Background: The Coronavirus Disease 2019 (COVID-19) pandemic became much more severe in 2021. Healthcare students were a crucial population that needs to participate in disease preventive assistance and were very susceptible to COVID-19 exposure due to the specialized nature of their area of study. Knowledge, attitudes, and practices were important for protecting healthcare volunteer students against infection in COVID-19 sampling.
Methods: A cross-sectional descriptive study was conducted on 195 volunteer students of Can Tho University of Medicine and Pharmacy (CTUMP). Participants were interviewed with a series of questions and performed demonstrations under the observation of data collectors.
Results: Students had a solid understanding of infection control, with the best understanding of the topic coming from content based on maintaining a minimum safe distance, where 98.5% of students answered correctly. In 59% of cases, students displayed a positive attitude about a minimum safe distance. Students performing demonstrations displayed strong practical knowledge, with 100% of students correctly demonstrating how to wear and remove clean gloves and 95% of students washing their hands exactly. There were some factors related to the knowledge of students including gender, course, number of sessions attended, and skills training background while related factors of the attitudes of students were number of sessions attended, and skills training background.
Conclusion: Students participating in COVID-19 community sampling showed good understanding and attitudes toward most research topics. Most students practiced hand washing routine, wearing, and removing clean gloves well. Students' gender, course, number of sessions attended, and history in skills training were associated with their knowledge and attitudes.
COVID-19, Pandemics, Infection control, Infectious disease, Public health
The COVID-19 outbreak initially surfaced in December 2019 among a group of persons who had pneumonia of unknown origin, with Wuhan city in China's Hubei province serving as the first epidemic center [1,2]. The Wuhan City Health Commission announced a pneumonia outbreak with an unidentified etiology to the public on December 31 st , 2019, and also informed the WHO of the situation [1]. The emergence of 2019-nCoV was declared a Public Health Emergency of International Concern (PHEIC) on December 31 st , 2020. COVID-19 has subsequently spread quickly around the world [3-5]. In Singapore as of May 28 th , 2022, there were 23 fatalities and 17,267 recovered cases, or 53% of COVID-19 patients. Meanwhile, there were 10 SARS-CoV-2 infections in Malaysia, according to the country's Ministry of Health, bringing the total number of cases to 7,629. Malaysia also had recorded 115 deaths at that point. The Philippines had the biggest one-day increase since the virus first appeared there in January, with an additional 539 cases being reported there, bringing the infection total to 15,588,921. The total number of people who died as a result of the viral illness in the Philippines increased to 921 after 17 further individuals passed away [6]. Vietnam reported 639 new cases between April 5 th and April 11 th , 2023, representing an average of 90 new cases every day. The frequency of hospital admissions also tended to rise; 10 instances of severe patients, or an average of 1-2 severe cases per day, were reported in a week [7]. Around 10% of all COVID-19 patients are health workers, according to preliminary studies from many nations [6]. Several countries, including China [8,9], Singapore [10], India [11], Brazil [12], and the United Kingdom [13,14], have reported that volunteers make considerable contributions to charitable work. Students studying the health sciences make up the majority of the COVID-19 prevention volunteers. To protect themselves from infection while working, volunteer health science students need to be knowledgeable. Since the community sampling team has the greatest participation rate among all volunteer teams, it is crucial to pay close attention to this team and the issues of knowledge, attitudes, and practices among students about infection control. In Can Tho City, there were 1,020 students in the squad for community testing and 20 backup students, all of whom were mobilized by Decision No. 129/QD-BCD on August 7 th , 2021 [15]. According to the Ministry of Health's instructions, Can Tho City, one of the Vietnamese cities directly under the central government, began implementing social distancing on July 12 th , 2021. Following a time of isolation, the COVID-19 pandemic continued to grow in complexity, and on August 7 th , 2021, the City's Steering Committee for COVID-19 Prevention and Control, which is led by the Chairman of the City People's Committee, began to intervene. Can Tho has approved a plan to form a local COVID-19 team for quick testing and sampling. The largest state institution in the Mekong Delta, Can Tho University of Medicine and Pharmacy (CTUMP), has often had students take part in community testing both inside and outside of the province. At CTUMP, a survey of 2,032 students found that 72.5% of them said they were prepared to respond to the COVID-19 pandemic [16]. To better understand the knowledge, attitudes, and practices of infection control among the student volunteers at CTUMP who were part of the community sampling team, our research team carried out a cross-sectional descriptive study on COVID-19 pandemic co-prevention. The student subjects were chosen from among normal students at CTUMP who were members of the community sampling team, took part in the campaign in Can Tho, and consented to participate in the study. The characteristics of the volunteer students, such as their gender, academic year, number of sample sessions, training status, etc., were also gathered and examined. Recommendations for policymakers were also given along with an explanation of the factors impacting their knowledge, attitudes, and practices of infection control.
