthritis, Seronegative, Monoarticular
RA: Rheumatoid Arthritis; LOM: Limitation of Movment; OPD: Out Patient Department; MRI: Magnetic Resonance and Imaging; Anti-CCP: Anti Citrullinated protein Antibody; DMARDS: Disease Modifying Anti Rheumatoid Drugs; SpA: Seronegative Spondyloarthritis; ACR Eular: An American College of Rheumatology/European League against Rheumatism
Rheumatoid arthritis (RA) is a chronic, systemic inflammatory disorder of unknown cause that can affect many tissues and organs, but principally attacks synovial joints. Its symmetric and infiltrative nature causes pain, edema, and limitation of movement (LOM) of multiple joints. Monoarticular RA is a rare entity reported to initially affect large joints such as hips and knees, progressing to a polyarticular presentation within 3-5 years [1,2]. We are reporting a case of Monoarticular Seronegative Rheumatoid Arthritis in a 32-year-old male.
32-year-old male presented to OPD (outpatient department) with pain and swelling of his right knee. Pain was sudden in onset and progressive over 2 weeks. No history of fever or trauma. He had a history of similar pain and swelling 1 year back for which arthrocentesis was done and took symptomatic treatment initially followed by Ayurveda treatment for couple of months. He was symptomatically better since then. Sudden knee pain and swelling started again two weeks back. No other joints involved. He doesn't have any other extra-articular manifestation or co morbidities.
His clinical examination was unremarkable except for the right knee. There was a diffuse swelling over knee and suprapatellar region (Figure 1). No dilated veins scars or sinuses No local rise of temperature. There was medial joint tenderness. Effusion with a positive patellar tap present. Both active and passive range of movements painless up to 90 deg but further limited by pain. Valgus/varus stress test negative. Mcmurray - negative, No clinical signs of instability. No distal neurovascular deficits. Other knee, both hips, both ankles and spine were clinically normal.
