Antiretroviral therapy (ART) restores immune function and reduces HIV-related adverse outcomes. Patients on ART are recommended to periodic monitoring to ensure effective and durable treatment outcomes. Treatment failure is the main indication for ART switching and assessed by criteria used to define virologic, immunologic or clinical failure.
The aim of the study was to determine incidence and clinical predictors of ART failure in ART user adult HIV patients in North West Ethiopia.
A retrospective follow up study was conducted from June 1, to August 30, 2018 to determine the incidence and associated factors with first line ART failure among 315 adult ART users who started treatment between January 1, 2012 and December 31, 2017. Data regarding patients' socio-demographics, clinical characteristics, and treatment-related information were collected through review of their medical charts. Data were analyzed using SPSS version 21. Bi-variable and multivariable Cox proportional hazard model was used to identify predictors of treatment failure. P ≤ 0.05 was used to declare association.
Among 315 patients enrolled, 185 (59%) were females. Median age was 35 years (IQR 30-40 years). During 13,374 person-months of follow up, 32 (10.2%) persons failed their first line ART regimen at incidence of 2.39 failures per 1000 person-months of observation. Inadequate adherence (AHR (95% CI) = 6.01 (2.543-14.661), P value = 0.001), WHO clinical stage 3 and 4 (AHR (95% CI) = 4.471 (1.625-12.301), P value = 0.004), low base line BMI (AHR (95% CI) = 3.343 (1.552-7.201), P value = 0.002), and presence of ART drug toxicities (AHR (95% CI) = 2.470 (1.013-5.594), P value = 0.03) were found to be significant predictors of ART failure.
Incidence of ART failure in ART clinic, University of Gondar hospital was considerable. Inadequate adherence was found to be the strongest predictor of first line ART failure. Close follow up and focused care is important to identify early treatment failure using the available resources.
Antiretroviral drugs, Treatment failure, Adherence
Antiretroviral therapy restores immune function and reduces HIV-related adverse outcomes. It has transformed HIV/AIDS from inevitably fatal disease to chronic, manageable illness [1,2]. Patients on ART are recommended to periodic monitoring and evaluation to ensure effective and durable treatment outcome [1,2]. Over the past decade, there has been an unparalleled effort to provide access to antiretroviral therapy (ART) for HIV-infected individuals in sub-Saharan Africa, the region with the highest HIV burden [2]. In Sub-Saharan Africa, observations on effectiveness of ART showed encouraging results despite concerns in durability of therapeutic response [2-4].
ART failure can be defined as progression of disease after initiation of ART. It occurs in the form of virologic failure, immunologic failure, or clinical failure [2]. Patients unnecessarily remained in failed regimen experienced higher morbidity and mortality, and failed regimen might threaten successful ART program [2]. Options for second-line ART regimen are limited in African countries due to constraint resources.
African studies reported incidence of ART failure ranged from 0.96-5.88 per 100 person-year of observation (PYO) [3-5]. Documented predictors of treatment failure in Africa include, but not restricted to, younger or older age, male gender, low educational status, high pretreatment viral load, low pretreatment CD4 count, low base line BMI, advanced HIV disease (WHO clinical stage 3 and 4), presence of opportunistic infections, TB co-infection, type of ART regimen, ART drug toxicities, drug-drug interactions, and inadequate ART adherence [3-9].
In Ethiopia, ART scale-up began in 2005, and ART access to eligible individuals rose to 59% by the year 2017 [2,10,11]. First line ART regimen in Ethiopia comprises combination of three drugs in two classes of antiretroviral drugs, i.e. nucleoside (tide) and non-nucleoside reverse transcriptase inhibitors (i.e. 2NRTIs + 1NNRTI) [2]. Few studies conducted in Ethiopia revealed rate of ART failure among adult ART users ranged from 0.4 to 8 per 100 PYO. Predictors of treatment failure were not well explored and not consistent among studies [10-16].
Hence, this study was designed to disclose the incidence and predictors of ART failure for clinicians and health program planners to continually survey and improve quality of ART care.