Students in Vietnam's healthcare science participated in this cross-sectional survey. At the biggest public medical university in the Mekong Delta, Can Tho University of Medicine and Pharmacy (CTUMP), Vietnam, participants were chosen from nine different academic fields, including medical technology, nursing, pharmacy, odonto-stomatology, medicine, traditional medicine, preventive medicine, and public health. These 9 fields are all fields in the university. To be able to conduct a comprehensive and objective survey, we surveyed all the majors that the school is training. The proportion of participants from each field is fortuitously different. A 2-step procedure was used to recruit eligible volunteers for the study: face-to-face interviews, followed by practice demonstrations that data collectors watched. Data was gathered from December 2021 to February 2022.
The face-to-face interview questionnaire was answered by 195 students who volunteered to participate, and 40 students participated in the practical activities. We surveyed after the volunteers had finished their assignments and gone back to the classroom; therefore, we did not provide support for clothes or other equipment; instead, it was up to our teamwork. In addition, we had restricted sources at the time due to their limited output in our nation. So, only 40 students participated in the practical activities. The Cochran formula was used to determine the sample size, with significance level = 0.05, allowable error d = 0.07, and p = 0.67 as the percentage of students volunteering to ensure knowledge of infection control (based on one of our pilot studies on 21 students participating in community sampling at CTUMP), and with the estimated appropriate sample size therefore being 174 students. As a result, statistical analysis was deemed appropriate for the study.
Student volunteers' typical traits were as follows. Students were from 20 to 24-years-old. Those included male and female students. The courses including 46 th , 45 th , 44 th , 43 rd , and 42 nd were 2 nd , 3 rd , 4 th , 5 th , and 6 th year courses, respectively. Those were all courses being trained at school enrolled at the institution except for lockdown the 47 th course (freshman) due to not being eligible to conduct COVID-19 testing samples in the community. Those majors included medical technology, nursing, pharmacy, odonto-stomatology, medicine, traditional medicine, preventive medicine, and public health. The number of sessions attended included under 14 sessions, from 14 to 28 sessions, and over 28 sessions. The skills training subject consisted of 2 modules and the subject content was basic clinical practice. Competencies, such as infection control competencies, were taught in the second year of all 9 academic fields at CTUMP and were provided to medical students in this course. Those were divided into 3 groups studied, currently studying, and have not studied students.
Students who volunteered were assessed for the following knowledge of infection control: the six steps of standard hand washing, how to wear clean gloves, how to wear personal protective equipment, how to use N95 masks, how to collect specimens, how to take off gloves, how to take off PPE, how to take off PPE on a general level, how to use disinfecting spray on surfaces, and the minimum safe distance. Each process was divided into steps and 1 point was awarded for each correct step.
Assessment of the student volunteers' attitudes toward infection control included the following: six steps of routine hand washing, the use of clean gloves, the use of PPE, the use of N95 masks, the technique for taking samples, the handling of gloves, the PPE removal process, the PPE removal principle, the removal of N95 masks, the use of disinfecting spray on surfaces, and the minimum safe distance. Depending on how each response to questions was worded, a score of 4, 2, or 0 was assigned to the attitude concerning the levels of disagreement (strongly disagree, disagree, agree, and agree with strong disapproval) in the above topics.