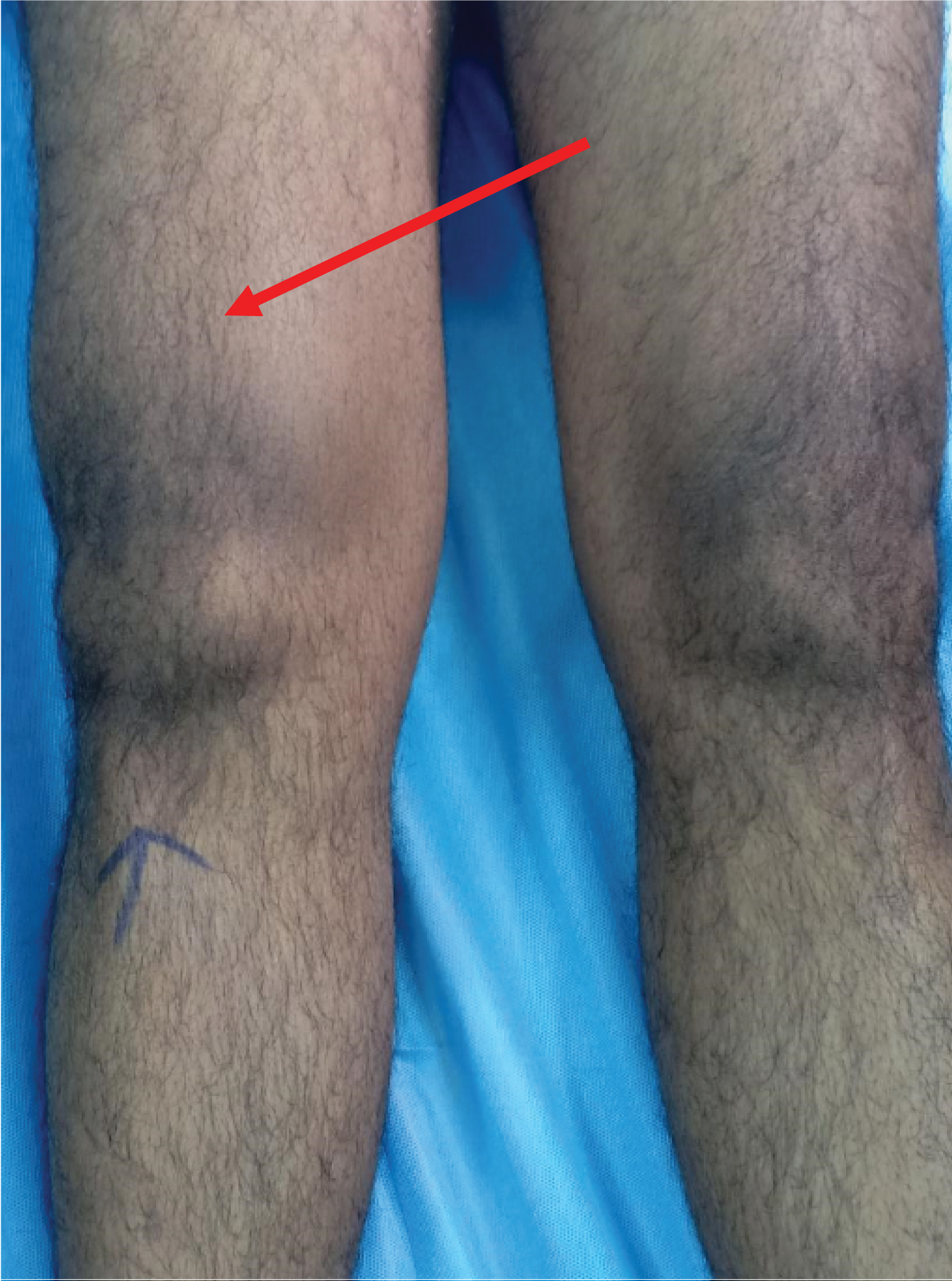 Figure 1: Clinical picture of knee showing effusion.
View Figure 1
Figure 1: Clinical picture of knee showing effusion.
View Figure 1
X-rays of both knees were normal except for soft tissue swelling (Figure 2), MRI (Magnetic Resonance Imaging) (Figure 3) of knee showed: Extensive synovitis in right knee joint with moderate to large volume effusion. Ligaments and menisci were intact. No significant cartilage erosions were seen.
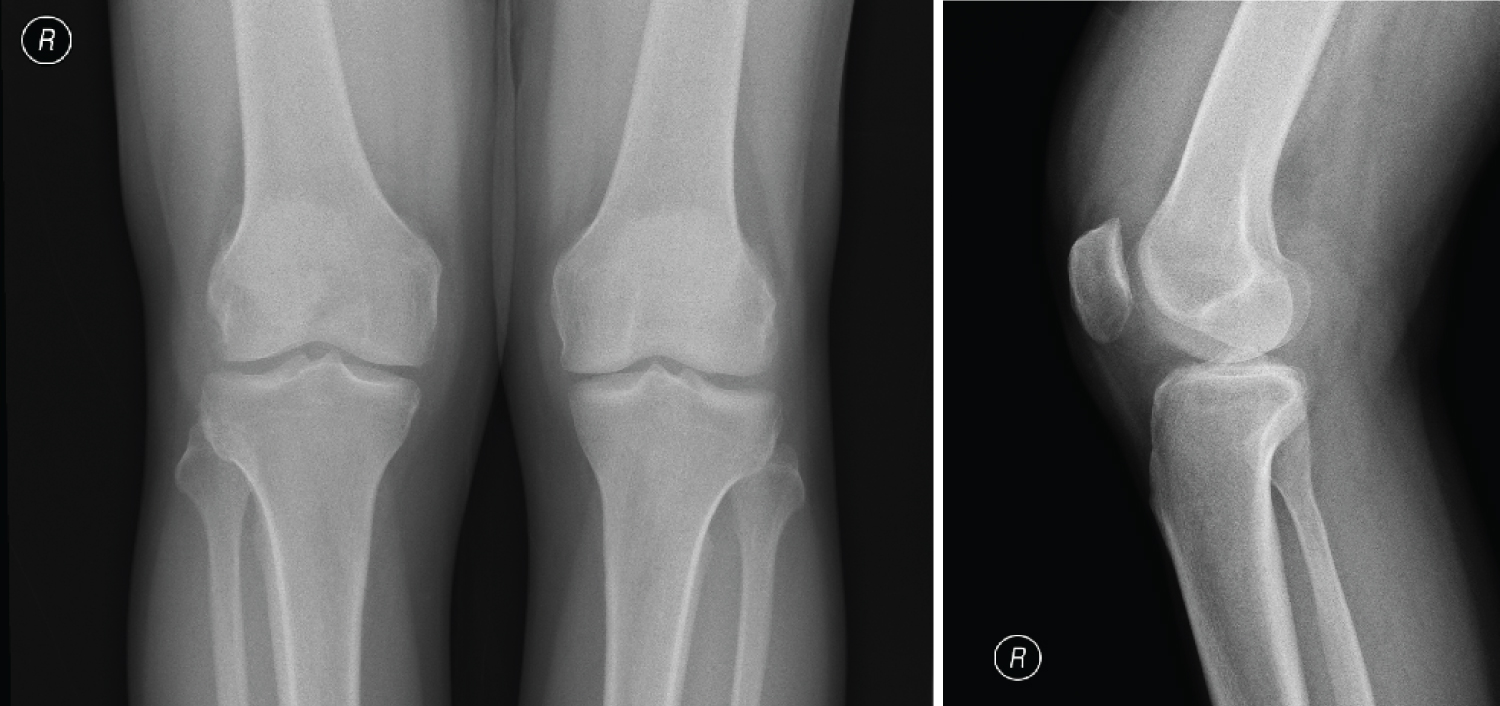 Figure 2: Weight bearing X-rays of both knees showing soft tissue swelling around knee.
View Figure 2
Figure 2: Weight bearing X-rays of both knees showing soft tissue swelling around knee.
View Figure 2
 Figure 3: MRI Image showing synovial hypertrophy and effusion.
View Figure 3
Figure 3: MRI Image showing synovial hypertrophy and effusion.
View Figure 3
Routine laboratory evaluation of the blood was inconclusive for any particular aetiology. (Hb-15.8 gm/dl, TC- N68 L25.7 M2.6 E3.2 CRP-28.1 Uric acid-6.4. RA Factor - < 10 IU/ml, Anti-CCP-8.54 U/Ml).
