Poliomyelitis is one of the leading causes of paralysis among children under five years of age, and has been a major public health threat until recent times when high success rates were attained in poliovirus elimination through massive vaccination campaigns in various regions worldwide. In the course of vaccination, a new trend of vaccine-derived poliovirus occurred, due to genetic reversions in the live attenuated oral polio vaccine that resulted in the emergence of virulent forms. To tackle this menace, a change in vaccination schedule should be implemented in the affected countries, such that the live attenuated oral polio vaccine be replaced with the inactivated poliovirus vaccine, or the bivalent oral polio vaccine should be used in place of the trivalent form.
Poliovirus, Vaccine, Outbreak, Paralysis, Eradication
In past times, Poliomyelitis has been a major public health threat worldwide as one of the leading causes of paralysis among children under five years of age. The disease is known to cause muscle wasting and acute flaccid paralysis in the extremities, mostly in the lower limbs, leaving the sufferers with deformed limbs and locomotion difficulties [1]. In more severe cases, paralysis of the respiratory muscles may occur and could be fatal without adequate medical intervention to support breathing. So far, no lasting cure has been developed against this disease and due to its epidemic prone nature, various countries and regions of the world have had a fair share of massive polio outbreaks, especially in Africa and some parts of South-East Asia, where the virus spreads quickly via faeces when adequate personal and environmental hygiene is not maintained [2].
Over the past couple of decades, there have been massive worldwide vaccination campaigns to end the wild polio outbreaks, with great success rates recorded across the globe, amounting to a worldwide drop in the prevalence of polio cases by 99% since its first peak in 1988 [3] when the disease was prevalent in over 125 countries worldwide, to about 20 endemic countries in 2000, and just two countries with Wild Poliovirus (WPV) cases in 2021 [4]. Back in 2012, the type 3WPV strain (WPV3) was eradicated globally, and in the year 2015, the type 2 strain (WPV2) was also completely eradicated worldwide, leaving only the type 1 strain (WPV1) to be battled with [4]. Till date, WPV1 cases have remained confined to the two South Asian countries Pakistan and Afghanistan. The last case of WPV in Africa was reported in 2016, with no other cases detected so far, which led the World Health Organization (WHO) to declare the African continent free of Wild Poliovirus (WPV) in August 2020, signifying a major milestone in global polio eradication efforts [5]. The global WPV eradication journey may be regarded as one of the greatest successes in the history of worldwide infectious disease outbreaks, alongside that of smallpox disease [5].
In the course of administering the Oral Polio Vaccine (OPV), the emergence of Vaccine-derived Poliovirus (VDPV) occurred due to a trend of genetic reversion of the live attenuated virus into a more virulent form capable of causing flaccid paralysis [6]. With time, the prevalence of these reverted virulent strains gradually increased and were found to commonly circulate within specific communities and populations with polio endemic history, thus, giving rise to the term circulating Vaccine-derived Poliovirus (cVDPV) [6].
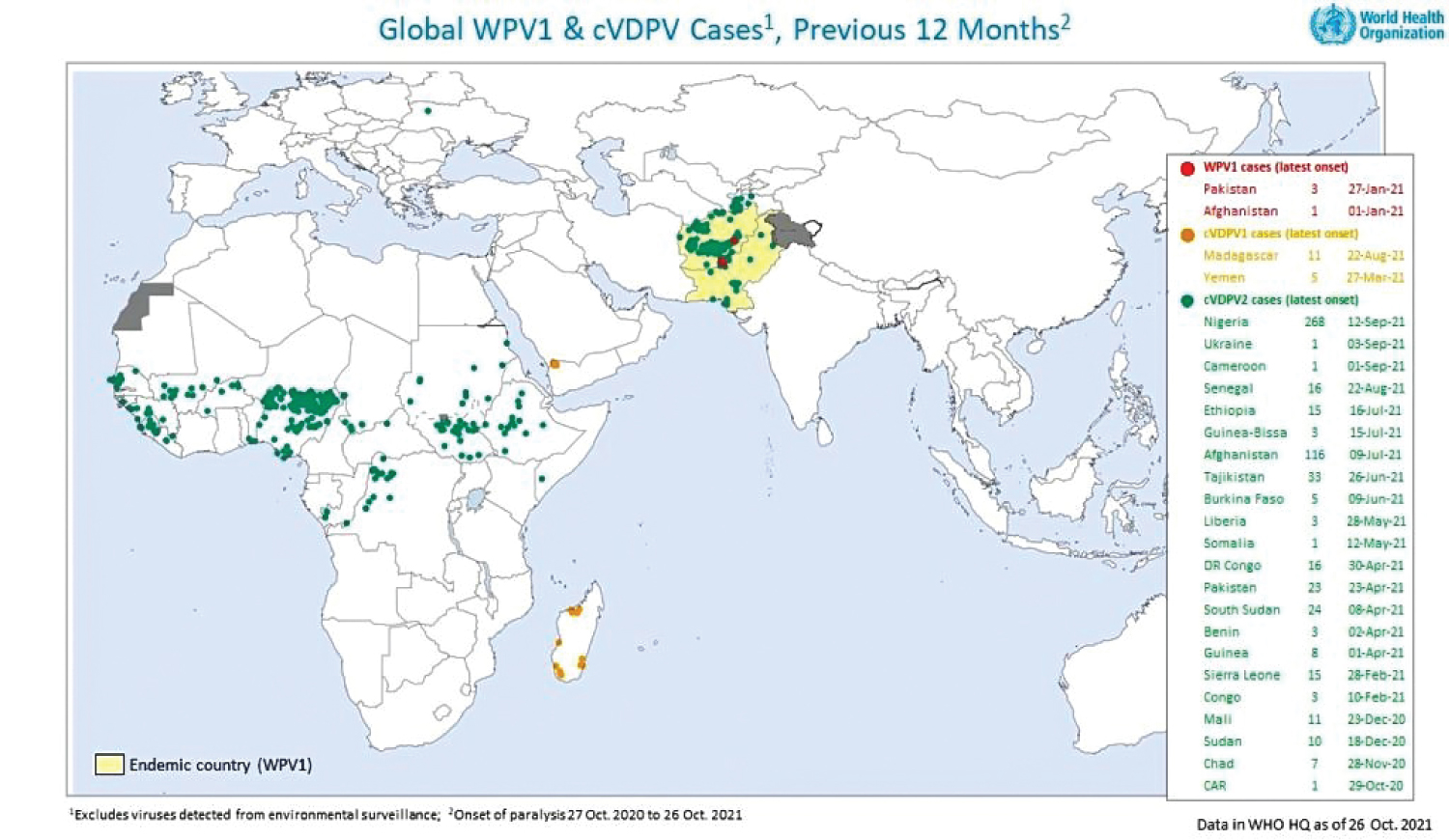 Figure 1: Global Cases of WPV1 and cVDPV as of October 26th, 2021 (Global Polio Eradication Initiative, 2021) [9].
View Figure 1
Figure 1: Global Cases of WPV1 and cVDPV as of October 26th, 2021 (Global Polio Eradication Initiative, 2021) [9].
View Figure 1