Practice demonstrations included proper hand hygiene, clean gloves, PPE, N95 masks, specimen collection methods, glove removal, PPE removal, and N95 page removal when working with student volunteers to practice infection prevention. When executing the necessary protocols, 1 point was awarded for each successful demonstration.
All data were processed using SPSS 20.0 software (IBM, Armonk, NY, USA) according to the medical statistics method. The Kolmogorov-Smirnov test is used to determine if a variable is regularly distributed. Non-normally distributed quantitative research variables are represented as the median, maximum, and lowest values. Frequencies and percentages are employed to represent qualitative characteristics. We employ the tests of the mean rank of two independent groups (Mann-Whitney U-test) and mean rank of multiple groups (Kruskal-Wallis), with statistical significance established when p ≤ 0.05, to compare the mean difference between two or more groups.
Student characteristics are given in Table 1. Of 195 participants, the proportion of female volunteers who participated in the research was 52.8%, higher than male volunteers (47.2%). Several in the 45 th course participated in research with the highest quantity (43.6%) and students in the 42 nd course represented the lowest quantity (0.5%). General medicine represented the largest group of participating students (69.2%). Students who participated in more than 28 sessions were in the majority, while those who participated in less than 14 sessions were in the minority. The percentage of students who had studied skills training made up the majority, while the percentage of students who had not studied skills training made up the minority.
Table 1: General characteristics of the study subjects. View Table 1
Figure 1 describes knowledge of medical students’ infection control in COVID-19. The content about safe distance had the highest number of students with completely correct answers, 192 students (98.5%), while knowledge about the content of taking samples for COVID-19 testing had the lowest number of students with completely correct answers, 48 students (24.6%).
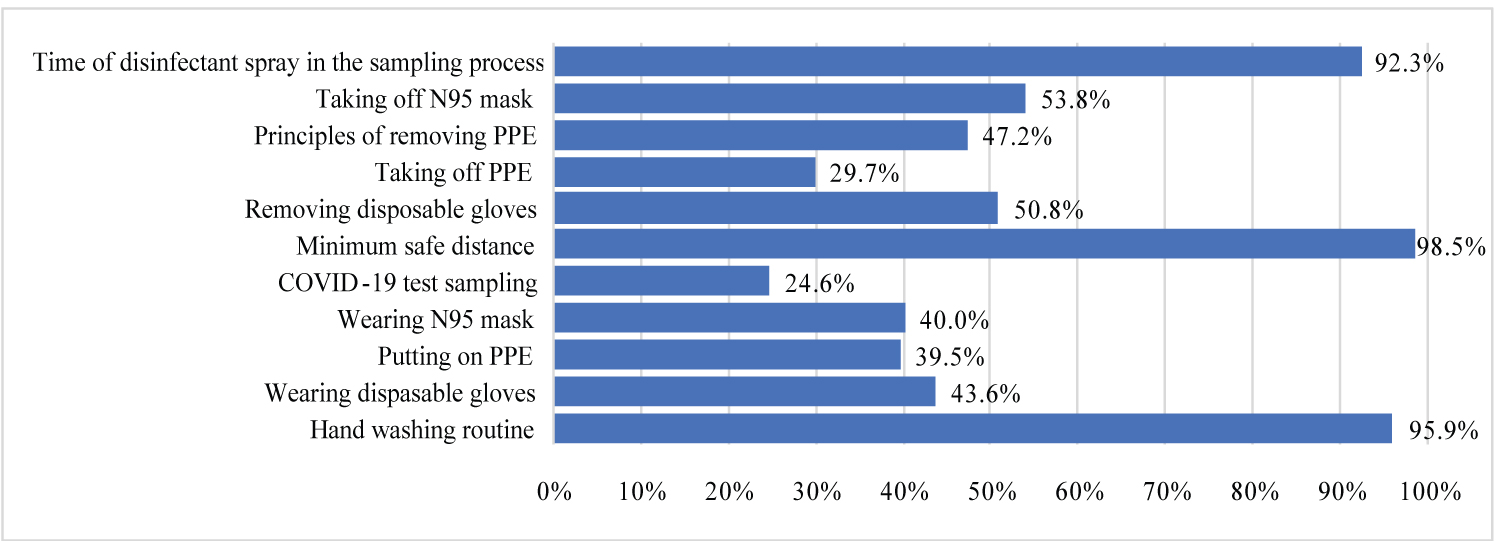 Figure 1: The proportion of correct responses on the COVID-19 infection control knowledge among student volunteers.
