
The world is facing an unprecedented test by an enemy, a novel and deadly enemy, the COVID-19 pandemic. As COVID-19 continues to spread all around the world, social, political and serious economic consequences await this planet. After the introduction and a brief epidemiological summary, this article discusses the threat that is COVID-19 to major global urban centers. The impact of COVID-19 across the globe is particularly inimitable and more so in major global urban centers for several reasons including these being international hot spot destinations, global financial hubs attractive for entrepreneurs from across the globe, densely populated areas, as well as having higher percentages of low-income individuals and families.
COVID-19, Epidemiology, Virus, Infectious diseases, Pandemic, Urban centers
COVID-19: Coronavirus Disease 2019; SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; PPE: Personal Protective Equipment; JFK: John F Kennedy; DC.: District of Columbia
Coronavirus disease 2019 (COVID-19) is an infectious disease which is caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) [1]. The novel coronavirus belongs to family Coronaviridae of single-stranded RNA viruses that are protected by a lipid envelope covered with club-like projections.
Humans who are infected with novel coronavirus experience fever, tiredness, dry cough, and shortness of breath. Other symptoms include muscle pain, abdominal pain, sputum production, diarrhea, sore throat, and loss of smell or taste [2,3]. It is important to point out that despite being infectious and capable of transmitting COVID-19, certain infected individuals show no symptoms. Even though most people recover from the disease without needing special treatment, individuals who are older and those with underlying medical problems such as cancer, diabetes, cardiovascular disease, and chronic respiratory disease are more likely to develop serious illness, requiring mechanical ventilation to aid breathing. Without mechanical ventilation to aid breathing, COVID-19 is highly fetal in individuals who are seriously ill as they are not capable of breathing on their own. Even with mechanical ventilation, COVID-19 still presents a real threat to the lives of the elderly and people with compromised immune systems. The disease was first identified in 2019 in Wuhan (Hubei province, China) [4] and quickly spread all over the world, ravaging especially urban centers, travel destinations hubs, and densely populated areas.
The incubation period, that is the time between catching the virus and beginning to have symptoms of the disease, is estimated to range from 1-14 days, most commonly around five days [5]. The situation was still fluid by the end of March and beginning of April 2020, and as more data became available, about 2 weeks was accepted worldwide as the most common incubation period [6,7]. It has also been reported however, that the incubation period may last as long as 27 days in certain individuals. A 70-year-old man in China's Hubei province was infected with COVID-19 but did not show symptoms until 27 days later [8]. A longer incubation period could complicate efforts to contain the spread of the pandemic which had infected more than 700,000 people and killed more than 33,000 people globally by March 29, 2020. These numbers were still rapidly increasing [9] such that two days later (April 1, 2020), more than 921,000 people had been infected and more than 46,200 people had been killed globally.
In a little over three months period, the virus had already spread to all the continents and by March 29, 2020, 177 countries had reported cases [9]. In China where it all began, there had been over 82,000 cases reported and over 3,300 deaths by March 29, 2020 [9]. Several European countries especially Italy and Spain saw unprecedented speed of the spread and the influx of patients overwhelmed corresponding health care systems. By March 29, 2020, The combined numbers for Italy and Spain were more than 177,000 confirmed cases and a total of more than 17,400 confirmed deaths [9]. The United States of America became the epicenter of this pandemic with more than 142,000 confirmed cases by March 29, 2020 [9]. By the morning of March 31, 2020, there were over 164,000 confirmed infection cases in the United States, which was the highest in a single country globally at the time [10]. These numbers were increasing quite rapidly around the world as more and more tests were administered. On the morning of March 31, 2020, COVID-19 cases were reported in 179 countries [10]. The combined numbers for Italy and Spain had increased from about 177,000 [9,11] to over 196,000 [10] confirmed infection cases in just two days. The death toll for both countries (Spain and Italy) increased from about 7,400 [9] to more than 19,700 [10], which is more than double in just two days (March 29 - March 31, 2020) [10,11]. Economies around the world had started taking a hit as more and more companies closed their doors and laid off workers [12-14]. Several western governments came up with huge economic packages to help businesses and individuals who were facing financial hardships as a result of COVID-19 [15-19]. Numbers of infected people continued to accelerate at an alarming speed; for example, by the evening of April 2, 2020, the number of confirmed infected individuals had reached more than 1,014,000 with more than 53,000 deaths globally [20]. The United States continued to be the epicenter of the pandemic such that more than 245,000 cases with more than 5,900 deaths had been reported by the evening of April 2, 2020 [20]. The same day, the state of Louisiana reported a staggering 2,700 new cases in just 24 hours [21]. Two days later (April 4, 2020), confirmed cases reached more than 1,200,000 with more than 65,000 deaths globally. In the United States, confirmed cases went over 311,000 with more than 8,500 deaths [22,23]. In addition, The United States reported a staggering 1,224 deaths in just 24 hours [11,24] followed by 1,344 deaths on Saturday, April 4, 2020 [11,25]. By the end of the day on April 8, 2020, the number of infected cases had reached over 1,484,000 with more than 88,000 deaths globally [26]. These numbers increased to over 1,696,000 with more than 102,000 deaths worldwide on April 10, 2020 [27]. The United states continued to get hit hard as the number of cases reached over 501,000 cases with more than 18,000 deaths [27]. It is important to mention that with at least 161,807 confirmed cases on April 10, 2020, New York state now had more confirmed coronavirus cases than any country outside of the United States [28]. A few days later, on the morning of April 16, 2020, the total number of infection cases had reached a staggering 2,081,969 with 138,487 deaths globally [29]. In the United States, 639,664 cases with over 30,990 deaths had been reported [29].
