Introduction: Circulating Vaccine Derived Poliovirus (cVDPV), is a genetic mutation of the Sabin virus. Sierra Leone reported its last case of wild polio virus in 2010. However, in December 2020, the national disease surveillance program was notified of three people with acute flaccid paralysis who had cVDPV2. We investigated to identify the source, determine the magnitude of the outbreak and risk factors.
Methods: We assessed the clinical and vaccination status of the cases, searched for trivalent-OPV (tOPV) and monovalent-OPV (mOPV2) in the health facilities serving the affected communities. We searched for additional cases in the affected communities and collected stool specimens from contacts of case-patients. We assessed the cold chain management and routine immunization services. We conducted a vaccination coverage survey using the WHO zero-dose case investigation form in 128 randomly selected households of the affected communities.
Results: Case-patients were 26-month-old male from Kambia, 39-months-old female from Western Area rural, and 15-month-old female from Tonkolili district. All had fever and acute paralysis. No tOPV or mOPV were found in the facilities. Infections in two case-patients were genetically linked to cases in Guinea and Cote d'Ivoire. There was no history of travel within 21-days of onset of symptoms for all cases. All received three doses of OPV, two received one dose of Inactivated Polio Vaccine (IPV). Fourteen (47.4%) contacts tested positive for poliovirus type 2. Cold chain status at facilities was poor. Only 47% (44/93) of children 0-59 months received three doses of OPV and 48% (30/63) received one dose of IPV.
Conclusion: The cVDPV2 may have been imported from neighbouring countries. OPV and IPV coverage was low, and poor cold chain may have reduced the vaccine potency. We conducted enhanced surveillance and prepared for nOPV2 vaccination. We recommend strengthening AFP surveillance, routine immunization and improve cold chain management.
Circulating Vaccine Derived Poliovirus (cVDPV), Poliovirus, Sierra Leone
The World Health Assembly (WHA) adopted a resolution for the worldwide eradication of polio in 1988. At that time, there were more than 350,000 polio cases across 125 endemic countries globally. Since then, the Global Polio Eradication Initiative (GPEI) has reduced the number of endemic countries to 2 countries (Afghanistan and Pakistan) and also reduced the number of wild polio cases to 9 cases in these two endemic countries, as of June 20, 2022 [1]. After the Wild polio virus type 2 (WPV2) was eradicated in 1999, only two strains Wild Polio Virus type1 (WPV1) and Wild Polio Virus type3 (WPV3) remain in circulation. The 2013-2018 Polio Eradication and Endgame Strategic Plan has narrowed the gap in polio eradication and set the stage for a final eradication from the globe [2].
In August 2020, the World Health Organization (WHO) certified the African Region free of indigenous WPV transmission [3]. Although the globe is on the verge of WPV eradication certification, the achievement in the African region was challenged by outbreaks of circulating vaccine derived polio virus type 2 (cVDPV2)., which is derived from the oral polio vaccine (OPV). Despite significant progress in curbing WPVs in Africa, the cVDPV2 continues to expand across parts of central Africa, the Lake Chad region, the Horn of Africa and many West African countries including Ghana, Nigeria, Senegal, Guinea etc. Globally, a959 human cases and 411 positive environmental samples of cVDPV2 were reported in 27 countries in 2020 [4].
Globally, Afghanistan and Pakistan are the only countries reporting cases of wild polio virus [2,5,6]. The establishment of the global polio Eradication initiative (GPEI) in 1988 with the aim of completely eradicating polio viruses by the year 2000 has not been achieved even after three decade, but has made a significant impact or progress by reducing the number of polio cases and countries with wild polio virus to just two 2 [4,7]. For several years, a lot of eradication activities have been conducted globally in a well-coordinated way, and as a result of these activities Africa including Sierra Leone has been declared as wild poliovirus-free on August 25 2020 [8].
However, despite such progress, in 2021, the GPEI faces substantial novel challenges with managing outbreaks of cVDPV2s, a genetic mutation of the Sabin virus. A full five year after the global coordinated removal of serotype 2 oral poliovirus vaccine (OPV2) [9] from trivalent oral poliovirus vaccine (tOPV) for use in the national immunization programs, most countries delayed to avoid using mOPV2 by waiting for the nOPV2 availability, insufficient coverage of vaccination and validation of meeting the criteria for nOPV2 initial use, resulting from reversion to neurovirulence of attenuated vaccine virus [10-12]. Despite the Certification of the wild poliovirus, Africa’s fight against polio isn’t over because in many countries, vaccination is done with oral drops containing a weakened form of the poliovirus which sometime mutates into a strain that can spread in under- immunized communities and cause paralysis [2,3]. In 2020, 959 human cases of circulatory vaccine- derived polio type 2 (cVDPV2) and 411cVDPV2- positive environmental samples were reported globally from 27 countries, of which 21 were from African Region including Sierra Leone [13,14].
