Carcinosarcoma of the parotid is a biphasic neoplasm composed of malignant epithelial and mesenchymal components. It is a rare malignancy with < 100 cases reported in literature.
Case 1: A 58-year-old male, underwent total parotidectomy for longstanding preauricular swelling. Histomorphology revealed a biphasic neoplasm composed of carcinoma with plasmacytoid morphology and osteosarcoma in the background of pleomorphic adenoma. Carcinoma component was confirmed to be myoepithelial carcinoma by immunohistochemistry. The patient presented with local recurrence two months later.
Case 2: A 32-year-old female with swelling in the left cheek for 6 months and suspected to be malignant on biopsy underwent radical parotidectomy. It showed a biphasic neoplasm consisting of duct carcinoma with comedo necrosis and undifferentiated pleomorphic sarcoma in the background of pleomorphic adenoma which was confirmed by immunohistochemistry.
Carcinosarcoma can arise both de novo and from long standing pleomorphic adenoma. Most patients are aged between 50 - 70 years. Case 2 presented in 3rd decade. The carcinoma component in case 1 was myoepithelial carcinoma which is unusual as compared to duct carcinoma. Sarcoma components may be chondrosarcoma, rhabdomyosarcoma, osteosarcoma or undifferentiated pleomorphic sarcoma.
Malignancy in pleomorphic adenoma should be diligently screened for true sarcoma component due to worse prognosis than carcinoma ex pleomorphic adenoma and also exclude sarcomatoid carcinoma.
Pleomorphic adenoma, Carcinosarcoma, Carcinoma ex pleomorphic adenoma
Malignancy in pleomorphic adenoma, which is the most common salivary gland neoplasm can be subclassified into three types namely Carcinoma Ex Pleomorphic Adenoma (CXPA), Carcinosarcoma Ex Pleomorphic Adenoma (CSXPA) and Metastasizing Pleomorphic Adenoma (MPA) [1]. Among these, carcinosarcoma ex pleomorphic adenoma is less common compared to carcinoma ex pleomorphic adenoma [2]. Carcinosarcoma ex pleomorphic adenoma is also known as true malignant mixed tumor as it contains both malignant epithelial and mesenchymal components in the background of pleomorphic adenoma (mixed tumor) which is known as mixed tumor traditionally [3]. Here, we report two such cases of carcinosarcoma arising in the background of pleomorphic adenoma. A brief review of literature in the past two decades is also discussed.
A 58-year-old man presented with complaints of swelling over the left pre auricular region for the past 5 years. There was no significant comorbid illness or family history. Hemogram, biochemical parameters and serology were within normal limits. Ultrasound of the neck revealed a well-defined solid lobulated heterogeneous lesion of size 7.8cm x 4.8cm in the left parotid region and angle of mandible, not separate from the parotid. Few enlarged lymph nodes were also noted adjacent to the lesion. There was no evidence of vascular or skeletal invasion. Contrast Enhanced CT (CECT) scan of the neck showed a large heterogeneously enhancing solid density lesion involving left parotid gland and involving its deep lobe and reported as likely to be pleomorphic adenoma/ carcinoma.
Fine Needle Aspiration Cytology (FNAC) revealed plasmacytoid cells exhibiting moderate to marked anisokaryosis with few spindle cells. Many binucleated and multinucleated osteoclast like giant cells were seen. A diagnosis of myoepithelial carcinoma was considered.
The patient then underwent total parotidectomy with lateral tarsorrhaphy. Histopathological sections revealed a malignant biphasic neoplasm composed of sheets of plasmacytoid cells exhibiting moderate nuclear pleomorphism, vesicular chromatin and prominent nucleoli (Figure 1A) adjacent to areas of bland tumor cells arranged in ducts and tubules melting into a chondromyxoid stroma (Figure 1B). Foci of osteoid rimmed by tumor cells and multinucleated osteoclast type giant cells were seen (Figure 1C). Lymphovasuclar and perineural invasion were noted. All margins were free of tumors. One intra-parotid lymph node identified showed reactive changes. On immunohistochemistry, the plasmacytoid neoplastic cells were immunoreactive for Smooth Muscle Actin (SMA), p63 (Figure 1D) and CK5/6 with a proliferative index of 30% and they were negative for Pan cytokeratin (PanCK). The adjacent bland ductal cells of pleomorphic adenoma were positive for PanCK. The sarcomatous component was immunoreactive for SATB2 (Figure 1E). Immuno morphological features support the diagnosis of CSXPA composed of myoepithelial carcinoma and osteosarcoma.
