Scabies is a skin infection that is a result of direct skin to skin contact and is primarily mediated by close and extended contact with scabies infested person. Scabies occurs worldwide among people of all ages, races, genders and social classes and has been identified as a neglected tropical infectious disease. Globally, it affects more than 130 million people at any time.
The aim of the study was to assess prevalence of scabies and associated factors among primary school children in Raya Alamata District, Tigray, Ethiopia, 2017/2018.
A school based cross-sectional study design was conducted among school children in Raya Alamata District from November 2017 to June in 2018. The sampling technique was multi-stage sampling and sample of the 495 students was selected using simple random sampling technique from the schools. The data was collected using observation (clinical investigation), structured questionnaires and check lists. Data entry, cleaning, editing and analysis were done using SPSS statistical software package version 20. Variables with p-value < 0.25 in the binary logistic regression were selected for final analysis; and final significance was determined at p-value < 0.05.
There were 64 cases of scabies with a prevalence of 12.93%. The multivariable logistic regression shows that family history of scabies AOR = 4.73 (95% CI; (1.52, 14.69)), sharing cloths with others (AOR = 17.61; 95% CI (4.98, 82.64)), sleeping with scabies ill person (AOR = 3.74 [1.11, 12.62] and sharing of beds with (AOR = 4.45 (1.04, 19.02) were significant variables at p-value < = 0.05.
The prevalence of scabies in school children was 12.93% in elementary school children, which is relatively higher compared to other studies which seeks public health attention. Family history of scabies, share cloth with others, sharing of bed to others and Sleeping with scabies ill person was factors related to scabies under adjustment of other variables. This is high burden which seeks public attention.
Scabies, Skin infection, Children, Prevalence, Raya Alamata
AOR: Adjusted Odds Ratio; APSGN: Acute Post streptococcal Glomeruli Nephritis; CHS: College of Health Science; COR-Crude Odds Ratio; CI: Confidence Interval; GBD: Global Burden of Disease; IRB: Institutional Review Board; MDA: Mass Drug Administration; NTD: Neglected Tropical Disease; PI: Principal Investigator; SPSS: Statistical Package Social Science; WASH: Water Sanitation and Hygiene; WHO: World Health Organization
Scabies is a common communicable infection disorder of the skin caused by a mite. This mite, Sarcoptes scabiei is sometimes known as the human itch due to the intense itching caused when the pregnant female mite burrows into the top layer of skin and lays eggs [1]. The common symptom of scabies infestation is pruritus. Disruption of the skin's protective barrier function promotes secondary bacterial infections, which can lead to additional, potentially life-threatening complications [2]. Scabies occurs worldwide among people of all ages, races, genders and social classes and has been identified as a neglected tropical disease (NTD) [3]. Poverty and poor hygiene are factors in the spread of scabies, as they are nearly always associated with overcrowding, sharing of beds, poor hygiene, lack of access to health care, inadequate treatment, primarily mediated by close and extended contact with scabies infested persons and malnutrition [4].
Among family members' scabies is common and frequently observed in institutional places like care centers, nursing homes, schools etc. [5]. Incubation period: Development of the symptoms depends on the infectious status a person who is infected with scabies typically has around 12 mites at any given time [6]. During this time, which may take as long as 4-6 weeks to begin, it is important to remember that an infected person can spread scabies, even if he/she does not have symptoms yet. In a person who has had scabies before, clinical manifestation usually appear much sooner (1-4 days) after exposure. Studies indicated that children who slept on the floor with other children contracted more severe infection and became re-infected in greater proportions. This facilitates skin-to-skin contact and therefore the spread of scabies mites from infested to healthy children [7,8]. The sequel of scabies predisposes affected children to sepsis and other non-supportive invasive infections (e.g. lymphadenopathy, acute post-streptococcal glomeruli nephritis (APSGN) and rheumatic fever [9].