The novel coronavirus infected people of all ages and all classes around the world; the old, the young, the rich and the poor [30,31]. When it comes to the mortality rate in general, elderly people are at a higher risk over young people, and individuals with underlying medical conditions are at a higher risk over healthy individuals of the same age [30-33]. It has now become increasingly clear that COVID-19 also discriminates by sex, with females who got infected being less likely to die from the disease. The observation was first made in China where one study found a fatality rate of 2.8% in men and only 1.7% in women [30]. The same pattern was observed by other countries including in USA, France, Germany, South Korea, Iran, Italy, and Spain [34,35]. Key biological differences in the way men and women fight off infections could be one key piece of context as to why COVID-19 is more fetal in men than in women. It is known already that women usually tend to mount a robust immune response. This is in part because women have two X chromosomes, and the X chromosome happens to contain most of the genes related to the immune system. Consequently, two X chromosomes instead of one also have a broader diversity of immune responses [35,36].
Multiple data sources, maps, and projections show that major metropolitan areas are bearing the brunt of COVID-19, as it quickly spreads across Europe, North America, and the rest of the world. COVID-19 is especially threatening to major global cities for several reasons some which are examined following. As infectious people who might not even know they are infected because of lack of symptoms flew from destination to destination so did COVID-19. People from all over the world land at major international airports in major cities such as New York, London, Los Angeles, Houston, Rome, Paris, Madrid, and others on an hourly basis. This kind of influx cruelly contributed to a quick COVID-19 spread early on before individual countries started closing international borders, airports and cancelling most non-essential travels. The world is so connected now more than ever, we are all linked and what affects one country will more than ever before affect other countries directly or indirectly. The vulnerability of major metropolis around the world to COVID-19 spread becomes even more obvious when we think about global business centers and tourism. Major cities that are attractive to tourists are equally attractive to major global businesses, international conferences, and major sporting events. Global major cities are appealing to investors for several reasons including these being particularly strategic locations to leading financial institutions, reputed stock exchanges, a dense concentration of public and private banks, trading and insurance companies, and corporate headquarters for investment banks. These hubs are likewise eye-catching to global professionals and major global businesses because they are equipped with first-class infrastructure, communications, commercial systems, and there is a transparent and sound legal and regulatory regime backed by a stable political system [37-39]. In addition, such cities are favorable destinations for professionals because of the high living standards they offer along with immense growth opportunities [37-39]. Consequently, the probability of both infected and non-infected individual from different parts of the world finding themselves in these major global city centers all at once is very high. As these international travelers went back and forth in and out of these major centers, so did COVID-19. New York is especially vulnerable as the JFK international airport is one of the busiest international airports in the world.