Sierra Leone did not report any case of circulatory Vaccine Derived Poliovirus (cVDPV), until recently on the 10 th of December 2020 when the WHO Sierra Leone country office notified the National Disease Surveillance program about a child with acute flaccid paralysis who had cVDPV2 from Kambia District. On the following day, two additional case were reported, one from Tonkolili and one from Western Area Rural districts [10]. On the next day of notification, the National Rapid Response (NRRT) team was dispatched to support the districts on investigation of the event, identify the source of infection, determine the magnitude, scope of the outbreak and the risk factors contributed to it.
The Emergency Operation Centre (EOC) has been activated to level 2 and regular meetings were being held at the national and district level . The national Rapid Response Teams (RRTs) were dispatched to the affected districts to support them with investigations and risk assessment. The polio outbreak response plan has been developed which included plan for a vaccination response.
We employed descriptive study to investigate the outbreak of circulating vaccine derived Polio-Virus type 2 (cVDPV2) in Tonkolili, Western Area Urban, and Kambia Districts, in Sierra Leone.
Tonkolili district: This district comprises of eleven chiefdoms, and it is centrally located in the country with Magburaka as the capital, while Mile 91 is the commercial centre. The population of the district is 530 000. Number of facilities, population under fifteen, number of healthcare workers etc. are more relevant than geographic description.
Kambia district: Is in the North-Western Province, and borders by Republic of Guinea in the North, Port Loko district in the South and Bombali district in the East. Kambia town is the largest town and the district capital. The district provides a vital trade route between Sierra Leone and the neighboring Republic of Guinea. The total population size of about 404,822, under fifteen population and 108,145 (44.5% of total population) etc.
Western area rural district: This district is located predominantly around the peninsula in the western Area of Sierra Leone. The Freetown peninsula consists of three parallel ranges of highlands that are narrow but extend about 30 km south of Freetown.
Suspected case: A Suspected case is any case presenting with Acute Flaccid Paralysis (AFP) case is defined as a child < 15 years of age presenting with recent or sudden onset of floppy paralysis or muscle weakness due to any cause, or any person of any age with paralytic illness if poliomyelitis is suspected by a clinician.
Confirmed: A Suspected case with isolation of WPV or VDPV in stool specimen collected from a suspected case or a close contact.
Compatible: A suspected case with no adequate specimen collection, no isolation of WPV or VDPV from the case or close contacts and residual paralysis after 60 days follow up that is deemed by the national expert review committee to be clinically and epidemiologically compactable with poliomyelitis.
Contact: A Contact of AFP case is defined as a child less than 15 years of age who had been in direct contact with the index AFP case within one week prior to the onset of paralysis and/or within two weeks after onset of paralysis.
We used the WHO Zero Dose Polio Compatibles Sabin2 and VDPV case Investigation Form to collect data from the cVDPV2 confirmed cases and we used the Integrated Diseases Surveillance and Response Case Investigation form to collect data from suspected and probable AFP cases.
We collected demographic data such as age, sex, occupation, address, clinical data such as signs and symptoms, risk factors information including travel history. Stool samples were collected from contact of case-patients to test for the presence of the polio virus infection and collected blood specimen from case patient to test for immunogenicity. We reviewed records from five health facilities to identify missed cases and search for additional cases. The immunization performance of the affected districts and the vaccination status of the cases were assessed. Furthermore, the investigation searched for trivalent-OPV (tOPV) and monovalent-OPV (mOPV2) in the health facilities serving the affected communities to identify possible source of infection.
A total of 19 Close contact with case-patients were identified, two stool sample were collected from each in 24 hours apart and tested for wild or cVDPV2 infection. We checked on the availability of refrigerators, cold boxes, and vaccine carriers. Physical search on the availability of all polio vaccines to know their potency, expiring date and VVM stage. Also, we monitored the fridge tag 2 and the temperature recording chart for proper temperature.
The performance of the district in routine immunization was also assessed based on coverage of OPV3, dropout rate etc. We reviewed the immunization registers to identify missed and defaulter cases. V accination coverage survey was conducted using the updated WHO Zero dose case investigation form in 128 randomly selected households of the affected communities. Households which have at least one child of age under-five years were included in the survey. We reviewed the immunization card of all under five children in the selected households to assess the polio immunization status of the children and understand the risk of polio transmission in the communities.
The districts AFP surveillance performance was assessed based on key AFP surveillance indicators mainly non-polio AFP detection rate, stool adequacy rate, non-polio enterovirus isolation rate etc.
The investigation team identified three positive cases for cVDP in three districts, one in Western Area Urban, one in Kabmia, and one from Tonkolili.