View Figure 1
Figure 1: The proportion of correct responses on the COVID-19 infection control knowledge among student volunteers.
View Figure 1
Attitudes towards medical students’ infection control of COVID-19 are illustrated in Figure 2. When it came to the information regarding safe distance, 115 students exhibited the most proper attitude (59%). Out of attitude scores for all exercises, the fewest students scored full points in donning gloves, at only 3 students (1.5%). 65 students who received the maximum score when wearing PPE was the highest (33.3%). The procedure for removing PPE received the highest rating from 62 students or 31.8% of the class. Attitudes about removing N95 masks reached a maximum score for 76 students, accounting for 39%. 45 students or 23.6% of students received the maximum score for attitudes about spraying surfaces with disinfectant.
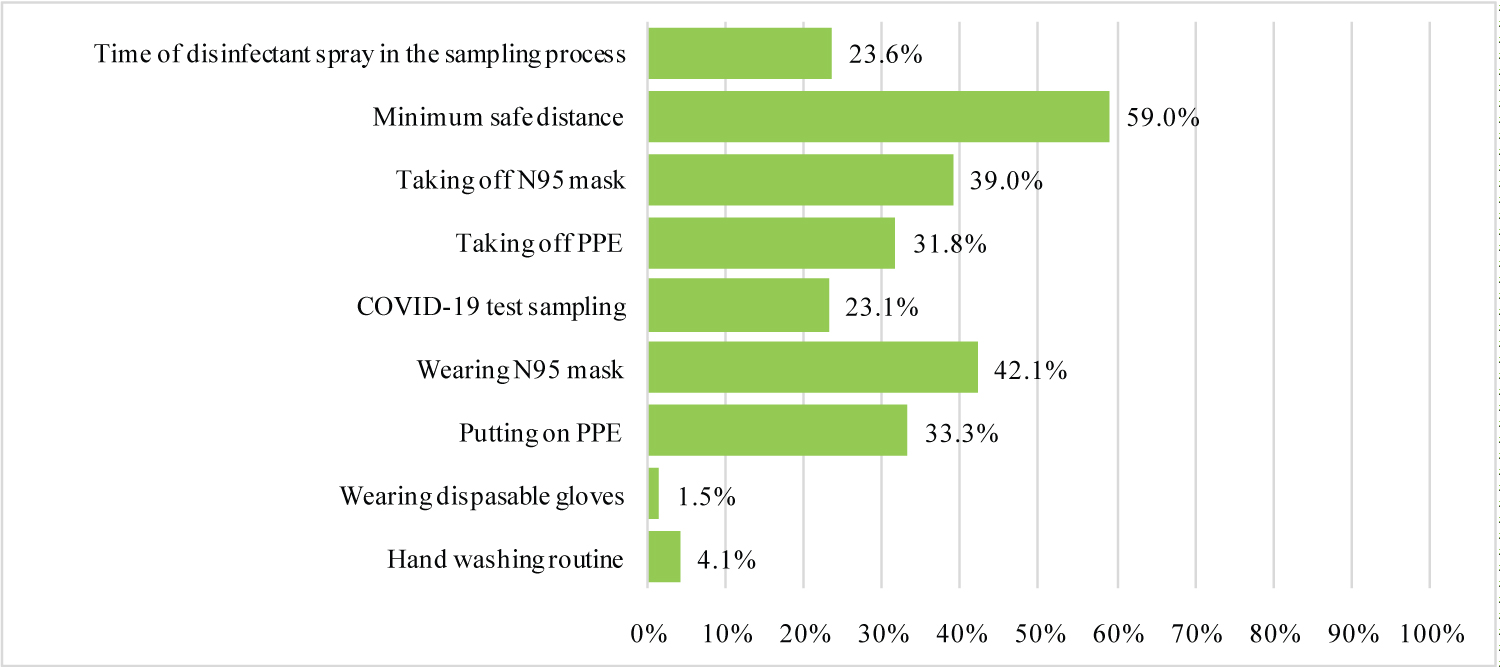 Figure 2: The proportion of correct responses on the COVID-19 infection control attitudes among student volunteers.
