Vascular anomalies is associated with increased complexity and complication during live donor nephrectomy. We hereby report a right transperitoneal laparoscopic nephrectomy done in donor with complete left sided IVC (LIVC). Preoperative evaluation by CT Angiography clearly demonstrated venous anomaly. In view of long right renal vein, right laparoscopic donor nephrectomy was performed. Length was sufficient for anastomosis in recipient. Recipient's serum creatinine was 1.2 mg/dl on 5th postoperative day. Postoperative stay for donor was uneventful. LIVC is not a contraindication for transperitoneal Laparoscopic donor nephrectomy.
Laparoscopic donor nephrectomy, Complete left inferior vena cava, Venous anomalies
Left sided Inferior vena cava (LIVC) is a very rare great vessel aberration, which is result of developmental abnormalities of supracardinal veins. Different from other reports of LIVC presentation, in our case LIVC is completely lying on left side even cranial to renal vein joining which was traced up to mid thorax level. As per our knowledge this has never been published before. Prevalence of LIVC is only 0.1-0.4% with slight Male preponderance [1]. In order to increase pool of donors, we often tend to include donors with even with venous anomalies. Now a day's Laparoscopic donor nephrectomy (LDN) has become gold standard for kidney retrieval during live kidney transplantation. Generally left LDN is preferred over right side due longer renal vein length, which favours anastomosis [2]. Current literature regarding anatomical variations and their risks related to laparoscopic donor nephrectomy procedure is insufficient [3]. We hereby report a case of Right transperitoneal Laparoscopic nephrectomy done in a donor with complete Left sided IVC.
Voluntary kidney donor was a 37 years male. His CT renal Angiography reported right renal vein length of 44 mm and left renal vein length of 28 mm with left side three renal arteries (Figure 1). In view of long right renal vein and single renal artery, preoperative workup was done and he was planned for right laparoscopic donor nephrectomy (LDN). Transperitoneal right LDN was performed with 4 port. After colon mobilisation ureteral gonadal complex was identified and dissected to reach hilum. Hilar dissection was performed after duodenal kocherisation. Single renal artery was dissected till its origin from aorta. Superior dissection of kidney to free it from Adrenal gland was performed. Lateral and posterior dissection done to mobilise kidney completely. Right renal vein and right renal artery was clipped with 10 mm Hem-o-Lok clips. Kidney was retrieved using Pfannenstiel incision. There was no intraoperative complication and surgery was performed as any other right LDN. Measured graft renal vein length was 30 mm and was anastomosed to recipient right external iliac vein (End to side). Postoperative period was uneventful and donor was discharged on 3rd postoperative day. Recipient made a good recovery with serum creatinine of 1.2 mg/dl on 5th postoperative day.
 Figure 1: Left sided inferior vena cava. From caudal to cranial (a-d) show left sided inferior vena cava, origin of right renal vein from left inferior vena cava, continuation of left sided inferior vena cava till D10 vertebra further confirming complete left sided inferior vena cava(red arrow- inferior vena cava, grey arrow- aorta).
View Figure 1
Figure 1: Left sided inferior vena cava. From caudal to cranial (a-d) show left sided inferior vena cava, origin of right renal vein from left inferior vena cava, continuation of left sided inferior vena cava till D10 vertebra further confirming complete left sided inferior vena cava(red arrow- inferior vena cava, grey arrow- aorta).
View Figure 1
Left sided Inferior Vena Cava is very rare and usually clinically silent great vessel anomaly. Incidence of IVC anomaly is 0.1 to 3%. Out of which LIVC comprises of 0.1-0.4% only. At around 6th week, IVC formation starts and completed by 10th week of gestation. Three paired venous structures (Posterior, sub cardinal and supracardinal) sequentially appear and regress selectively to complete formation of IVC [4]. The posterior and supracardinal vein are dorsal, and the subcardinal veins is ventral. The left subcardinal vein regresses and the right supracardinal vein persists as the renal segment of IVC. The right supracardinal vein forms the definitive IVC just below junction of renal vein and IVC. If Left supracardial vein doesn't disappear, a duplicate IVC is formed. If the right supracardial vein regresses, a Left IVC results.
Madhavan K, et al. reported IVC embryology in detail and concluded that in cases of LIVC from caudal to cranial, IVC is seen as lying on left and ventral to the aorta, and after receiving the left renal vein, it crosses anterior to the aorta to reach its normal position on the right side. The origin of the right renal vein is normal [5]. But in our case it's unique in presentation and has never been reported before. Here IVC is lying completely on left side even proximal to level of renal vein. It was traced proximally till D 10 vertebra as completely lying on left side only. Previously reported case had left sided IVC till renal hilum level.