Case-patient 1: On the 27 th of October 2020 a 26-months-old male, resident of New London, Kambia II town developed high fever and partial weakness of the lower limb. On the 30 th of October, 2020, he was brought to the Kambia Government Hospital (KGH), during his examination by a clinician, the child had high fever and weakness of the lower limb with a preliminary diagnosis of cerebral palsy and then antibiotic injection was prescribed. The child was ill-looking, mildly pale, moderately malnourished, slightly febrile (temperature 37.80 C) with tetraparesis (flaccid paralysis) predominantly in the lower extremities but fully conscious. The child was irritable and mild respiratory distress with marked tenderness and reduced stimuli in all limbs. Muscle power at detection was 3/6, mRDT positive, Hb 7.6 g/dl, no abnormality detected in the other systems.
On the 4 th November, 2020 the District Surveillance team was notified about the case in the hospital as a suspected Acute AFP case. The case was immediately investigated, two stool Samples were collected within 24 hours. The case hadno travel history, no contact with AFP case and had received three doses of polio vaccine in addition to IPV as per the immunization card. On the 6 th of November, 2020 the stool samples were sent to the Central Public Health Reference Laboratory (CPHRL) and on the 4 th December, 2020 the samples were subsequently shipped to Abidjan-Ivory Coast for confirmation.
On 10 th December 2020 at 6:51pm the national surveillance program received notification email from the World Health Organisation (WHO) country office that a Poliovirus type 2 (PV2) was isolated from the stool samples collected from Kambia district. The samples were also referred for sequencing in the National Institute of Communicable Diseases (NICD), South Africa, the Regional Polio Reference Laboratory for the validation of the initial results and to determine the source and the origin of the virus. On the 11 th of December 2020 at 2: 45pm the national Surveillance team informed the Kambia district surveillance team about the confirmed Poliovirus type 2 (PV2) from the stool samples collected from this patient. However, within few weeks the case-patient symptoms became worsen and was unable to survive and died on the 15 th December, 2020.
Case-patient 2: On the 19 th November, 2020, a 15 months female child presented with fever, acute symmetrical paralysis of the lower limb, severe malnutrition at Wundugu New Ferengbeya Community Health Post (CHP), Dansogoia Chiefdom-Tonkolili District. On the 24 th November, 2020 a community informant through the Auto-Visual AFP Detection and Reporting (AVADAR) program notified the Tonkolili district surveillance team about the case. On 25 th of October 2020, the team investigated the case and collected two stool samples within 48 hours. The child had no recent travel history, no contact with any AFP cases and had received three doses of the oral polio vaccine. On the 28 th of November 2020 the samples were sent to the CPHRL who then shipped the samples to the regional laboratory in Abidjan, Côte d’Ivoire onthe 30 th November, 2020.
On the 13 th of December 2020 the national surveillance team received the result which indicated that Poliovirus type 2 (PV2) was isolated from the samples. The samples were also sent to the National Institute of Communicable Diseases (NICD), South Africa (the Regional Polio Reference Laboratory) to confirm the initial results and do sequencing to determine the source and the origin of the virus. The outcome of the result from South Africa indicated a vaccine derived Type 2 polio and genetically linked to Cote d’Ivoire. However, due to timely medical interventions, the patient-case had improved prognosis and partially recovered and discharged to his home.
Case-patient 3: On the 11 th November 2020, a 39 months male child presented with fever, acute malnutrition, diarrhoea and weakness of the left lower leg, weakness of the lower limbs at the Black Hall Road Community, Freetown. On the 27 th of November 2020 the child was treated at home with drugs bought from a drug store, but the fever could not subside. The mother was asked by her husband to take the child to the hospital for treatment. First, the mother took the child to a nurse nearby their home who gave the child two crystalline injections for two days. After three days of treatment at home, the child who was initially walking prior to the treatment started experiencing weakness of the lower limbs.
On the 4 th of December, 2020, due to the unusual symptoms observed by the mother prompted her to take the child to the Ola during Children’s Hospital (ODCH) for further treatment. The hospital IDSR focal notified the Western Area Urban DHMT who investigated the case and collected stool samples within 24 hours. The case took three doses of oral polio vaccine, no contact with any AFP case and had no recent travel history. On 7 th December, 2020, case-patient samples were sent to CPHRL and then the samples shipped to the regional laboratory in Abidjan, Côte d’Ivoire.
On the 4 th January, 2021 the national surveillance team received samples result which indicated an isolation of circulating vaccine derive poliovirus type 2 (cVDPV2). The samples were also sent to South Africa for sequencing. The result shows that the case was genetically link to Guinea. Due to the timely medical intervention, the child was fully recovered, discharged from hospital to his home. From the active case search conducted, two additional cases were identified of acute flaccid paralysis in the affected communities who met the standard case definition for poliomyelitis.