He was admitted and evaluated. As blood investigations were inconclusive for any particular pathology and the patient being symptomatic even after a course of anti-inflammatory medication, and MRI suggestive of synovitis it was decided to do a diagnostic arthroscopy along with arthrocentesis. He underwent arthroscopic synovial biopsy and synovial debridement Synovial fluid was aspirated before arthroscopy. Analysis was started as soon as the fluid was aspirated. The fluid was sent for bacterial, fungal cultures and microscopic evaluation.
Arthroscopy revealed extensive synovial hypertrophy with normal menisci and ligaments (Figure 4 and Figure 5). The hypertrophied synovium was debrided (Figure 6).
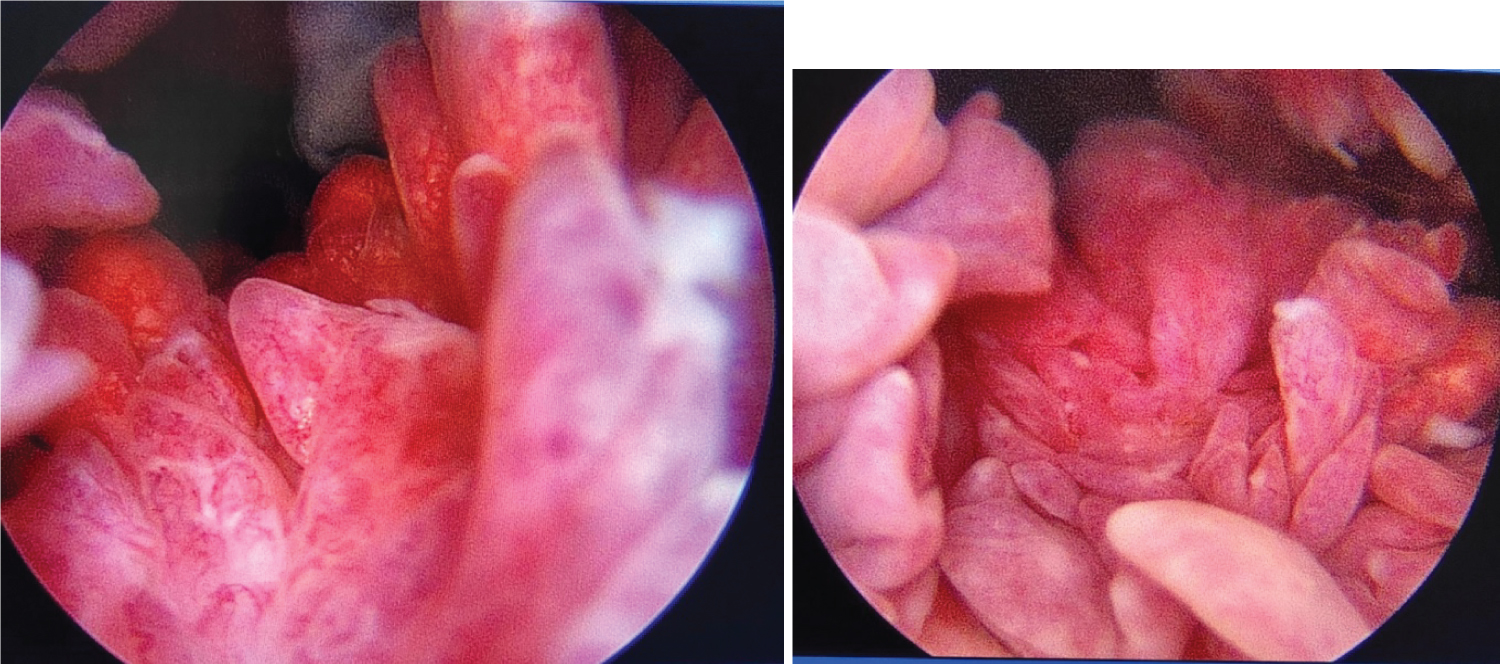 Figure 4: Arthroscopic images showing extensive synovial hypertrophy.
View Figure 4
Figure 4: Arthroscopic images showing extensive synovial hypertrophy.
View Figure 4
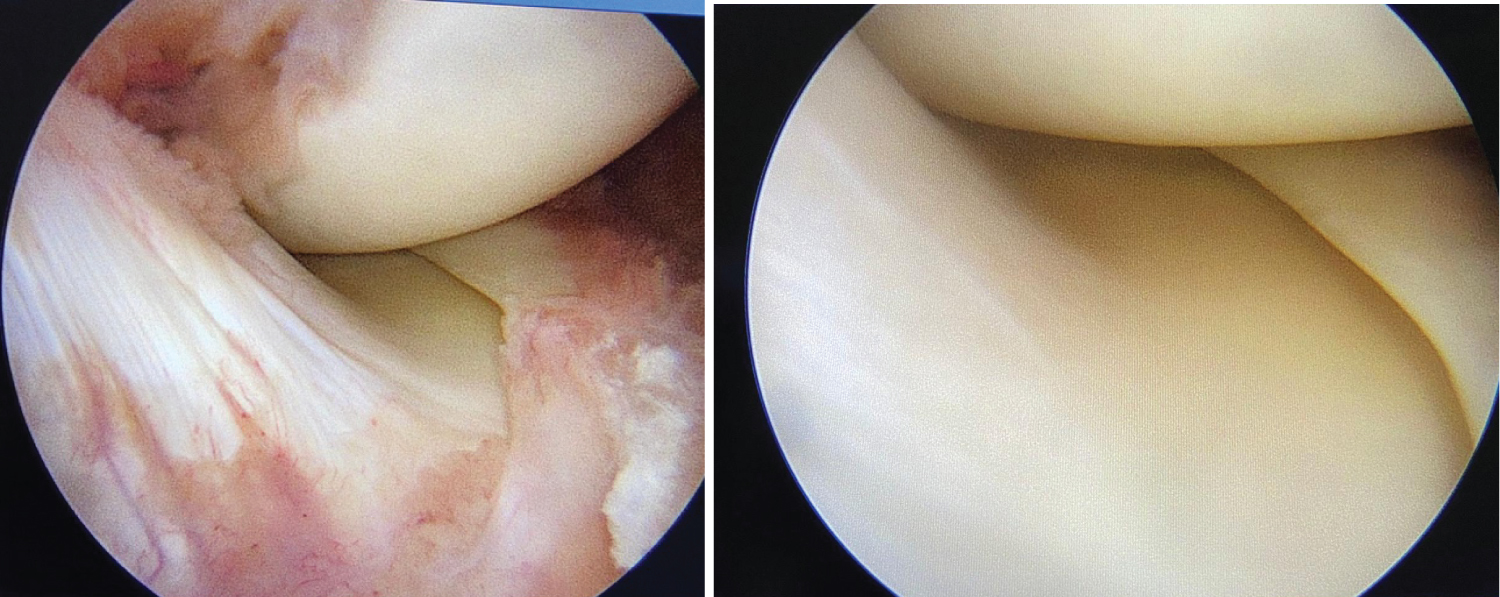 Figure 5: Showing normal menisci ligaments and articular cartilage.