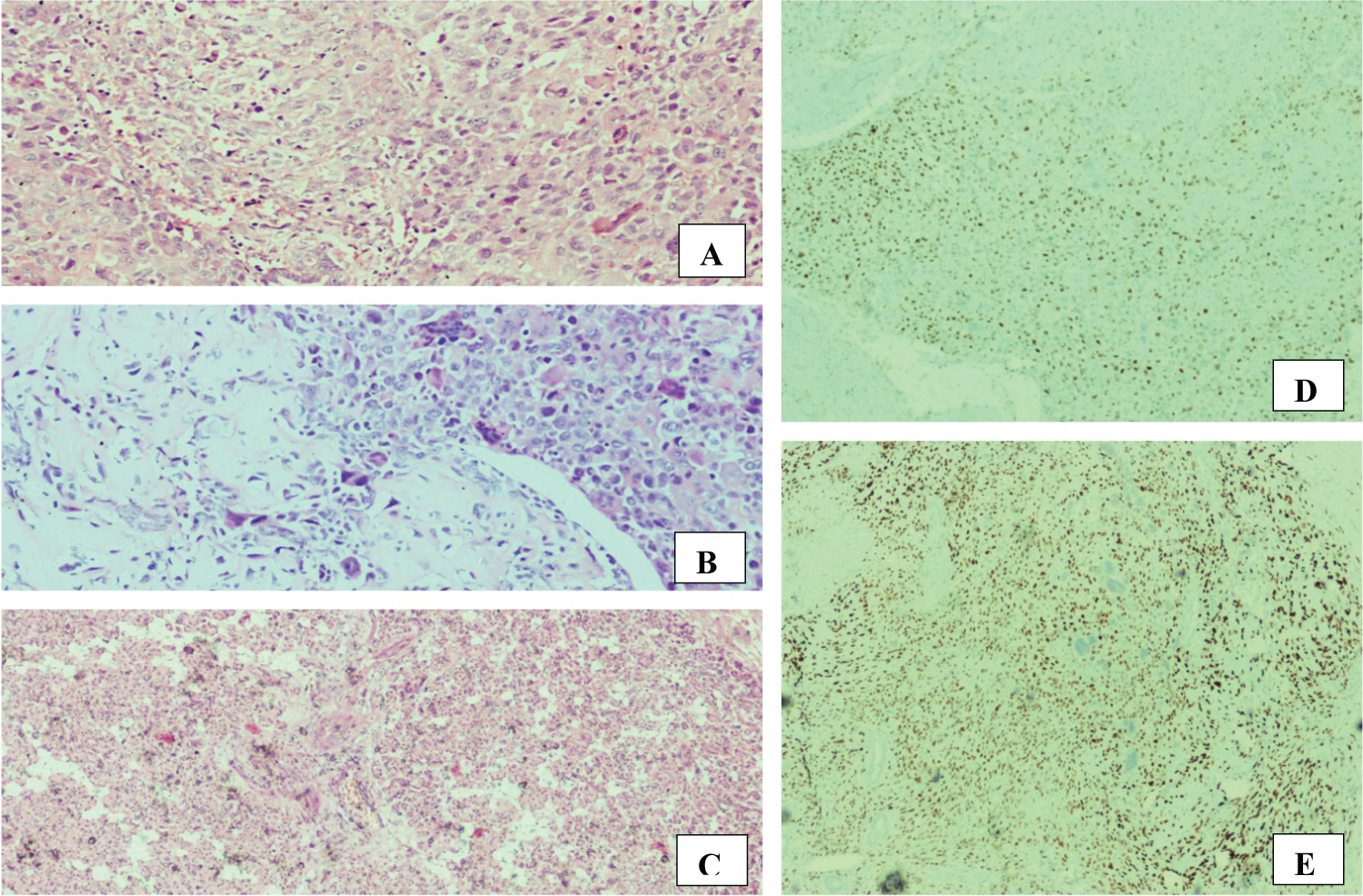 Figure 1: (CASE 1) (A) Myoepithelial carcinoma component, Haematoxylin and Eosin stain x100; (B) Neoplastic cells seen amidst osteoid along with numerous multinucleated osteoclast type giant cells - osteosarcoma component, Haematoxylin and Eosin stain x100; (C) Foci adjacent to the tumour revealed classic areas of pleomorphic adenoma composed of small benign ducts and tubules, Haematoxylin and Eosin stain, x40; (D) p63 Immunohistochemistry highlighting the neoplastic myoepithelial component, x40; (E) SATB2 immuno histochemistry highlights the neoplastic osteoid, x40
View Figure 1
Figure 1: (CASE 1) (A) Myoepithelial carcinoma component, Haematoxylin and Eosin stain x100; (B) Neoplastic cells seen amidst osteoid along with numerous multinucleated osteoclast type giant cells - osteosarcoma component, Haematoxylin and Eosin stain x100; (C) Foci adjacent to the tumour revealed classic areas of pleomorphic adenoma composed of small benign ducts and tubules, Haematoxylin and Eosin stain, x40; (D) p63 Immunohistochemistry highlighting the neoplastic myoepithelial component, x40; (E) SATB2 immuno histochemistry highlights the neoplastic osteoid, x40
View Figure 1
Interestingly, the patient returned with complaints of swelling and pain at the operative site 2 months later. MRI revealed an irregular altered signal intensity lesion - suggestive of residual/ recurrent disease for which he received radiation of 60Gy in 30 fractions.
A 32-year-old female presented with complaints of swelling in the preauricular region for the past 6 months. It was insidious in onset and slowly progressive. The patient did not have any other comorbid illnesses. Clinically, there was a huge swelling seen in the left cheek with ulceration. The patient was anemic with neutrophilic leukocytosis. Biochemical and