From the total of 19 stool samples collected from close contacts of the confirmed cases, 14 (47.4%) were found to be positive of the poliovirus type 2. No tOPV or mOPV2 vaccines in the health facilities serving the affected communities (Figure 1).
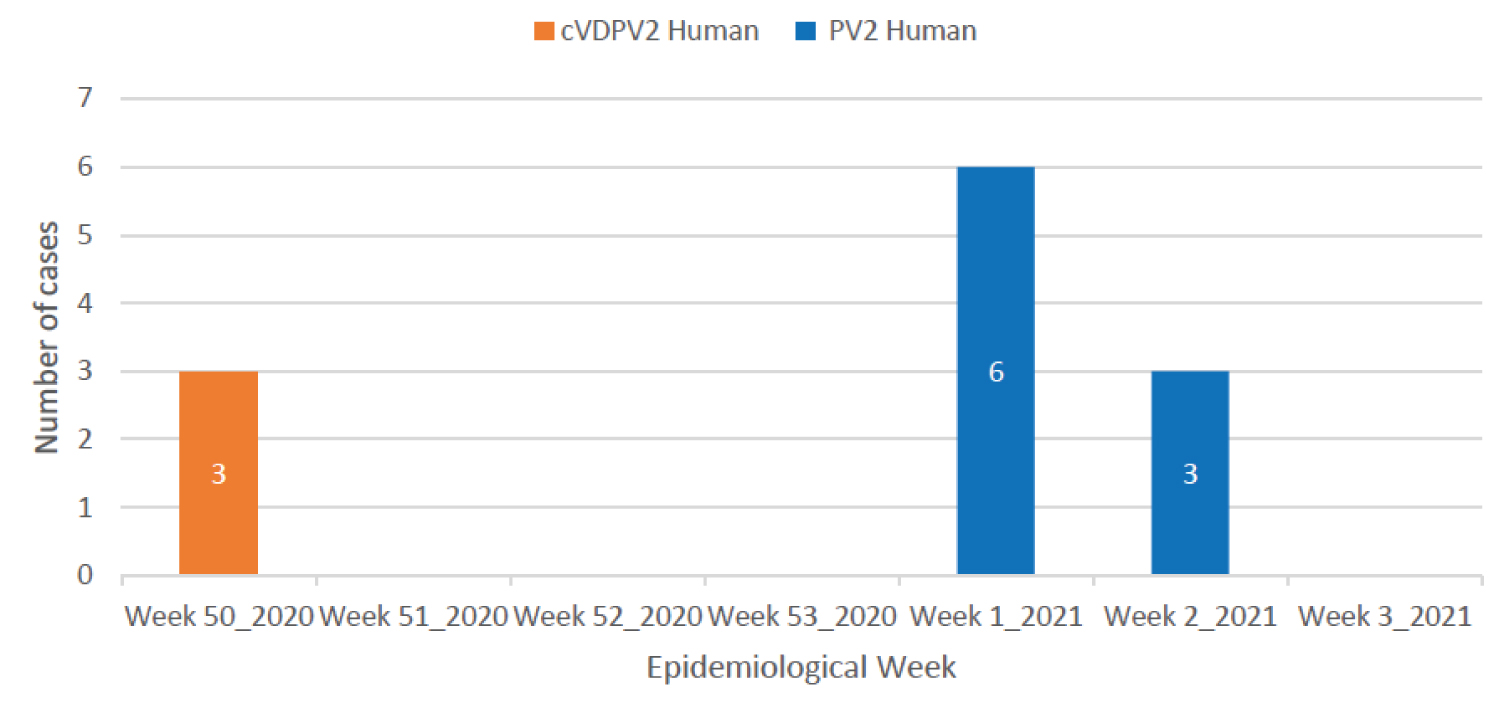 Figure 1: Cases of Polio by week of confirmation, Sierra Leone, 2020-2021 (n = 12).
View Figure 1
Figure 1: Cases of Polio by week of confirmation, Sierra Leone, 2020-2021 (n = 12).
View Figure 1
The rapid immunization survey showed that 47% (44/93) of the children (0 to 59 months) had received at least 3 doses of OPV during routine immunization services, 48% (30/63) of the children age (0 to 59 months) had received at least one dose of IPV (Figure 2 and Figure 3).