View Figure 5
Figure 5: Showing normal menisci ligaments and articular cartilage.
View Figure 5
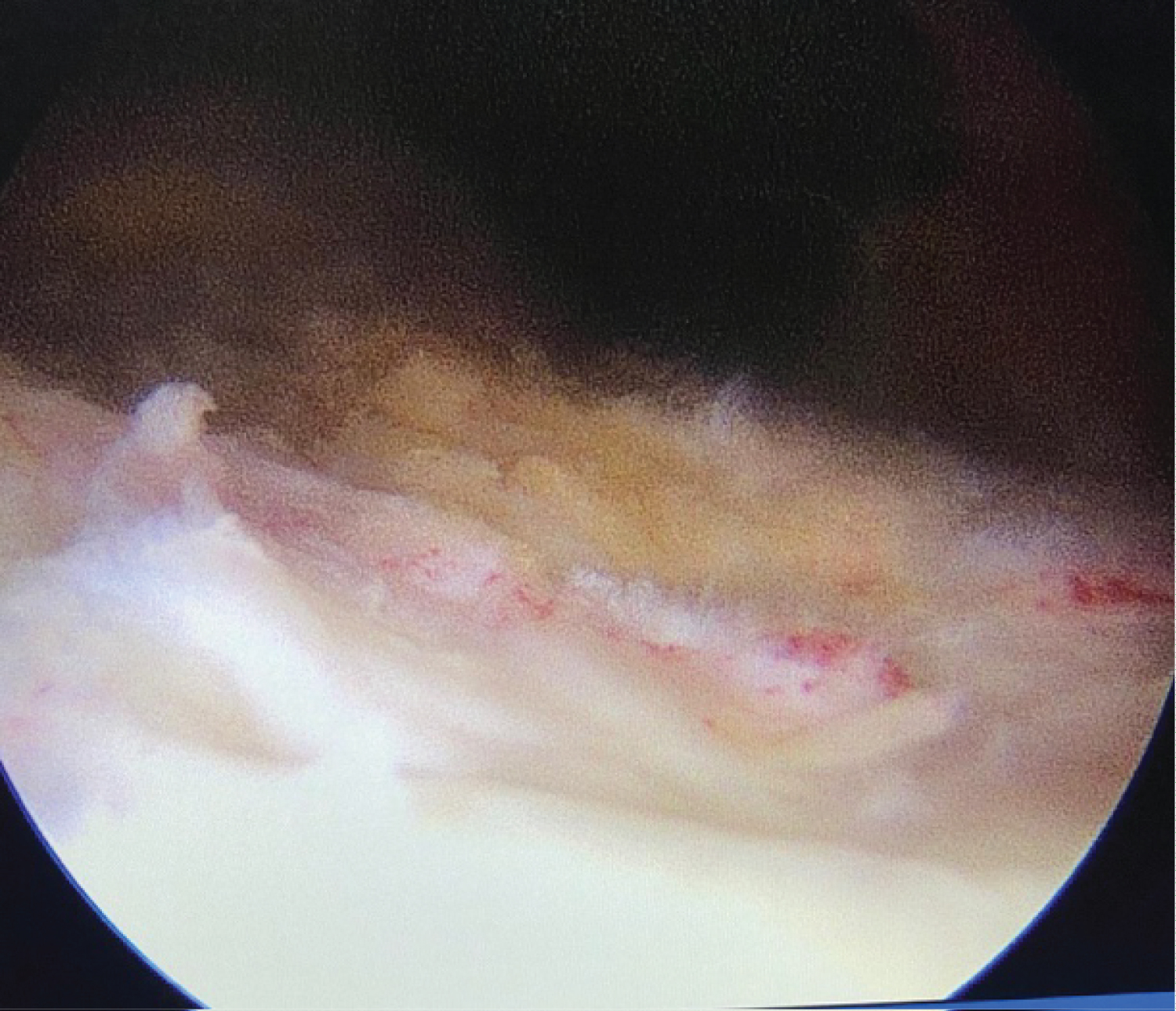 Figure 6: After debridement of synovium.