Even Simforoosh, et al., in their series of three incidentally detected LIVC intraoperatively, observed that it does not impact the outcome of elective LDN and found it interesting that in spite of a short left renal vein stump (~1.5 cm), its anastomosis was easier compared to right renal vein [6]. The left kidney is preferred in donor nephrectomy due to its long renal vein. In our case due to completely left sided IVC, right renal vein length was around 44 mm (Figure 2), hence was planned for right laparoscopic donor nephrectomy in view of longer right renal vein. Although Vena cava anomalies are very rare, but with good preoperative evaluation and identification of these rare anomaly we can prevent morbidity. At our centre, preoperative 3D CT Angiography is preferred mode of evaluation of donor, which with help of talented radiology team provide fast and accurate evaluation of vascular anatomy and is recommended before any kidney donor workup.
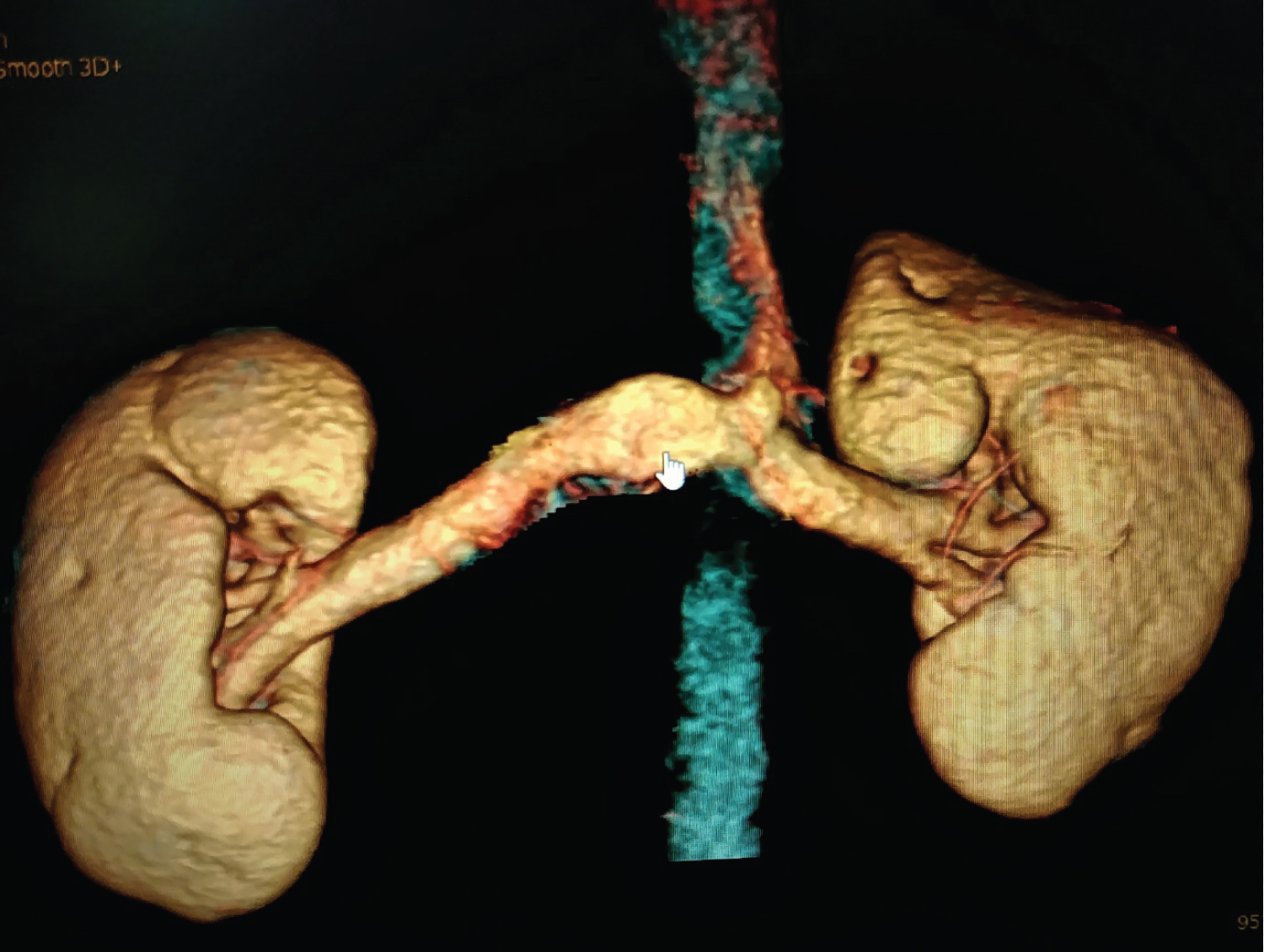 Figure 2: Reconstructed image showing right and left renal vein origin from left inferior vena cava confirming long right renal vein.
View Figure 2
Figure 2: Reconstructed image showing right and left renal vein origin from left inferior vena cava confirming long right renal vein.
View Figure 2
LIVC is not a contraindication for laparoscopic donor nephrectomy. Prior 3D CT Angiography with detailed and elaborative report with nice images can guide us well to go ahead with laparoscopic donor nephrectomy. Choice of side to be taken based on venous anomalies and length of renal vein. Every surgeon performing laparoscopic donor nephrectomy should be well aware of these venous anomalies and prepared for the same.