The prevalence rates of scabies varies from country to country, most often it ranges from 0.3% to 46%. Scabies contribute to significant economic costs in national health services in the developed world, due to outbreaks in health institutions and vulnerable communities. However, in resource-poor countries, the sheer burden of scabies infestation, as well as their complications contributes to a major cost on health-care systems [10].
Complications include secondary infections by group of streptococci and acute post-streptococcal glomerulonephritis. Shame, restriction of leisure activities, and stigmatization are common. Treatment of scabies includes a variety of topical compounds, but control at the community level is not an easy task. As ivermectin kills a variety of other parasites, this oral drug is increasingly used for mass treatment. Intervention should address socio-emotional aspects using an integrated approach with professionals from different areas, and the community [11].
In general, poverty and poor hygiene are factors in the spread of scabies, as they are virtually always associated with overcrowding; sharing of beds, poor hygiene, lack of access to health care, inadequate treatment and malnutrition, because of this problem scabies is a common parasitic disease. Moreover, the disruption of the skin's protective barrier function promotes secondary bacterial infections, which can lead to additional, potentially life-threatening complications.
Globally an estimate of more than 300 million cases of scabies occurs every year. Scabies infestations can affect a person from all socioeconomic levels, which knows no preference to age, sex, race or standards of personal hygiene. Anyone who has had contact with the mite can catch scabies. Scabies spreads rapidly through crowded conditions where there is frequent skin-to-skin contact between people, such as hospitals, institutions, child-care facilities, and nursing homes. In young, healthy persons scabies is generally considered to be more of a nuisance than a disease. In elderly persons, or those who are immune compromised, scabies is generally not diagnosed until coetaneous (skin) lesions and symptoms are apparent. Because of the long incubation period, many people can be exposed to scabies before the infested person is diagnosed [12].
Scabies burden is highest in low and middle-income countries of the tropical regions, such as East Asia, Southeast Asia, Oceania, as well as tropical Latin America. It is most commonly seen in children, adolescents and the elderly population. Although similar global epidemiological studies are scarce, scabies is an impediment to that goal, particularly in countries with high prevalence and poor access to effective treatment. Conflicts in areas such as Africa and the Middle East have led to increasing numbers of refugees seeking shelter and protection in Europe. Ethiopia has been particularly affected by natural disasters such as the El Niño weather phenomenon, leading to severe drought and scabies outbreaks [13].
The prevalence of scabies in many populations rises and falls cyclically, peaking every 15-25 years, due to unknown reasons [14]. The International Alliance for the Control of Scabies supported endemic countries including Ethiopia, Fiji and the Solomon Islands in the submission of a dossier and compendium of evidence for scabies [15]. Campaign mass provision of ivermectin is a promising strategy for the control of scabies. Total treatment with ivermectin followed by active case finding was conducted in five communities in the Solomon Islands between 1997 and 2000 and resulted in a significant reduction in the prevalence of both scabies and bacterial skin infections [14,15].
It's listing as a neglected tropical disease by the World Health Organization (WHO) in 2013 recognized the neglect in public and private sector expenditure on this problem, the lack of attention at local, national, and international levels, and the higher incidence of this infection amongst the poor [16].
Scabies has been occurring as infection of human beings for thousands of years. Its distribution is throughout the world, with the occurrence of outbreak during war, famine and overcrowding. Currently there are an estimated of 300 million people infested with scabies. Recent immunological study, such as cross-reactivity with house dust mite allergens and an altered T-helper-1/T-helper-2 pattern contribute to a better understanding of the problem [17].
In Ethiopia drought expansion and increased number of water scarce district with Water, Sanitation and Hygiene/WASH/limited intervention further worsen the disease expansion and severity among the vulnerable. The total of highly affected District in Amhara, Tigray and Oromia reached to 32 district - 24 district in Amhara, 5 in Tigray and 3 in Oromia regions were highly affected, with limited surveillance for scabies, a total number of more than affecting about 250,000 with prevalence more than 15% in some district [18].