The Oral Polio Vaccine (OPV) is known to have certain types such as monovalent OPV (mOPV), bivalent OPV (bOPV) and trivalent OPV (tOPV), which are based on the 3 serotypes of wild poliovirus; type 1, type 2 and type 3 [7]. The type 2 WPV is known to be the most virulent form, hence, it has a higher likelihood of reversion to VDPV when the trivalent OPV containing serotypes 1, 2 and 3 is used. This has been confirmed by the fact that over 94% of cVDPV cases worldwide are cVDPV2, meaning that they emerged from OPVs containing the type 2 strain (mainly tOPV) [8]. So far on a worldwide scale, there are over 599 cases of cVDPV, with 583 of these being cases of cVDPV2 in Africa, while 16 are cases of cVDPV1 in Yemen and Madagascar [9]. A few cases of WPV1 still reside in Pakistan (3 cases) and Afghanistan (1 case), which reflects a progressive drop in WPV1 cases and implies the possibility of completely eradicating wild poliovirus worldwide. Overall, 99% of the current cVDPV and WPV1cases occur in Africa and South Asia respectively, with very few cases in Yemen (Middle East) and Ukraine (Europe) [9].
To reduce the burden of VDPV in Africa where this trend is more common, we recommend a change in the current vaccination schedule being used in regions facing the VDPV challenge, with specific adherence to the vaccination recommendations outlined by the Centers for Disease Control and Prevention (CDC) [10]. Countries utilizing only OPV should completely employ the administration of Inactivated Poliovirus Vaccine (IPV) instead, as it does not contain the type 2 strain and is less likely to revert to VDPV [8]. For developing countries that may find it difficult to cope with the expenses of combining OPV and IPV in their vaccination campaigns, another effective strategy that can be employed is the use of bOPV containing serotypes 1 and 3 instead of the trivalent vaccine format, so as to limit the emergence of cVDPV type 2. In addition, the World Health Organization (WHO) also issued an Emergency Use Listing (EUL) recommendation for utilization of the recently developed novel Oral Polio Vaccine (nOPV2), which is a modified version of the monovalent type 2 OPV (mOPV2) currently being used in low- and middle-income countries (LMICs) [11]. The nOPV2 has undergone rigorous rounds of analysis and clinical trials which have proven its efficacy and genetic stability, with significantly minor chances of reverting to the virulent form, thus, the use of this new vaccine type will help minimize cVDPV outbreaks in LMICs [11].
Implementing the above-mentioned strategies requires concerted efforts by local and international governing bodies, policy makers, health-related organisations, religious and political leaders, non-governmental organisations (NGOs) and vaccination campaign groups. There is a need to strengthen epidemiological research, data acquisition and outbreak surveillance in order to effectively monitor and respond to cVDPV cases in polio-endemic regions, as well as polio-free areas. Advocacy efforts by NGOs must be intensified to bring to fore the importance of maintaining polio eradication efforts despite the prevalent COVID-19 response, to prevent the reemergence of WPV cases in Africa. Partnerships between governing bodies and health-related organisations in terms of funding and training of health workers will serve to strengthen the coverage of vaccination campaigns, and the importance of focal persons, religious leaders and political leaders in local communities must not be overlooked, as they could play a vital role in suppressing vaccine hesitancy among rural community indigenes. Eradicating vaccine-derived polio and maintaining zero WPV status must remain a priority in Africa and on a global scale.
The authors declare no conflicts of interest.
None received by the authors.