serological investigations were within normal range. Radiograph of soft tissue neck revealed a large soft tissue opacity in the supraglottic region. CECT scan of neck showed a large heterogeneously enhancing mass lesion in the parotid gland measuring 5.9 x 5.5 cm originating from the superficial lobe of parotid gland without obvious extension to deep lobe, suggestive of malignancy. Prominent level II, III and IV lymph nodes that were likely to be metastasis were also noted.
FNA smears showed a poorly differentiated malignant tumor composed of markedly pleomorphic tumor cells - suspicious of sarcoma. In view of a biphasic malignant neoplasm, a differential of carcinosarcoma was given on biopsy. Subsequently, the patient underwent left radical parotidectomy with modified radical neck dissection. Macroscopically, a friable growth with fleshy and hemorrhagic areas was seen ulcerating the skin. Histopathological evaluation revealed classic areas of pleomorphic adenoma composed of small tubules set in a hyalinized stroma along with a biphasic malignant neoplasm. The carcinoma components were arranged in large ducts with central necrosis (Figure 2A) and the poorly differentiated component was composed of extensive foci of markedly pleomorphic spindle cells (Figure 2B). Neck dissection showed a single metastatic node. Immunohistochemically, the benign ductal components of pleomorphic adenoma and carcinoma components were highlighted by PanCK (Figure 2C and Figure 2D) respectively and the sarcomatous areas were immunoreactive for vimentin (Figure 2E) and negative for PanCK, Epithelial Membrane Antigen (EMA), SMA, S100, CD34, desmin and SATB2. Both components exhibited high proliferative activity. Based on immune morphology, a diagnosis of CSXPA composed of salivary duct carcinoma and undifferentiated pleomorphic sarcoma was rendered.