There were few studies in school from grade 1- grade 8 in Tigray and our study was refilled the gap on the missed information and our study was also detected the factors affecting the scabies in rural Raya Alamata primary schools. Therefore, this study aimed at determining the prevalence of scabies and associated factors among primary school children in Raya Alamata.
The study was conduct at Raya Alamata District. It is found in southern zone of Tigray Region; Ethiopia and it is Part of the Southern Zone. Raya Alamata District is bordered on the south and west by the Amhara Region, on the northwest by Ofla, and on the northeast by Raya Azebo. Town of Alamata is surrounded by Alamata District. It is about 182 Km south of the city of Mekelle and 600 Km far from capital city of Ethiopia/Addis Ababa. Raya Alamata has a total population of 100,014, of whom 49,506 are men and 50,507 women; 5,341 or 5.34% are urban inhabitants. With an area of 1,952.14 square kilometers, a total of 22,730 households were counted in this district, resulting in an average of 4.4 persons per household [19]. Administratively it is divided into 15 Tibias. Regarding education, there are 58 primary schools that have a total of 23,354 students. These primary schools are hosting for students respectively [20], the study was conducted from Nov, 2017 up to June, 2018.
Prevalence is the number of hosts infected with 1 or more individuals of a particular parasite species (or taxonomic group) divided by the number of hosts examined for that parasite species. It is commonly expressed as a percentage when used descriptively and as a proportion when incorporated into statistics [21].
A School based cross-sectional study was carried out in public primary school children in Raya Alamata district.
The source population includes all primary school children in Raya Alamata rural Tabias.
The study population was primary school children who attend classes in selected sections of selected schools during the data collection period, in Raya Alamata district.
Inclusion criteria: All primary school children were included in the study.
Exclusion criteria: Primary school students who are absent from school for two consecutive days during data collection period excluded.
Sample size determination: The sample size was using single proportion for finite population with 95% confidence interval, marginal error (d) of 5% and the prevalence of the scabies among primary school children in Cameroonian (with overall 338 scabietic participants) was 17.8% [22], so this proportion was used to determine the sample size. To compensate for non-response, 10% of the sample was added.
n = sample size from infinite population.
Z = the standard score (critical value) corresponding to 95% confidence level = 1.96.
D = the proportion of sampling error between the sample and the population = 5% (0.05).
p = To calculate the sample size we used the study conducted in Cameroon at primary school children 1,902 participants were used from this the prevalence of scabies was found to be 338 (17.8%).
The total sample size was 225, with design effect 2, 10% non-response rate the final sample size was: n = (225) x 2 = 450 + 45 = 495.
Sampling techniques and procedure: The sampling technique used was multi stage. First 7 kebelles was selected from Raya Alamata District by random sampling. Second from the selected kebels 15 schools was selected by simple random sampling and followed by selection of 38 sections from the 152 sections by random sampling and proportional allocation to size was done to each selected section. Finally, students were selected by systematic random sampling from their class rosters. The sampling width was taken by proportion formula the total student in the sections divided by total sample size that is 2458/495 = 5, and then every 5th in the roster was included in the study (Figure 1).