The percentage of the world's population living in urban areas continues to increase exponentially. It is estimated that by 2025, about 70% of the global population will live in urban areas and major metropolis. Crowded urban areas in developing and industrialized countries are uniquely vulnerable to public health crises such as COVID-19 and they face daunting challenges in surveillance, response, public communication, and locate and isolate [40]. In terms of infectious diseases such as COVID-19, the risk in urban centers is closely related to the characteristics of cities. Take an example of a city such as Lagos, Nigeria or New York. Lagos is the largest city in Nigeria with over 21 million people [41,42]. The city of New York is the most populous city in the United States. With an estimated 2018 population of 8,398,748 distributed over about 302.6 square miles (784 km2), New York is also the most densely populated major city in the United States [43]. Because there are so many people in a city such as New York, people are constantly in close proximity to each other: Passing near each other on the streets, travelling together in buses and subways, working together, enjoying sport or cultural events together, eating together in restaurants, and drinking together in bars [44]. Consequently, social distancing and the closure on non-essential businesses and events around the world became necessary in order to stop the spread of COVID-19. When a disease is communicated from person to person, particularly if it is air-borne or transmitted through casual contacts, it will normally be communicated faster and to more people in a city than in a rural area. Urbanization has thus become one of the factors that enhance the spread of diseases in today's world. In a city, an outbreak can soon become an epidemic, and as cities such as New York have good transportation systems linking to other cities, the epidemic quickly becomes a pandemic [44]. Wuhan and New York City responses to COVID-19 pandemic illustrates some of the new challenges and creative response strategies that will increasingly be needed in most cities worldwide in the fight against similar pandemics. A 1000-bed hospital was built in just 10 days in Wuhan, china [45] and in New York, makeshift hospitals were set up in order to try and deal with the influx of COVID-19 patients as well as patients with other types of diseases [46,47].
Because of having many low-income individuals/ families, urban centers can act as centers for disease transmission which can accelerate the spread of pathogens. We have seen this in US cities such as New York, New Orleans, Chicago, Detroit, and others. In addition, social inequality and poverty can increase individual susceptibility to infection significantly. Many low-income individuals and members of low-income families have weakened immune systems and that could play a major role in increasing transmission and mortality rates [48-50]. In addition, communities such as the African American community which are mostly concentrated in city centers might be more exposed because many held low-wage or essential jobs, such as food service, public transit and health care, that required them to continue to interact with the public [51]. Dorianne Mason, the director of health equity at the National Women's Law Center in USA correctly pointed out that this outbreak was exposing the deep structural inequities that make communities pushed to the margins more vulnerable to health crises in good times and in bad [51].
According to the Washington post article published on April 7, 2020, an analysis of available data and census demographics showed that US counties that are majority-black and these are usually urban counties, had three times the rate of infections and almost six times the rate of deaths as counties where white residents are in the majority [51] (Figure 1).