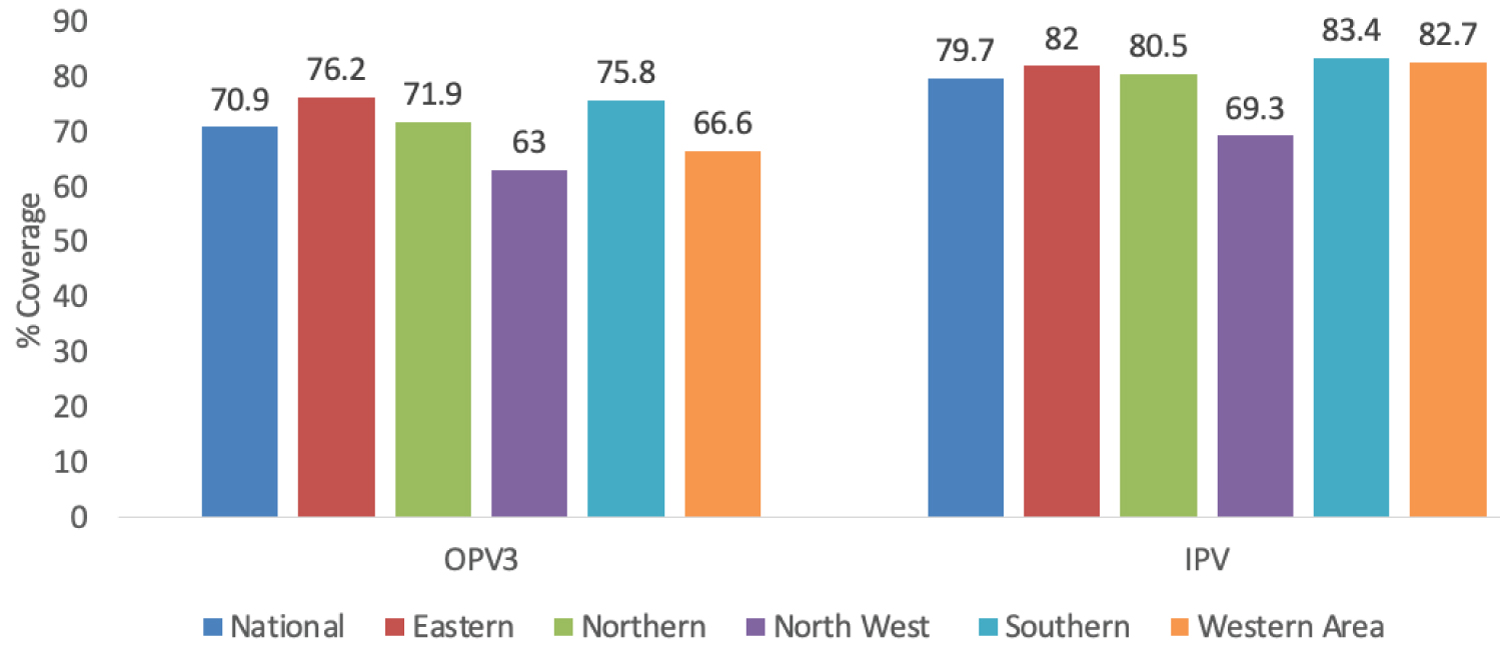 Figure 2: Immunization coverage by province, Sierra Leone, 2019 (DHS 2019).
View Figure 2
Figure 2: Immunization coverage by province, Sierra Leone, 2019 (DHS 2019).
View Figure 2
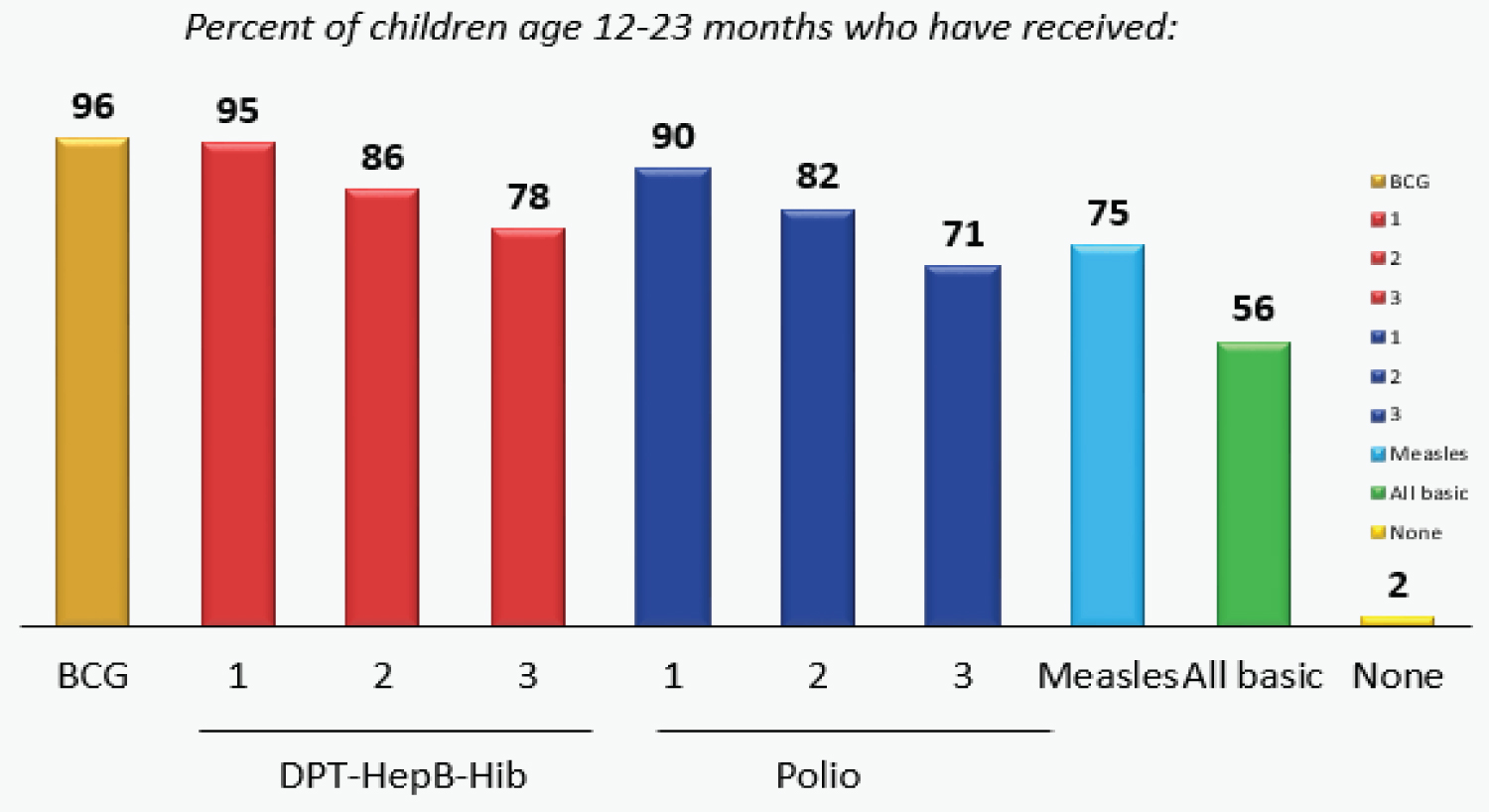 Figure 3: Percentage of children age 12-13 months who have received vaccination.
View Figure 3
Figure 3: Percentage of children age 12-13 months who have received vaccination.
View Figure 3
According to the routine administrative immunization data for 2020, 10 districts have an OPV3 coverage above the minimum target of 80%. Six districts that are below the 80% target includes: Tonkolili (78%), Bombali (73%), Karene (69%), Falaba (63%), Western Area Urban (54%) and Kono (71%). Likewise, 10 districts have an IPV coverage above 80% while 6 districts have an IPV coverage below 80.
National AFP detection rates for 2017, 2018 and 2019 were 2.5, 3.8 and 3.8 respectively. The preliminary national non-Polio AFP detection rate for Sierra Leone in 2020 was 3.2 per 100,000 while stool adequacy was 80.0%. Preliminary data for 2020 shows only 2 districts had not met the minimum target of nonpolio AFP rate of 2/100,000 (Kambia and Port Loko. But 8 out of 16 districts had not met the target of 3 per 100,000 which is mostly used for risk assessment: Kambia, PortLoko, Moyamba, Bonthe, Pujehun, Bo, Kenema and Kailahun. Five districts had not met the stool adequacy target of 80%: Western Urban Kono, Bo, Pujehun and Bonthe.
Following the investigation of this outbreak, a total of 38 confirmed cVDPV2 were detected, of which 9 (23.7%) were detected through environmental surveillance, for example from samples collected from the environment, 15 (39.5%) were from AFP cases, and 14 (36.8%) were from contacts of the confirmed cases. The median age of the cVDPV2 cases detected through AFP samples was 32 months (range: 14-55 months). All 15 AFP cases had received at least three doses of OPV (Table 1, Figure 4 and Figure 5).