A five year (January, 2012 to December, 2017) hospital-based quantitative retrospective follow-up study was conducted from June 1, to August 30, 2018 at University of Gondar specialized hospital. The hospital is located in North-West Ethiopia which is 750 km away from the capital, Addis Ababa. The hospital has a catchment population of five million people. The ART Clinic was established in 2003. A total of 5,540 clients started ART since its establishment. Free access to ART in the clinic was launched in 2005.
The source population was HIV patients above the age of 18 years who were on HIV care at University of Gondar hospital from January 1, 2012 to December 31, 2017. All adult HIV patients who took ART > 6 months and had complete data during the study period were considered as study subjects. Patients who were less than 6 months on ART, who had been on second line ART regimen, lost to follow up, transfer in, and pregnant and lactating mothers were excluded from the study (Figure 1).
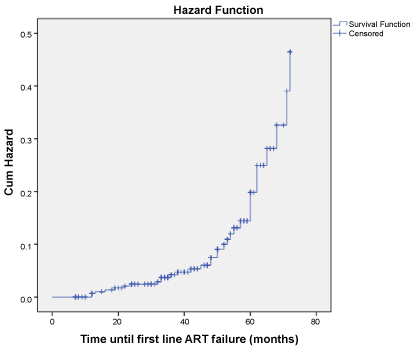 Figure 1: The cumulative hazard of first line ART failure among ART users at University of Gondar Specialized hospital, North West Ethiopia from Jan 1, 2012 to Dec 31, 2017 (n = 315).
View Figure 1
Figure 1: The cumulative hazard of first line ART failure among ART users at University of Gondar Specialized hospital, North West Ethiopia from Jan 1, 2012 to Dec 31, 2017 (n = 315).
View Figure 1
The primary outcome was treatment failure, defined by virological, immunological or clinical failure. Adherence to ART was assessed by pill counts at visits and records adherence as GOOD (≥ 95% adherence), FAIR (80%-95%), or POOR (< 80%). Missing doses in the last 3 days or missing > 15 doses since last visit was defined as poor adherence.
HIV viral load was measured at 6 months and 12 months after initiating ART and every 12 months thereafter. CD4 count was determined every 6 months until patients were stable on ART, and then as indicated.
The sample size was calculated based on a log-rank test with the assumption of the proportional Cox hazard model. In a recent study conducted in Bale hospital, Southern Ethiopia, magnitude of treatment failure was 11.74%. Among the different predictors of treatment failure, inadequate adherence after initiation of ART yields the maximum sample size, with an HR of 1.60. The sample size required was 286 with 10% of contingency for incomplete data resulted in 315 study subjects to be included in the study. An assumption of significance level α = 0.05 (Zα/2 = 1.96) and power 1-ß = 0.8 (Zß = 0.84) were considered. Systematic random sampling technique was used to recruit 315 patients' charts from a total of 1650.
Pretested and structured questionnaires were used to collect the data. The questionnaires were constructed with socio-demographic characteristics (age, gender, marital status, religion, residence, occupation and educational level) and information related to HIV infection and antiretroviral therapy (nutritional status, WHO clinical stage, concomitant opportunistic infections (OIs), tuberculosis (TB) co-infection, functional status, type of ART regimen, presence of ART drug toxicities, and level of adherence) as predictor variables for ART failure.
The medical records to be reviewed (both baseline and follow up records) were identified by their medical registration/card numbers. Then data collectors reviewed and extracted data from patient medical records and registries using a check list. A total of five health professionals, three ART nurses as data collectors and two public health officers as supervisors, were recruited for the data collection process.
Training on the objective of the study and how to review the documents as per the data extraction format was given to data collectors. All questionnaires were checked during the data collection period by the responsible supervisors to check for completeness, clarity and consistency. Data were cleaned to check for errors during entry.
Data were entered into Epidemiological information (EPI INFO), version 7.1 and was analyzed using Statistical Package for Social Sciences (SPSS) version 21.
Descriptive statistics, such as median and inter quartile ranges (IQR) was used to compute continuous variables, and counts with percentage for categorical variables. Both bi-variable and multivariable Cox proportional hazard model was fitted to identify predictors of treatment failure. Those variables with a p. value < 0.2 in the bi-variable analysis were exported to multivariable analysis to control the possible effect of confounders. Hazard ratio with 95% CI and P-value ≤ 0.05 in the multivariable model was used to select variables which have a significant association with the time to ART failure. Kaplan-Meier survival curve was used to estimate the median survival time from initiation of antiretroviral therapy to treatment failure.