View Figure 2
Figure 2: The proportion of correct responses on the COVID-19 infection control attitudes among student volunteers.
View Figure 2
The demonstrations of content about wearing and removing gloves displayed the highest number of completely correct students, 40 students (100%). Regarding the content about taking samples for COVID-19 testing, the lowest number of students were completely correct, with 26 students (65%) earning full points. The number of students who successfully practiced donning and removing N95 masks was 27 (67.5%) and 37 (92.5%), respectively. Students’ practices of infection control are given in Figure 3.
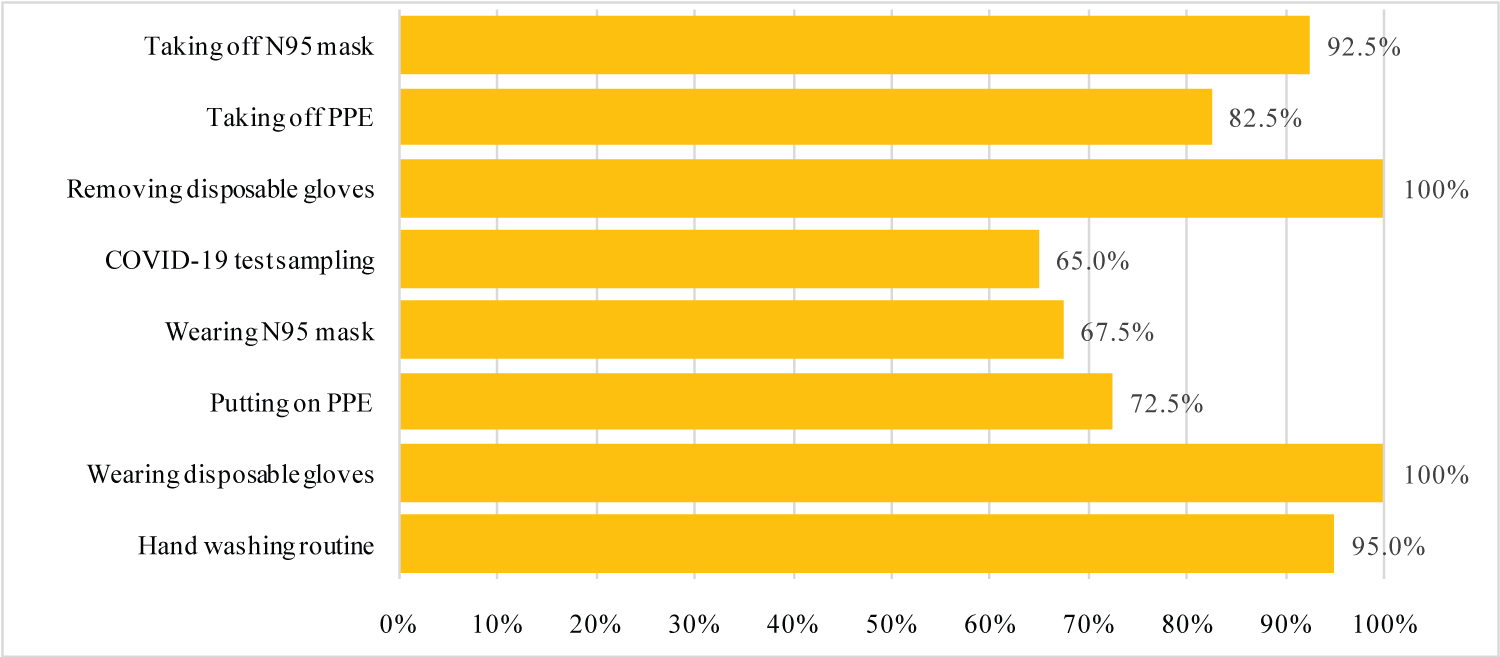 Figure 3: The proportion of correct responses on the COVID-19 infection control practice among student volunteers.