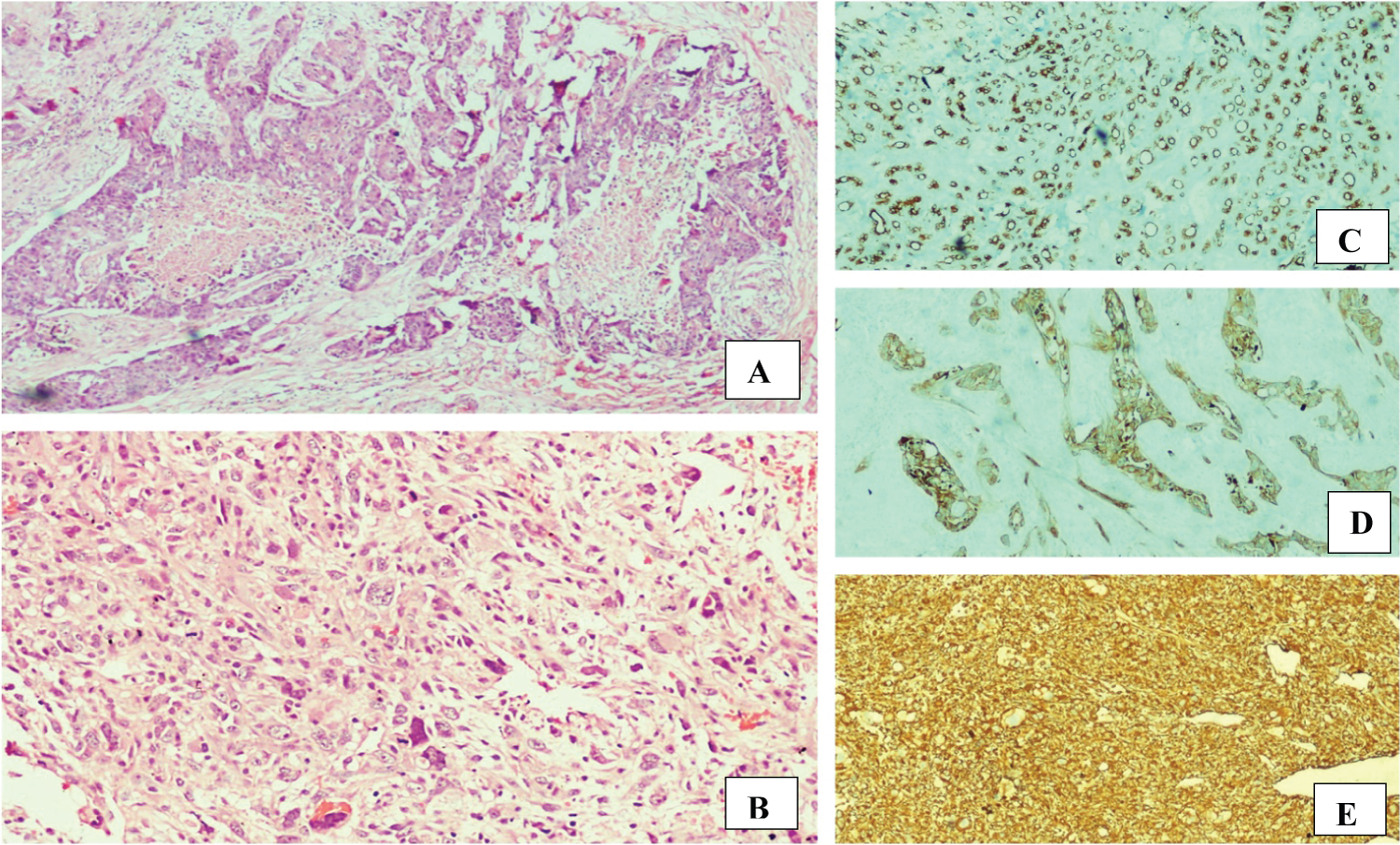 Figure 2: (CASE 2) (A) Salivary duct carcinoma with central comedo type necrosis, Haematoxylin and eosin stain, x40; (B) Sheets of markedly pleomorphic tumor cells - undifferentiated pleomorphic sarcoma, Haematoxylin and eosin stain, x100; (C) Pan CK immunohistochemistry highlighting the tubules and ducts in pleomorphic adenoma area, x40; (D) Pan CK immunohistochemistry highlights the malignant epithelial elements, x40; (E) The undifferentiated sarcomatous areas are immunoreactive for vimentin, x40.
View Figure 2
Figure 2: (CASE 2) (A) Salivary duct carcinoma with central comedo type necrosis, Haematoxylin and eosin stain, x40; (B) Sheets of markedly pleomorphic tumor cells - undifferentiated pleomorphic sarcoma, Haematoxylin and eosin stain, x100; (C) Pan CK immunohistochemistry highlighting the tubules and ducts in pleomorphic adenoma area, x40; (D) Pan CK immunohistochemistry highlights the malignant epithelial elements, x40; (E) The undifferentiated sarcomatous areas are immunoreactive for vimentin, x40.