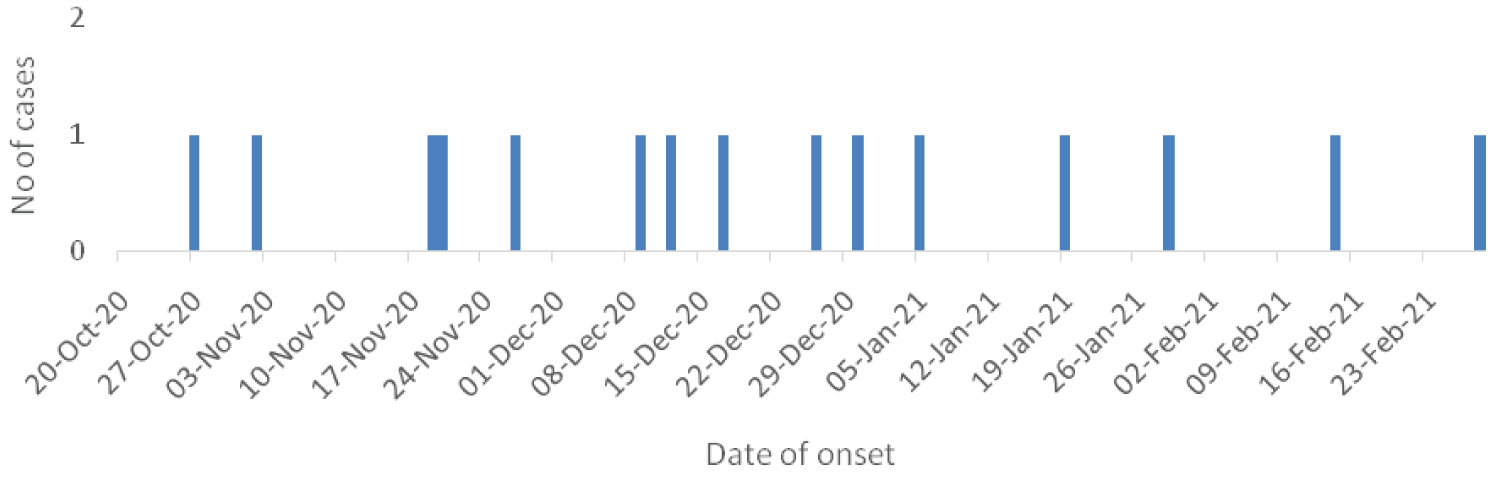 Figure 4: Confirmed cVDPV2 AFP cases by date of onset (N = 15).
View Figure 4
Figure 4: Confirmed cVDPV2 AFP cases by date of onset (N = 15).
View Figure 4
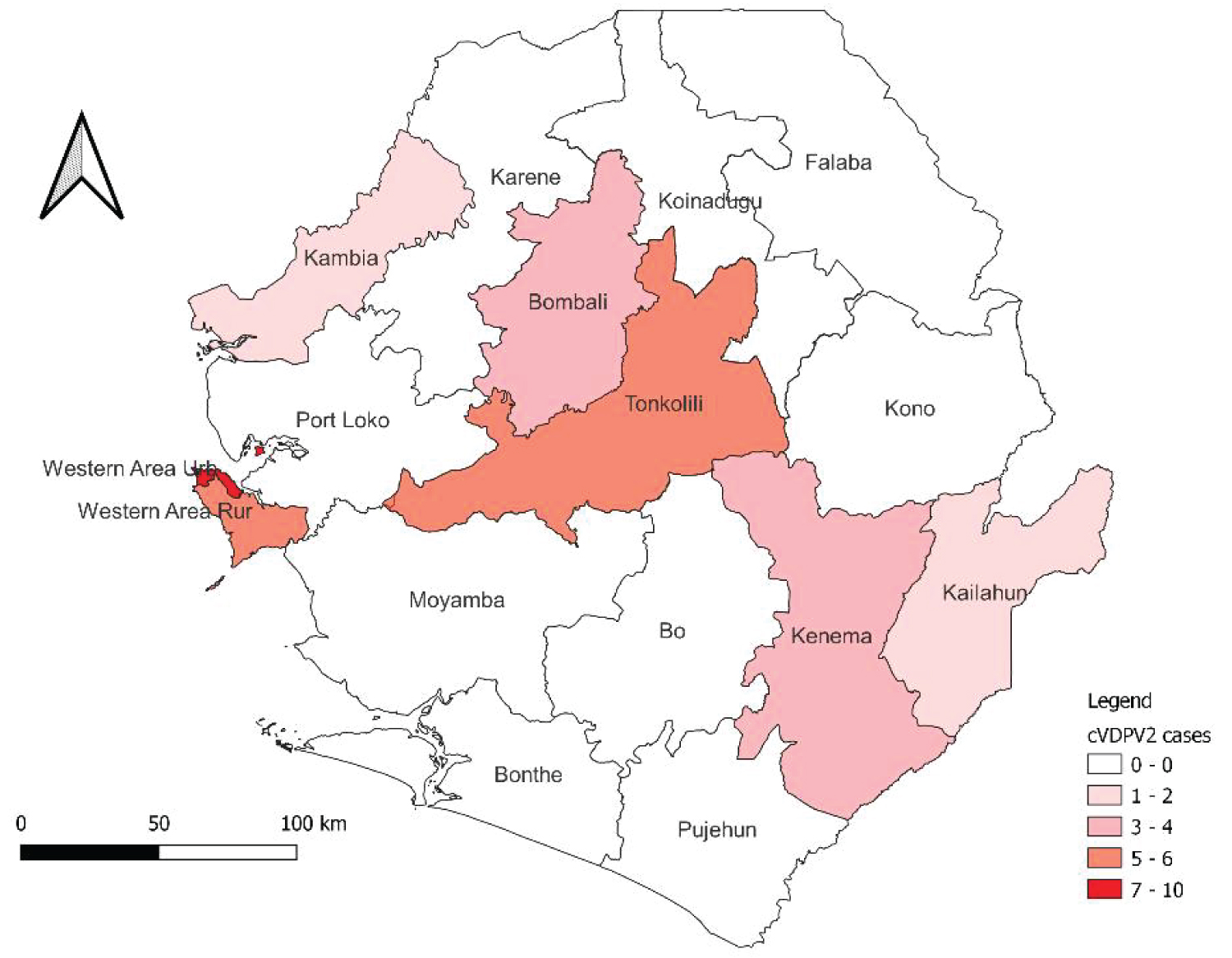 Figure 5: Distribution of cVDPV2 cases by district, Sierra Leone, 2020-2021.