View Figure 6
Figure 6: After debridement of synovium.
View Figure 6
Synovial biopsy showed Sections showed fragments of fibro-adipose tissue with hyperplasia and hypertrophy of the synovial lining cells, resulting in a papillary pattern at the surface of the synovium. Fibrinous exudate admixed with occasional neutrophils was seen at the synovial surface in few foci. Sub-synovium showed vascular proliferation and dense perivascular infiltrates of lymphocytes and plasma cells (Figure 7a and Figure 7b). Lymphoid follicles are seen. Suggestive of Rheumatoid Arthritis.
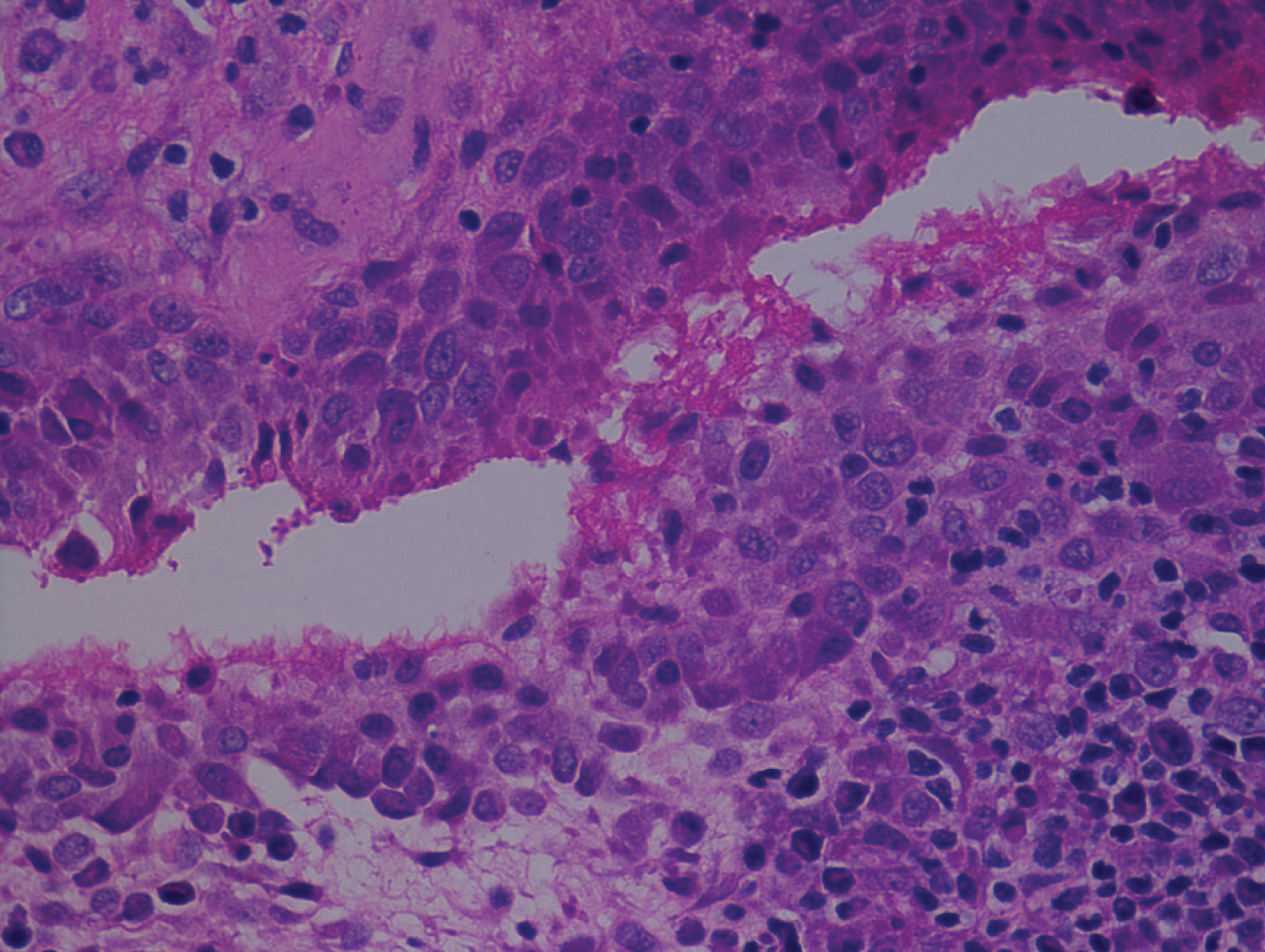 Figure 7a: Synovial biopsy showing hyperplastic hypertrophic synovial epithelium.