Ethical clearance was obtained from the Research Ethical Review Board of School of Medicine, University of Gondar. Formal letter of permission was obtained from University of Gondar hospital administrative body. Confidentiality of information was maintained by coding and restricting access to the questionnaire.
Treatment failure: Is categorized as clinical, immunological and virological failure and defined as follows:
Clinical failure: New or recurrent WHO clinical stage 4 conditions, or new or recurrent WHO stage 3 with pulmonary TB or severe bacterial infections.
Immunological failure: Fall of CD4 count to baseline (or below) or 50% fall from on treatment peak value or persistent CD4 levels below 100 cells/mm3.
Virological failure: Persistently detectable viral load exceeding 1000 copies/mL after at least 6 months of starting a new ART regimen.
Inadequate adherence: Total missed appointments described by greater than three days per month.
ART drug toxicities: Clinical or laboratory adverse events resulting in hospitalization, major disabilities, changing or discontinuation of the culprit ART drug(s).
Lost to follow-up: Study subjects who newly initiated ART and were then lost to follow-up, defined as not having been seen at ART clinic for ≥ 1 month and for whom vital status (alive or dead) was not already known
Base line BMI (recorded at the initiation of ART): ≥ 30 kg/m2 obesity, 25-29.9 kg/m2 over weight, 18.5-24.9 kg/m2 normal, ≤ 18.5 kg/m2 under nourished.
Functional status: Working is capable of going out of home and does routine activities; ambulatory is capable of self-care and going to toilet unsupported; bedridden is cannot go even to the toilet unsupported.
A total of 315 HIV infected individuals on first line ART regimen were included in the study. The median age at the time of enrollment was 35 years (IQR 30-40). One hundred eighty six (59%) were females, 149 (47.3%) were married, 260 (82.5%) were orthodox Christian by religion, and 254 (80.6%) were urban dwellers. Forty percent of study participants were not employed. One-quarter of (24%) had no formal education (Table 1).
Table 1: Socio-demographic characteristics of HIV/AIDS patients on antiretroviral therapy at UOG, North West Ethiopia, from Jan 1, 2012 to Dec 31, 2017 (n = 315). View Table 1
Almost half of them (49.8%) had advanced disease (WHO clinical stage 3 and 4) at time of ART initiation. Majority of them 261 (82.9%) had a BMI > 18.5 kg/m2, and 272 (86.3%) were actively engaged in routine activities (working functional status).
The median CD4+ count at the time of ART initiation was 201 cell/mm3 (IQR 112-309), and majority of them 244 (77.5%) had CD4+ count > 100 cell/mm3 (Table 2).
Table 2: Clinical characteristics of HIV positive patients on first line ART in UOG, North West Ethiopia from Jan 1, 2012 to Dec 31, 2017. View Table 2
TDF/3TC/EFV or AZT/3TC/EFV (EFV-based regimen) was the frequently prescribed ART regimen (68.6%). Majority of patients 244 (79%) had good adherence (> 95%) to their ART regimen. One in five (21.3%) patients experienced drug toxicities while on ART. Among those who experienced ART failure, 26/32 (81%) each had virologic or immunologic failure (Table 2).
The study subjects were followed for median follow up period of 42 months (IQR 32-56). During 13,374 person-months of follow up, 32/315 (10.2%) persons failed their first line ART regimen at incidence of 2.392 failures per 1000 person-months of observation. Ten persons failed the ART regimen at incidence of 1.955 failures per 1000 person-months within 2 years of follow-up. Another 16 persons failed the treatment at incidence of 2.151 failures per 1000 person-months in 2-4 years of follow up. The rest 6 persons failed their ART regimen at incidence of 4.386 failures per 1000 person-months after 4 years of follow-up.
Multivariable Cox proportional hazard model was used to identify predictors of treatment failure. Accordingly, patients with inadequate adherence, WHO clinical stage 3 and 4, low BMI, and experiencing ART drug toxicities were at more hazard risk of ART failure by 6.01 , 4.47, 3.34 and 2.47 times with 95% CI (AHR (2.543,14.661)), (AHR (1.625,12.301)), (AHR (1.552,7.201)) and (AHR (1.013,5.594)), respectively. Patients educated to secondary level was at lower risk of ART failure (AHR = 0.0283 (95% CI: 0.089-0.897)) as compared to those not joining formal education (Table 3).