View Figure 3
Figure 3: The proportion of correct responses on the COVID-19 infection control practice among student volunteers.
View Figure 3
Table 2 depicts the variables relating to students' knowledge, and attitudes toward infection control. The average overall rank for knowledge of infection control among women is greater than that of males (107.30 > 87.59, p = 0.015). Students of the 42 nd course had the greatest average rank (164.00), while students of the 45 th course had the lowest average rank (81.93) with p < 0.001. Knowledge in the skills training groups that had been and were studying had a higher average rank than the group that had not studied, with p = 0.031. Regarding opinions about the material covered in skills training, the groups that learned and did not learn had a higher average rank than the group that was learning (p = 0.041). The class that attended less than 14 sessions had the greatest average score in terms of practice. The group that had been studying had a higher average rank than the group that had not yet been taught the skills when they practiced the material contained in skill training.
In this study, male volunteers (accounting for 91) were fewer in number than female volunteers (accounting for 103). According to Pham Thi Ngoc Nga's research on 847 students studying at CTUMP, the university has more female students (487) than male students (360). Students of the 45 th course (3 rd -year students) participated in research in the highest numbers with 86 students, and the 42 nd course (6 th -year students) had the lowest number of participating students with 1 student. The hectic course schedule and the scheduling of clinical internships at hospitals throughout the survey period caused these above sampling results. The research had general medical students as the largest participating group with 135 students and public health students making up the smallest number of participants with 3 students [17].
Students who are currently enrolled in and have completed medical education and simulation practice have a deeper understanding of medicine. Studying medical education and simulation centers has given 5 th -year student and final-year students at CTUMP the necessary medical knowledge and abilities, according to research on 462 of these pupils [18]. So, students did not worry during the study and are willing to take on future tasks related to the medical field in anti-epidemic work, and will also be able to handle the challenging circumstances that appear throughout the anti-epidemic process.
The content of 6 routine hand washing steps had a high number of students answering correctly, namely 187 students, accounting for 95.9%. In addition to this data, a study of 589 general medical students in the 5 th and 6 th years at the University of Medicine and Pharmacy in Ho Chi Minh City had a correct answer rate of 92.4% [19]. Our study's rate and this rate are not the same. An important reason is that we examined 2 nd to 6 th years students (from the 46 th course to the 42 nd course) in all fields who took COVID-19 test samples in the community. The University of Medicine and Pharmacy - Hanoi National University surveyed 653 students, with 99.1% of students answering correctly [20], showing that health students across Vietnam clearly understand how to wash their hands properly before taking samples. Samples are important in the prevention and control of SARS-CoV-2 infection. Regarding the technical knowledge of specimen collection, the research results showed only 48 students answered correctly (24.6%); this figure is lower than a study on 589 students in their 5 th and 6 th years of study for a Medicine major at the University of Medicine and Pharmacy in Ho Chi Minh City, in which 62.3% answered correctly [19]. The content of the minimum safe distance has 192 students with correct answers (98.5%), these results are more positive than a study on nursing students at Hanoi Medical College in which only 54.2% of students answered correctly [21]. In the knowledge of spraying and disinfecting surfaces, 92.3% of students answered correctly; this is also considered very important knowledge in the prevention of COVID-19 and is emphasized clearly in an article from the Ministry of Health, Department of Preventive Medicine [16]. The proportion of students successfully answering questions about donning and removing personal protective equipment was 39.5% and 29.7%, respectively. This is comparable to research on 589 students at the University of Medicine and Pharmacy in Ho Chi Minh City, which had correct answer rates of 34.8% and 26.1%, respectively [19]. These figures may be relatively low because this knowledge is quite new to students participating in the fight against COVID-19 and includes many detailed steps that are prone to errors. Only 78 students (40%) correctly described the procedure of wearing an N95 mask; 105 students (53.8%) correctly described the procedure of removing the N95 mask. The role of the N95 mask in limiting the spread of COVID-19 is shown by Wang, et al.; 10 out of 213 medical professionals who did not wear masks were infected with COVID-19 and none of the 278 people who wore N95 masks became infected [22]. Regarding knowledge of the protocol for wearing clean gloves and removing gloves, respectively, 85 students (43.6%) and 99 students (50.8%) answered correctly. The principles of removing PPE had 92 students (47.2%) giving correct answers.