View Figure 5
Figure 5: Distribution of cVDPV2 cases by district, Sierra Leone, 2020-2021.
View Figure 5
Table 1: IPV vaccination status of confirmed cVDPV2 AFP cases (N = 15). View Table 1
The 2020 cVDP2 outbreak was the first to be reported from Sierra Leone with confirmed cases from three Districts: Kambia district, Tonkolili and Western Area Rural. In total, 38 case were confirmed, xx males and xx female between the ages 15-39 months. The polio outbreak then constituted a significant threat to the World Health Assemble-endorsed targets of stopping all forms of poliovirus transmission in the world [15]. The outbreak also signalled the susceptibility of security-compromised populations which is worsened by the weak healthcare system.
The source of the infection for all cases could not be identified and no evidence of travel history of the case patient. However, the cases may have contacted an asymptomatic patient who might have travelled to the affected countries. The finding from the risk assessment indicates that tOPV or mOPV2 was not found in the affected health facilities, it is unlikely that the virus is derived from the vaccine administered to the children. This is similar to a study conducted in Korea 2012 to 2019 about the resurgence of polio occurring almost 20 years after polio eradication was declared in Asia has been reported which was believed to be imported from another country [16].
The result from our routine immunization shows low coverage for children aged 0 to 59 months OPV 47% and IPV 48% which could be the reason for the outbreak of vaccine derived polio in the country. This study is similar to the study conducted in Ghana 2019 that assessed the immunized children fully immunized were 49% after the diagnoses of circulating vaccine derived polio virus in the northern region [10]. The finding conducted from the blood samples collected from the case patient indicated that cases 1 and 2, cases from Kambia and Western Area Rural districts were genetic linked with cases in Guinea and case 3, which was reported from Tonkolili District was linked to cases in Cote d’Ivoire, which implies the possibility of importation of cVDP2 in the country. This study is similar with the study conducted in the Accra Institute for Medical Research were the cVDPV2 was isolated from the site were the AFP or poliovirus was identified from AFP contact children [17]. Individuals in contact with AFP cases have a higher likelihood of asymptomatic infection and virus excretion than people who have not had contact. The collection of stool specimens from contacts of AFP cases provides an additional approach to determine if poliovirus is the cause of paralysis in an AFP case.
This investigation confirmed the occurrence of circulatory vaccine derive polio (cVDP2) outbreak in Sierra Leone. However, the source of infection was not identified, the health authorities need to increase the inactivated polio vaccine coverage to prevent further spread of cVDPV. Health workers should always look out for polio-like symptoms of acute flaccid paralysis among children by testing the presence of polio virus in the patient’s stool samples. The risk assessment findings indicates that more than 50% of the children surveyed did not receive at least one dose of IPV which has the tendency to increase the poliovirus infection due to the high number of unvaccinated children. Therefore, the risk of infection and circulation in Sierra Leone is high. Based on the results of the investigation and also global data on cVDPV, nOPV2 campaign was conducted to stop and contain the circulation of the virus. Enhanced AFP surveillance activities including active case search and sensitization of district surveillance officers and district lab focal persons.
The Sierra Leone MOHS was recommended to strengthen routine immunization, especially across border districts and improve IPV coverage, and to enhance AFP surveillance. The Government conducted nationwide nOPV campaign and contained the CVDPV circulation by June 2021. Another approach to totally eliminate the risk of re-emergence of cVDPV2 is to utilize bivalent OPV that contains Sabin serotypes 1 and 3 strains, instead of trivalent OPV that contains Sabin strains of all three poliovirus serotypes and also and conduct cross-border vaccination at permanent transit point and the surveillance of nomadic population.