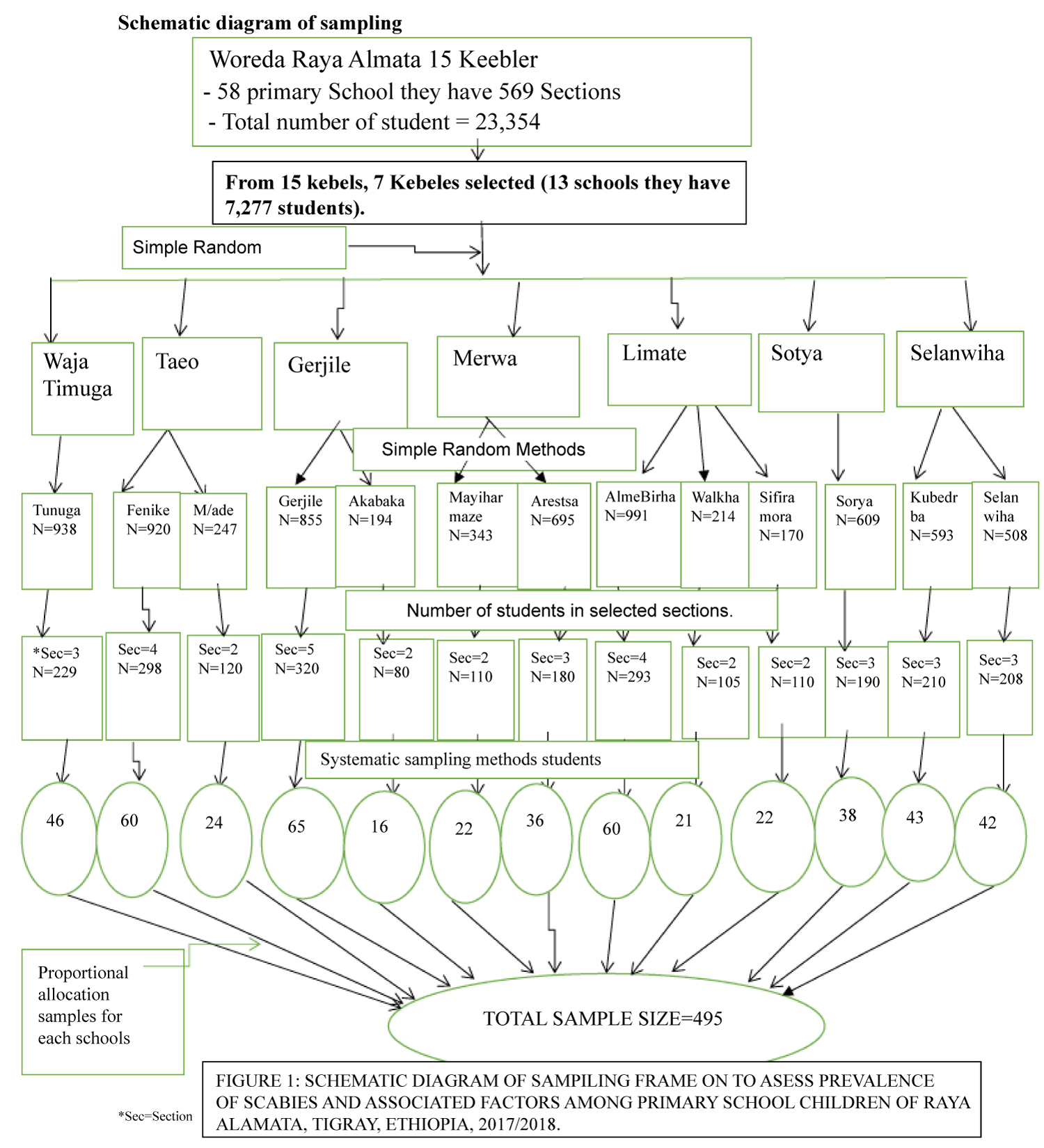 Figure 1: Schematic diagram of sampiling frame on to asess prevalence of scabies and associated factors among primary school children of Raya Alamata, Tigray, Ethiopia, 2017/2018.
View Figure 1
Figure 1: Schematic diagram of sampiling frame on to asess prevalence of scabies and associated factors among primary school children of Raya Alamata, Tigray, Ethiopia, 2017/2018.
View Figure 1
➢ Scabies
Socio-demographic data of the child
➢ Age
➢ Sex
➢ Religion
➢ Family size
➢ Income of house hold
➢ Sleeping with scabies cases
➢ Having animals at home
Personal hygiene factors
➢ Usage of soap on bath
➢ History of itching
➢ Shortening of nail
Living condition factors
➢ Sharing bed/mad/floor
➢ Water shortage
➢ Sharing cloth with others
Knowledge of scabies
➢ Transmission of scabies
➢ prevention method of scabies
Scabies: Development of skin lesions between the fingers or on the volar wrists, elbows, scalp and penis and with itching at night.