There were only 3 students who showed a proper attitude regarding the glove replacement method. To reduce the danger of COVID-19 infection when collecting community samples, the Ministry of Health of Vietnam has published a guideline on changing gloves. However, only 1.5% of the participating students displayed the recommended attitude. It is concerning that only 33.3% of pupils (65 students) demonstrated a positive attitude and received the highest grade while donning PPE. In a separate study of 597 nursing students at the Hanoi Medical College, the accurate response rate for the use of personal protective equipment was 98% [21]. The reason for this discrepancy is that whereas the research by author Tran Thi Nguyet only looked at one issue, our analysis considered two questions. So, when the two studies are compared, the form and the assessment questionnaire are different, causing this discrepancy. With 62 students demonstrating an appropriate attitude towards the PPE removal procedure or 31.8% of all students, PPE removal had the largest percentage of students displaying the proper attitude. Regarding the attitude towards removing the N95 mask, 76 students, or 39% of the participants, received the highest score. The removal of N95 masks during anti-epidemic procedures, which are crucial in reducing the spread of COVID-19 when obtaining samples in the community, demonstrates the genuine desires of some students participating in volunteer activities to limit the spread of COVID-19 [21]. As per Cheng, Wong, and Chen, we accept that N95 respirators' ability to stop the spread of SARS-CoV-2 has been shown and that the COVID-19 pandemic is a good time to advocate their usage in clinical settings [23]. There were 23.6% of students who received the highest score for opinions regarding cleaning surfaces after collecting samples (46 students). Thus, it demonstrates that, even though wiping the surface of objects after sampling is crucial since the virus can persist, student participants in our study do not always see it favorably. The virus may take hold on the surface of many items for 2 hours to 9 days [24]. Of the total number of participants, 23.1% were represented by 45 students who obtained the highest possible score on attitude regarding the sampling technique. We found that research participants' interviews were overly drawn out and that they had to retain a lot of information to take part in the study, which contributed to the participants' unfavorable sentiments during the sampling process. With 115 students (59%), scoring at the top of the scale, attitude toward safe distance was the subject where the greatest percentage of students were displaying the right attitude.
The procedure for donning and removing gloves was demonstrated correctly by 40 students, achieving 100% correctness. In the study by author Nguyen Thanh Ha on 196 subjects who were doctors and nurses, only 76.5% of subjects practiced correctly [25]. The percentages of students who successfully practiced donning and taking off N95 masks were 27 (67.5%) and 37 (92.5%), respectively. In another study, the rates of using and discarding masks for physicians and nurses were 82.7% and 90.8%, respectively [25]. In comparison to the rate of practicing wearing or removing PPE correctly in another’s research, which was 87.8%, the proportion of participants who earned the maximum scores while wearing and removing PPE were 72.5% and 82.5%, respectively [25]. The aforementioned variations may be the result of the two research projects’ varied assessment methodologies. Our study evaluated each procedure individually, and the author's study evaluated the entire process. In terms of the sampling process, 26 students (65%) performed it correctly. They mostly erred in the instructions to have subjects wipe their noses before taking samples and to let the cotton pad absorb the nasopharyngeal fluid for less than 5 seconds. 38 students correctly followed the recommended hand washing procedures, accounting for 95% of the total, which is comparable to the results of author Pham Thi Ngoc Nga's study on 847 students at CTUMP, where the rate of correct hand washing procedures was 92.1% [17].