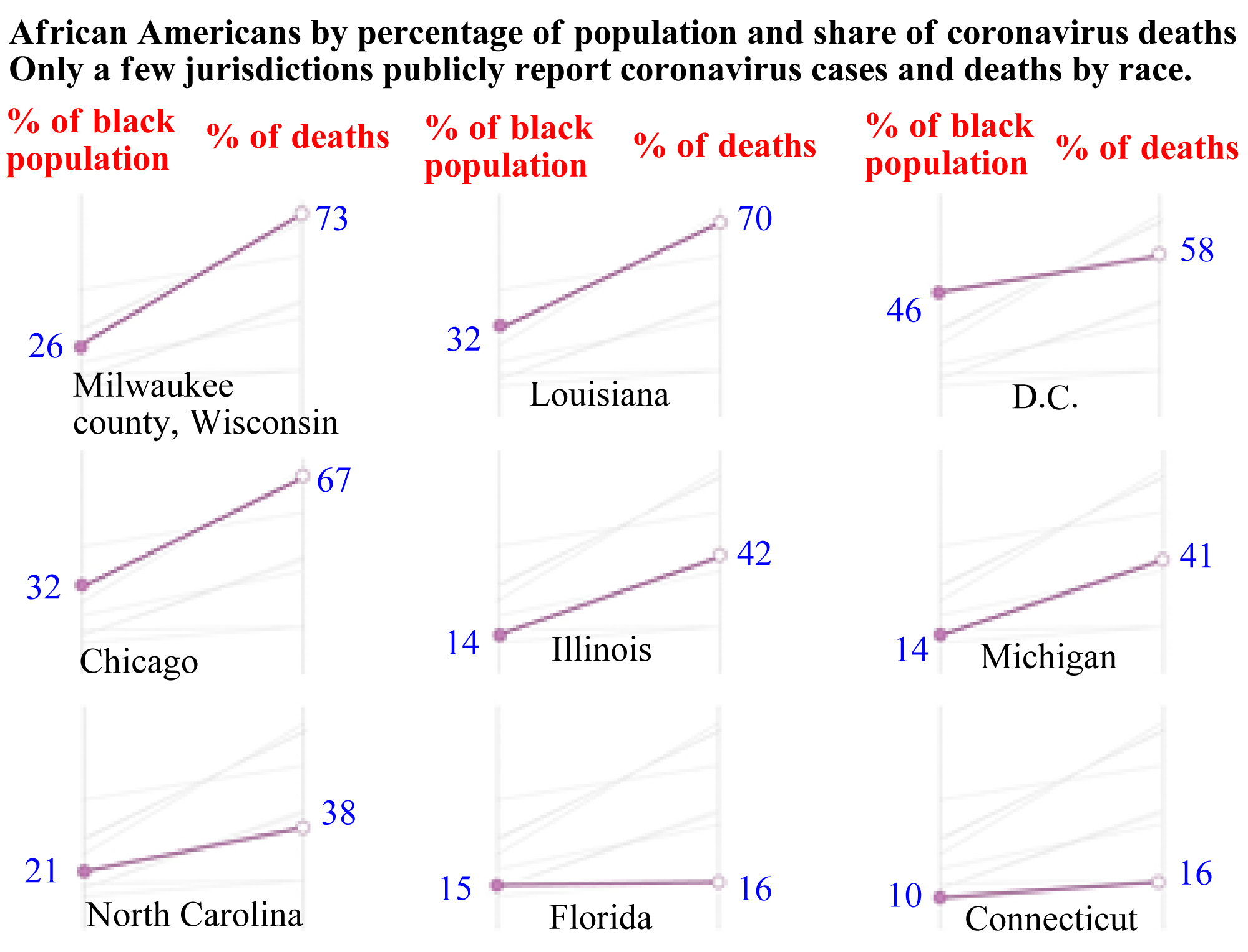 Figure 1: African Americans by percentage of population and share of COVID-19 deaths in selected US locations by April 7, 2020 [51].
View Figure 1
Figure 1: African Americans by percentage of population and share of COVID-19 deaths in selected US locations by April 7, 2020 [51].
View Figure 1
In Milwaukee county [52], the largest city in the state of Wisconsin, African Americans account for about 70% of the dead but only 26% of the population as seen in Figure1. This picture is similar in Louisiana state, where 70% of the people who had died were black, even though African Americans made up only 32% of the state's population [53]. In Michigan state, African Americans accounted for 33% of reported cases and about 40% of deaths, despite comprising only 14% of the population. Michigan state does not offer a breakdown of race by county or city, but more than a quarter of deaths occurred in Detroit, the largest city in the state of Michigan, where African Americans make up 79% of the population [54]. In Illinois [55], a disparity nearly identical to Michigan's exists at the state level, but the picture becomes clear when looking at data just from Chicago, again the largest city in the state of Illinois, where black residents have died at a rate six times that of white residents [51,56].
Countries around the world put in place strict measures in order to curb the spread of COVID-19. The common ones include stay-home for as much as possible and social distancing. These measures are difficult if not impossible for many low-income individuals in urban centers around the world. Think of a low-income family of 5 living in 1-bedroom or 2-bedroom apartment in New York, Detroit, Chicago, or New Orleans. How can this family practice social distancing? This is dangerous especially when one or more household members are still required to go to work daily and can potentially bring the virus back to the house.
In developing countries, a high percentage of people in urban centers earn their living on a day to day basis. This means that if a man does not go to work on a given day, his family might have nothing to eat by the end of the day. Most governments in developing countries will not be able to supply cash or free food to these individuals and families. The world has overcome so many threats over centuries. However, if the current situation does not change fast, many people in urban centers especially in developing countries might start dying not because of COVID-19, but because of other reasons, including food shortage related factors.
COVID-19 is a Pandemic that has shown to greatly increase morbidity and mortality over a wide geographic area. The pandemic has and continues to cause significant economic, social, and political disruption around the globe. Today, the international community has made progress toward preparing for and mitigating the impacts of pandemics. However, as COVID-19 numbers (confirmed infection cases and deaths) continue to rise rapidly, it becomes obvious that the world will continue to face challenges with new and previously unknown pandemics. There still exist significant gaps and challenges in global pandemic preparedness. The impact of COVID-19 is felt across the globe and more intensely so in major global cities. Early on, places like New York or Italy struggled to even have enough ventilators and/or Personal Protective Equipment (PPE) for health care workers who treat COVID-19 patients. This pandemic will one day be no more; the world will overcome this; until then, COVID-19 presents a deadly threat to humans especially in major global cities and it should be taken seriously by all of us.
Sincere appreciation goes to Sandra C. C. Twibanire for a great discussion on COVID-19.