Poor personal hygiene: A student who bath more than a week or who can't change cloth within a week or who can't wash hand after toilet or before eating food.
Good level knowledge: A child who has an awareness on transmission and prevention method of scabies.
Poor level of knowledge: A child who don`t have an awareness either of two transmission and prevention method of scabies.
A structured interviewer questionnaire was developed by reviewing different literatures. The questionnaire addressed three issues, namely: Socio-demographic data of the child, personal hygiene factors and living condition factors. The data was collected using clinical investigation (observation) and a structured interviewer administered questionnaires. Ten data collectors who were registered nurses were trained by a dermatologist for 5 days on how to diagnose scabies and also training was given on how to take informed consent from parents, assent form from students, approach participants and ensure ethical procedures including practical sessions at Alamata general hospital. Another 1-degree holder nurse and 1 health officer were assigned as supervisors to check for the daily activity, consistency and completeness of the questionnaire and to give appropriate support during the data collection process.
To collect quality data, the questionnaire was translated to local Tigrigna language by experts. A pre-test was conducted at 10% of the sample size (50 students) in Mokoni district two weeks before the actual data collection period to test variability, and the checklist was assessed for clarity, completeness and other corrections were done accordingly. Training was given to data collectors for five days before data collection, and the questionnaire was checked for completeness by the investigator. In each day of the data collection there was close supervision by the supervisors and principal researcher to support and monitor the data collection process by the data collectors. After data collection, each questionnaire was checked for completeness to commence data entry process on daily basis.
Completed questionnaires were coded and entered to SPSS version 20 statistical software package for analysis. Categorical variables were presented using frequencies and percentages. Continuous variables were checked for their normality using histogram chart. Normally distributed continuous variable like age was reported by mean and standard deviation. A binary logistic regression was used to assess magnitude, relationships and associations between independent variables and outcome variables. All variables with p-value < 0.25 (odds ratio not crossed 1) were selected for multivariable analysis and statistical significance was declared at p < 0.05 (odds ratio not crossed 1) The Hosmer-Lemeshow test was done and p-value was 0.38, which means that Hosmer-Lemeshow test is not statistically significant and therefore the model adequately fitted.
Ethical clearance was obtained from Institutional Review Board (IRB) of Mekelle University, College of Health Science. Support letter was obtained from School of nursing and official letter of permission was requested from Tigray regional health bureau and Raya Alamata District Education Office. The purpose and significance of the study were explained to the study participants and they were assured that they had the right to withdraw from the study at any stage. Written consents form parent children and assent for the children were obtained before the data collection. Then, parents and their respective children were invited by the teachers to come to the school where their child was learned. Detailed information about the child was obtained from his/her parents. Identified scabies cases were linked to health extension workers and district Health Office for treatment purpose. In addition to this, students were sensitized to adhere proper sanitation hygiene practices on their daily basis. Similarly, school directors were also informed to monitor their students' hygiene and provide necessary sanitation and hygiene facilities at their schools. Confidentiality of the study participant was maintained throughout the study.
The results will be submitted to Mekelle University Department of Nursing, Regional Health Bureau, Raya Alamata district Health Office and Tigray Public hospitals; presenting at the different workshops and so that it can be used as a source of information for possible planning and implementation of health intervention. Moreover, efforts were done to publish the findings of the study and disseminated through different journals and scientific publications.
A total of 495 students participated in the study with a response rate of 100%. About 56.28% of the respondents were males and 53.94% of the students were from grade 5 to 8. About 288 (66.06%) of the students have large family size, i.e., equal or greater than 5, as shown in the Table 1 (Figure 2).