View Figure 7a
Figure 7a: Synovial biopsy showing hyperplastic hypertrophic synovial epithelium.
View Figure 7a
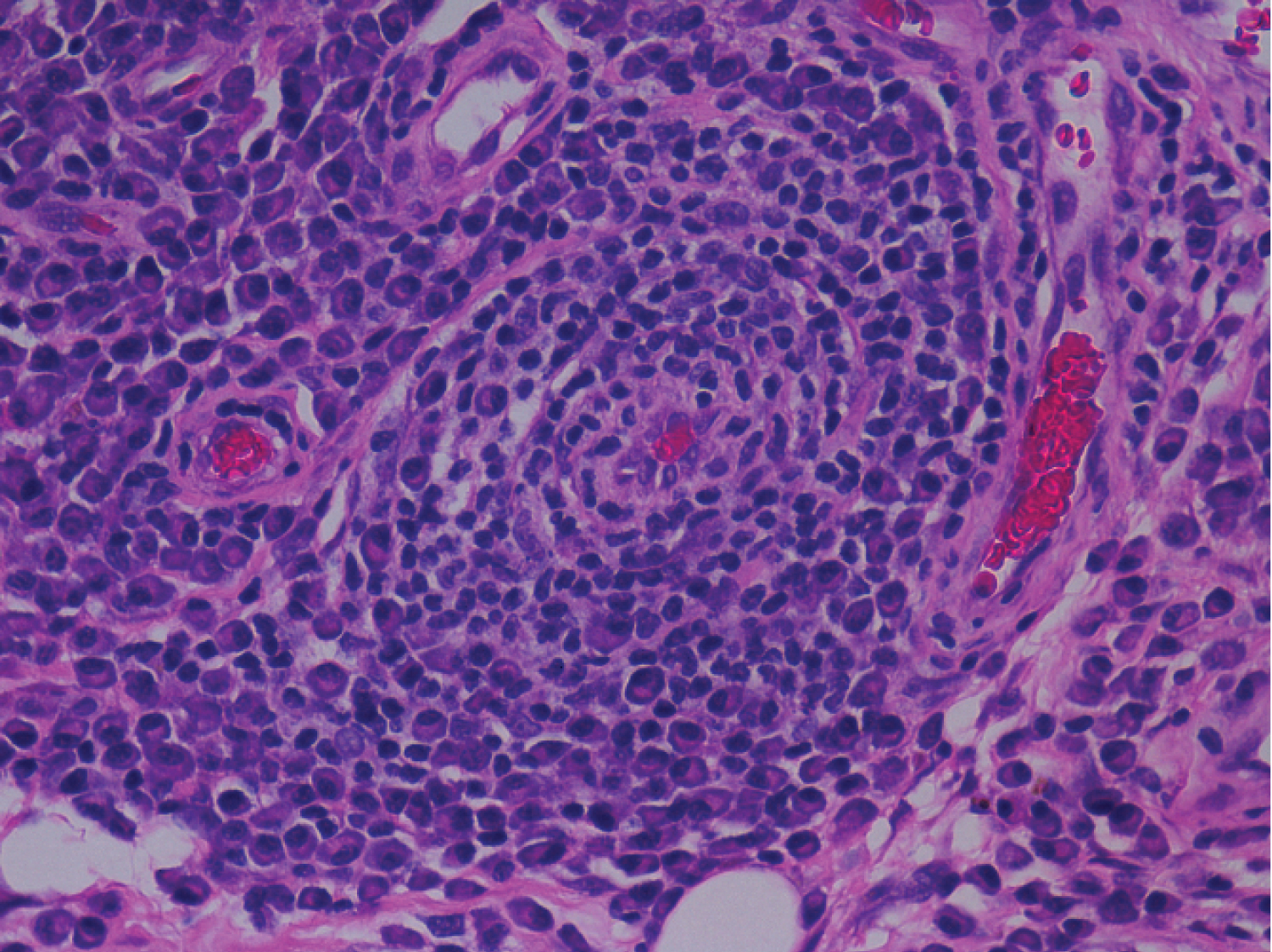 Figure 7b: Perivascular dense lymphoplasmacytic inflammation.