Men scored 87.59 out of 107.30 on the knowledge scale, while women scored 107.30. With p = 0.015, there is a difference between men's and women's awareness of infection control. The average rank for men's attitudes is 91.17, which is similarly lower than the average rank for women's attitudes, which is 104.10. As a result, it can be shown that men in our study have less knowledge and more negative views. Similar to our study, a different study of 222 medical students in Oman found that men had lower knowledge scores than women (16.4 vs. 16.5). The results for the attitude part, however, show the contrary, with males scoring 41.1 compared to women's 39.1, with a p-value of 0.01 [26]. Infection control in both sexes was similar, and the average rank of men and women in the practice section has a small difference, 20.57 for men and 20.41 for women, demonstrating that their skills in auditing practice are both very low. This is also demonstrated in a study of 222 medical students in Oman, where the practice score was 44.1 for men and 44.1 for women [26]. Students of the 42 nd course (the final year students) obtained the highest average rank of 164.00 with p < 0.001 among the courses taking part in the survey in terms of knowledge of disease control. This finding is in line with research done on 653 students at the University of Medicine and Pharmacy at Hanoi National University, which found that the 6 th -year students had the greatest comprehension rate at 89.19% with a p = 0.018 [20]. Students of the 44 th course (4 th -year students) received the highest average rank of 22.75 in the load control's practical component. The fourth-year students achieved the highest practice score of 11.9, matching the findings of research conducted on 741 students at nine medical schools in Uganda [5]. Volunteering during the pandemic was negatively impacted by two variables, according to a Chinese study: student classes and the risks associated with volunteer work. Moreover, the amount of time spent watching COVID-19 news, the impact on their country being predicted, and moral obligation all had a good impact on volunteering [27]. Additionally, sixth-year students received the highest average rank of 148.50 in the attitude section. This indicates that the 6 th -year students have a wealth of knowledge and expertise in infection control, perhaps as a result of their extensive training and experience in hospitals. As a result, they have a general understanding of the value of infection management and are likely to have a more optimistic perspective on the subject. The higher average scores occurred when the knowledge and attitude sections had > 28 sessions, with their values being 108.88 and 108.58, respectively. In terms of practice, the group of students who participated in the campaign for fewer than 14 sessions had the highest average score (28.42), while the group that participated for more than 28 sessions had a lower value (20.67). This disparity is partially explained by the fact that when students take part in several sampling sessions, they inadvertently begin to omit some stages from the actual performance of the exercises.
The drawbacks of our study included the limited sample size and the recall bias due to the lengthy research period.
The majority of research topics were approached with good comprehension and attitudes by the students taking part in the COVID-19 community sample. Most of them did a good job of routinely washing their hands, and putting on and taking off clean gloves. In addition, some factors that were associated with students' knowledge and attitudes were their gender, course, number of sessions attended, and history in skills training.
Conceptualization: K.H.P., T.H.N., Q.T.M.H.; methodology: K.H.P., T.H.N., T.A.N.; validation: Q.T.M.H., T.A.N.; investigation: N.D.T.T., P.T.V., N.M.P., T.M.D.; resource: N.M.P., T.M.D.; writing-original draft: K.H.P., Q.T.M.H., N.D.T.T., P.T.V., K.R.Z.; writing-review and editing: K.H.P., T.H.N., Q.T.M.H., K.R.Z.; supervisor: K.H.P., T.H.N.
No additional data are available.
The study has been approved by the Ethics Council in the Biomedical Research of Can Tho University of Medicine and Pharmacy and under the Helsinki Declaration of 1975, as revised in 2008.
The authors declared no potential conflicts of interest concerning the research, authorship, and publication of this article.
We are thankful to Can Tho University of Medicine and Pharmacy in Vietnam for supporting this study.
The authors received no financial support for the research, authorship, and publication of this article.