Table 1: Socio-demographics characteristics of students in selected primary schools of Raya Alamata district, June 2018 (n = 495). View Table 1
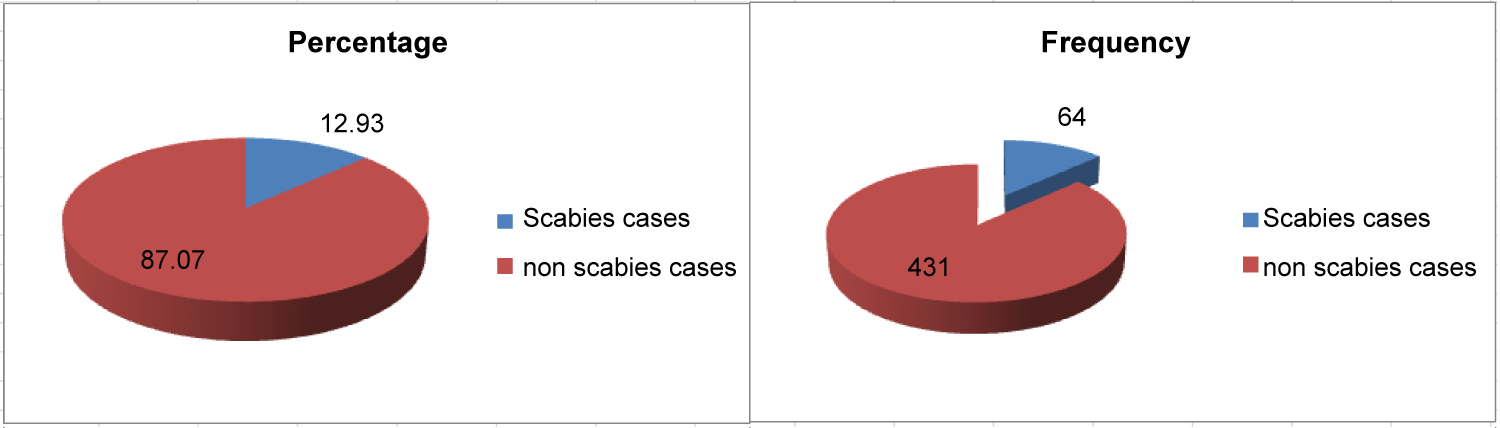 Figure 2: Prevalence of scabies among primary school students in Raya Alamata District June 2018, (n + = 495).
View Figure 2
Figure 2: Prevalence of scabies among primary school students in Raya Alamata District June 2018, (n + = 495).
View Figure 2
Personal hygiene: About 71.3% of the students take shower within a week but there are students who take shower 7-14 days, 15-30 days and even more than a month with a magnitude of 3.6%, 20% and 5.1% respectively. Around 65% of the students take shower with soap but the rest took shower with water only. About 98.8% of the students wash their clothes and only 54.7% shorten their nail when it grows more. About 48.1% of the students change their clothes every week and 40% change every two weeks as it shown in Table 2.
Table 2: Personal hygiene among primary school students in Raya Alamata District, June, 2018 (n = 495). View Table 2
Living conditions of students: About 62.4% of the student's family share same house with their animals. Significant number of students that is 36.4% do not get adequate water supply for their daily needs. About 54.1% of the interviewed students use source of water from pipe water followed by spring water of 17.4%. About 57.2% of the students have less than half an hour of walk distance from their home. About 22.6% of the students have practice of sleeping with scabies ill person and 30.1% of the students share beds for others as it shown in Table 3.
Table 3: Living condition characteristics of primary school students in Raya Alamata district, June, 2018 (n = 495). View Table 3
Associated factors of scabies in primary school children: There were 64 (12.93%) confirmed scabies cases among the screened elementary students. In the bivariate analysis age of student, religion on. Occupation of head of household (HH), income status of the household, family history of scabies was statistically significant. Frequency of shower, detergent used for shower, bathed with someone else in previous 6-week, share of cloth with others, shortening of nail regularly, change of cloth frequency were also significant associations with scabies. availability of water supply, source of home water, distance of source to home, sleeping with scabies ill person, sharing bed with others and know scabies transmission were associated with the confirmed scabies in the crude OR association.