View Figure 7b
Figure 7b: Perivascular dense lymphoplasmacytic inflammation.
View Figure 7b
Synovial fluid culture was negative for any bacteria or fungal growth.
He improved symptomatically following arthroscopic debridement and was started on DMARDS (Methotrexate 10 mg for 6 weeks followed by 7.5 mg for 4 weeks).
In clinical practice, there is a tendency for very low clinical index of suspicion for RA in patients presenting with chronic monoarthritis, and other common etiologies are usually considered. Often, serology including RA Factor and anti-CCP do not help as they may be inconclusive. The first question during the evaluation process is to determine the duration of symptoms and establish whether it is acute or chronic monoarthritis. If symptoms persist for more than 6 weeks, the condition is considered to be chronic. A thorough history and physical examination supported by imaging and laboratory testing can differentiate between inflammatory and non-inflammatory monoarthritis. The possible aetiologies of chronic inflammatory monoarthritis include indolent infections such as tuberculosis, fungal and rare parasitic infections, crystal arthropathies, and autoimmune diseases such as arthritis due to seronegative spondyloarthritis (SpA) and, to a lesser extent, RA. The differential diagnosis in the noninflammatory monoarthritis domain includes pigmented villonodular synovitis, single joint osteoarthritis, and neuropathic arthropathy.
Rheumatoid arthritis presenting as monoarthritis has been reported in the literature by Parker, et al. [3] with the largest cohort seen in the 1980s. They reported that out of 150 patients evaluated over a 12-month period, 12.6% were diagnosed with RA [3]. In our case even RA factor and Anti CCP were negative, only synovial biopsy was conclusive of rheumatoid arthritis. As per ACR Eular [An American College of Rheumatology/European League Against Rheumatism] (Table 1) our case cannot be classified under rheumatoid arthritis. Arthroscopic synovial biopsy provides maximum opportunity in understanding the pathology in inflammatory arthritis [4]. Goeb, et al. [5] suggested that early diagnosis and early treatment initiation in patients with inflammatory arthritis can be possible by precise arthroscopic biopsy sample from the most representative pathological areas. Histological examination by arthroscopic synovial biopsy is of a significant diagnostic value in rheumatoid arthritis [6,7].
Table 1: ACR-Eular Criteria (> 6 Definitive RA). View Table 1
Arthroscopic synovial debridement has been shown to be effective in preventing the progression of the disease process [6,7]. Arthroscopic debridement of the involved synovium helps in reducing the symptoms and thereby reducing the subsequent cartilage destruction and thereby halting the progression of the disease along with the medical management.
Rheumatoid Arthritis should be suspected in patients with persistent pain and swelling and with poor response to treatment and surgical approach (arthroscopic debridement) should be offered as it is a useful tool for both confirming the diagnosis and as a treatment for the patient. Synovectomy helps in relieving the pain and acquiring early ambulation, when combined with Anti rheumatic medication it can be an effective tool in the management of rheumatoid knee and preventing the progression of the disease. Arthroscopic synovial biopsy and synovectomy gives good results in patients with chronic synovitis of the knee [8]. Arthroscopic management offers the following advantages over open synovectomy: A more thorough evaluation of the joint and synovium, better access for surgical synovectomy, and decreased postoperative morbidity [9].
We would like to thank Mrs. Aleena Antony MSW Senior Counsellor for helping us in drafting the document and collecting the details for publishing the manuscript.
Written Informed consent was taken from the patient and relatives to use the clinical images and clinical details for publication purpose.
None.