Table 3: Cox proportional hazard analysis with bivariable and multivariable model for socio demographic and clinical characteristics of HIV patients on ART in UOG, North West Ethiopia from Jan 1, 2012 to Dec 31, 2017 (n = 315). View Table 3
The overall incidence of first line ART failure in this study was 2.39 per 1000 person-months (95% CI: 1.6-3.3) of observations. Higher incidence of ART failure was reported from Ethiopia (4.91 per 1000 person months) and Senegal (4.08 per 1000 person-months) [5,12]. Other studies from Ethiopia (0.78 per 1000 person-months) and Sub-Saharan Africa (1.33 per 1000 person-months) documented lower incidence of ART failure [5,14]. Reasons for varied results could be explained by differences in ART initiation criteria, ART regimen used, definition of ART failure and period of follow-up.
The cumulative hazard of treatment failure was 2, 2.2 and 4.4 failures per 1000 person-months in < 2 years, 2-4 years, and > 4 years of follow up period respectively. Study by Bayu, et al. from Ethiopia stated that treatment failure was 3-fold and 7-fold increase in those who took ART for 2-4 years and > 4 years respectively as compared to those who took ART < 2 years period [11]. The risk of treatment failure continued to steadily increase with longer treatment duration, possibly explained by decline in adherence rate with time, a phenomenon known as 'treatment fatigue' [4,7,11].
Inadequate adherence was found to be predictor of treatment failure (AHR (95% CI: 2.543-14.661) = 6.01)). This finding was consistent with studies conducted in Ethiopia (AHR (95% CI: 1.86-19.80) = 5.68)), Kenya (AHR (95% CI: 2.20-3.49) = 2.77)) South Africa (AHR (95% CI: 2.13-2.91) = 2.49)) and Uganda (AHR (95% CI: 2.3-11.05) = 5.05)) [7-9,12,15]. In fact adherence issue is the pillar for ART users. It is evident that individuals missing three doses of ART per month are associated with loss of sustained HIV suppression, and higher risk of drug resistance and treatment failure.
As in studies in South Africa and Uganda, treatment failure significantly occurred in those with WHO clinical stage 3 and 4 [8,9]. Advanced HIV disease often associated with high viral load and low CD4+ count. Higher viremic level and hindered immunologic recovery were identified as predictors of treatment failure.
Treatment failure significantly occurred in those who experienced ART drug toxicities, similarly reported in other developing world [16-18]. ART drug toxicity is a major contributor to poor drug adherence and hence to treatment failure.
Low baseline BMI was found to be predictor of treatment failure, congruent with Studies in other African countries [4,9,15]. Treatment failure in those with low nutritional status might be related to weakened immunity and blunted immune response.
Those educated to secondary level was found to be more protected from treatment failure as compared to non-educated ones, possibly explained by better understanding of adherence issues and impact of ART on life modification in those educated to secondary level [13]. The above finding was not congruent with other Ethiopian study, which revealed those with formal education had increased chance of treatment failure as compared to non-educated ones. This might be due to differences in level of counselling provided to both study groups, and adverse influence of associated social stigma and discrimination in educated ones [15].
Co-infection with TB or presence of other opportunistic infections were not found to be predictors of ART failure, unlike reports from other studies in Ethiopia and Sub-Saharan Africa [3,4,11,12,15,16].
Since it is a retrospective chart review study, other variables significantly affected the finding might have been missed. We suggest prospective study to determine thoroughly the predictors of ART outcome.
Incidence of ART failure at ART clinic, University of Gondar hospital was considerable. The independent predictors of treatment failure were poor adherence, advanced disease at baseline, low nutritional status and educational status. Close follow up and focused care is important to identify early treatment failure using the available resources.
Based on the findings obtained, the following recommendations were put forward in the study area. Validated measure of adherence shall be practiced as non-adherence was the most important determinant of ART failure. Detection of treatment failure using viral load and CD4+ count should be rigorously practiced.
We are grateful to ART Clinic, University of Gondar hospital, for providing the data during the research period.