The multivariable logistic regression shows that family history of scabies AOR = 4.73 (95% CI; (1.52, 14.69)), sharing cloths with others (AOR = 17.61; 95% CI (4.98, 82.64)), sleeping with scabies ill person (AOR = 3.74 (1.11, 12.62)) and sharing of beds with (AOR = 4.45 (1.04, 19.02)) were significant variables at p-value ≤ 0.05 (Table 4).
Table 4: Bivariate and multivariable logistic regression analysis result for significant variables (p ≤ 0.25) in bivariate analysis a study of scabies among school children in the primary schools of Raya Alamata district, June 2018 (n = 495). View Table 4
Hosmer-Lemeshow test was done and p-value was 0.38, which indicates the model is adequately fitted.
From the school based cross sectional study there were 64 (12.93%) confirmed scabies cases. This is lower compared to the study of a population-based survey in the Solomon Islands which reported a total un-weighted prevalence of scabies of 19.2% (95% confidence interval [CI] 17.5-21.0) [23]. These differences might be due to cultural and economic situations among the communities. It is also lower than that reported in a study conducted in Cameron school children shows out of 1902 study participants 338 (17.8%) were diagnosed with scabies [22]. This study also revealed lower prevalence compared to the cross-sectional study done in Amhara region, Ethiopia that showed that Majority of 543 (23%) scabies cases were occurred from Gashena town the younger age group 6-14 years was more affected by the disease with an age specific attack rate (ASAR) of 6%. This difference might be due to variation of water, sanitation and hygiene (WASH) related infrastructures, knowledge and cultural differences. Similarly, it might also due to time of study differences, since as the study time is earlier study participants may get sensitization about hygiene and sanitation.
However, in this study prevalence is higher compared to the research scabies among primary school children in Egypt which were 92 cases of scabies with a prevalence of 4.4% [24]. Similarly, it is higher compared to another study carried out in Kirkuk in displaced families' shows that 153 scabies cases be identifies out of 1693 participants' during the study period, with overall incidence rate of 9.33%, 9.88% in male and 8.73% in female [25]. These variations of prevalence of scabies among these studies might be also due to awareness differences on hygiene and sanitation as well as availability of infrastructures of WASH among the study populations.
The multivariable logistic regression shows that significant association. The odds of individuals with scabies were individuals that have family history of scabies were almost five times higher among scabies cases compared to participants who had no family history all other predictors being fixed at AOR = 4.73 (95% CI; (1.52, 14.69). This study is similar with the study in Egyptian shows significant variations in the risk of scabies infestation by factors such as family history of itchy rash [26]. This is because if there was family history of scabies the transmission rate might be high since there is probability of contact within the member of the family.
The other associated predictor was sharing cloths with others. The odds of individuals that share clothes with others were almost 18 times higher among scabies cases compared to students who did not share their cloths all other predictors being fixed with AOR = 17.61; 95% CI [4.98, 82.64]. This study is consistent with the study in Egyptian shows significant variations in the risk of scabies infestation by factors such as sharing clothes with others [26]. Similarly, it has supported by another study in Gondar that showed people who share close from ill person were 2.76 (95% CI = 1.04-7.41) times more likely to develop scabies, though their difference strength of association [27]. This is because sharing of close also shares the parasite to transmit from ill to non-ill person.
Sleeping with scabies ill person was also significantly associated with scabies. The odds of individuals that sleep with scabies ill person were almost 4 times higher among students who don't sleep with a person who had scabies all other predictors being fixed with (AOR = 3.74 [1.11, 12.62]. This is similar with study done in Amhara region, Ethiopia that showed sleeping with contacted scabies case (AOR: 25.3, 95% CI: 8.7-73.4, p: 0.0001) [28]. Additionally it has supported by another study in Gondar that showed individuals who had close contact with ill person were 5.37 (95% CI = 1.84-17.6) times more likely to develop disease scabies [28]. This is because close contact/sleeping with scabies cases one of the principal ways of transmission of scabies from scabies cases to healthy one.
Sharing of beds to others was significantly associated with scabies. The odds of scabies were almost 4 times higher among individuals that share bed to others compared to those who do not share to others all other predictors being fixed with (AOR = 4.45 (1.04, 19.02). This was similar with the study in Gondar indicated that people who share close from ill person were 2.76 (95% CI = 1.04-7.41) times more likely to develop scabies [28]. This is because sharing of bed can reside the parasite in the linen sheet and blankets that can have potential to transmit to healthy once.
The prevalence of scabies in primary school children are relatively higher compared to others which seeks public health attention family history of scabies, sharing clothes with others, Sleeping with a person who had scabies and sharing bed to others were significantly associated with scabies.
From overall findings of the study the following points are recommended to responsible bodies.
WASH facilities should be availed in the schools as well at their homes by Tigray water resource bureau and water resource office of Raya Alamata District.
Improve surveillance approach for early case detection and to provide treatment for scabies cases family to the community to create awareness regarding scabies mode of transmission and control mechanisms.
Strong and intensive health education on personal hygiene and sanitation should be provided by health extension workers and school teachers to avoid sharing clothes with others, sleeping with scabies ill person and sharing of bed to others.
• Routine school-based scabies screening should be undertaken by PHCU nurses.
➢ Advice should be given to avoid sharing of cloths their children with the person who have scabies.
➢ Cloths should be made clean and socked with hot water and/or other chemicals.
The researchers should conduct further study on scabies both at community and facility based.
Ethical clearance was obtained from Institutional Review Board (IRB) of Mekelle University, College of Health Science. Support letters was obtained from School of nursing and official letter of permission was requested from Tigray regional health bureau and Raya Alamata District Education office. The purpose and significance of the study was explained to the study participants and they were assured that they had the right to withdraw from the study at any stage. Written consents form parent children and assent for the children was obtained before the data collection, in which parents were invited by the teachers and their respective children to come school where their child was learned. Detail information about the child was obtained from this/her parents. Identified scabies cases were linked to health extension workers and district health office for treatment purpose. In addition to this, students were sensitized to adhere proper sanitation hygiene practices on their daily basis. Similarly, school directors were also informed to monitor their students' hygiene and provide necessary sanitation and hygiene facilities at their school. Confidentiality of the study participant was maintained throughout the study.
All authors agreed to publish in this journal.
All necessary data are available in secure computer with key locked by the author.
There is no any computing interest of authors regarding this article.
Mekelle University College of health sciences.
Author's Contributions ST: MT: AA: Had taken a principal role in the conception of ideas, developing methodologies, data collection, analyses and write up of the article. All authors read and approved the manuscript. Author 1 ST: Initiated the research, wrote the research proposal, conducted the research, did data entry and analysis and wrote the manuscript. Author 2 MT: Involved had taken a principal role in the conception of ideas, developing methodologies, data collection, analyses and write up of the article. All authors read and approved the manuscript. Author 3 AA: conducted the research, did data entry and analysis and wrote the manuscript.
Author 4 TB & Author 5 HH were supervisors for the research work.
I would like to give my thankfulness to Mekelle University, school of nursing for letting and financial support me to explore a lot of research methodologies and principles on how to write research thesis in a very fine way.
I also want to acknowledge to Tigray regional health bureau for giving me a chance to enroll in this program and have an opportunity to upgrade myself in nursing specialty.
I am also grateful to, Alamata district health office and respective schools where the data collections undergone for providing me the necessary information and cooperative support.
My deepest gratitude also goes to the data collectors, supervisors, my advisors and participants without whom this thesis would not be realized.