View Figure 2
Carcinosarcoma is an unusual tumor of salivary gland and accounts for 0.05% of all salivary gland tumors and 0.16% of all malignant salivary gland neoplasms [4]. Carcinosarcoma most commonly presents in the parotid gland (65%), followed by sub mandibular gland (22%) and sublingual gland (13%) [5]. True malignant mixed tumors are also reported in the minor salivary gland [3].
Carcinosarcomas can arise in the background of long standing or recurrent pleomorphic adenoma in approximately 30% of cases [6-8] or without histological evidence of pleomorphic adenoma, so called carcinosarcoma denovo [9]. In this report, first case had along-standing history with histological evidence of pleomorphic adenoma, whereas the second patient had a short duration of symptoms with tell-tale evidence of benign pleomorphic adenoma histologically. Most of the CSXPA of salivary glands present between fifth to seventh decades of life, but however, can range from 14-87 years [10]. There was no significant gender differences [10]. In our report, the second patient presented in the fourth decade.
Microscopically, true malignant mixed tumor of salivary glands can be composed of a wide variety of carcinomas and sarcomasas reported in literature. The malignant epithelial component is most often a poorly differentiated adenocarcinoma or undifferentiated carcinoma or squamous cell carcinoma [5,7]. Salivary duct carcinoma occurring as the carcinoma component in CXPA has been reported in a few articles in literature [11,12] but much rarer is its presence in CSXPA. A mucin rich salivary duct carcinoma ex pleomorphic adenoma has also been reported [13]. Rarer types of carcinomas arising from pre-existing pleomorphic adenoma include Adenoid cystic carcinoma, clear cell carcinoma, sarcomatoid carcinoma and large cell neuroendocrine carcinoma [14-17]. Occasionally, myoepithelial carcinoma occurring in CXPA has been reported [18] with its occurrence in CSXPA, a much more unusual event which is the histology in our first case.
The malignant mesenchymal component can be homologous or heterologous. The most common type of sarcomatous component is chondrosarcoma [5,19,20]. The other sarcomas which can occur in CSXPA are fibrosarcoma, leiomyosarcoma, and liposarcoma [21]. Only a few cases of CSXPA with osteosarcoma elements have been described to date with a brief review of such cases given by Chang Gok Woo, et al. [10]. Single case reports of rhabdomyosarcoma and myxofibrosarcoma present in CSXPA have been reported [7,17]. Undifferentiated pleomorphic sarcoma (previously known as malignant fibrous histiocytoma) is an unusual sarcoma in CSXPA with less than a dozen cases reported in literature to the best of our knowledge [22,23].
Few case reports have demonstrated cytology and histological correlation [22] as in our report, in which the FNA diagnosis of myoepithelial carcinoma was partly consistent with histological diagnosis. The osteosarcoma component was represented in the smear in the form of multinucleated osteoclast giant cells. FNA diagnosis of sarcoma in the second case also corresponded partly with that of histological diagnosis as malignant epithelial elements were not represented in the smear.
Electron microscopy and molecular analysis of carcinosarcoma of salivary glands were performed in a few studies on single case reports [21,24]. Cytoplasmic myoepithelial structures were detected on electron microscopy even in the absence of SMA on immunohistochemistry. Loss of heterozygosity analysis revealed complete deletion of 17p, 17 q and 18q suggesting allelic loss in both epithelial and mesenchymal components [24]. There have been speculations about PLAG1 and HMGA2 abnormalities (which are common in pleomorphic adenoma) in CSXPA but future studies using immunohistochemistry or molecular testing are needed for clear evidence [5]. Oligonucleotide array comparative genomic hybridization has revealed similar genomic profiles in both malignant epithelial and mesenchymal components [25].
One of the oldest case series of CSXPA was presented by James Stephen, et al. in 1986 comprising 12 cases, the majority of which were ductal carcinoma combined with osteosarcoma. In recent years, a population-level based demographic study on salivary gland carcinosarcoma was conducted by Avigeet Gupta, et al. in 2019, however, the independent histomorphological features were not registered [26]. A brief review of CSXPA cases in the past two decades is presented Table 1.
Table 1: A brief review of carcinosarcoma ex pleomorphic adenoma cases in the past two decades. View Table 1
CSXPA is a fatal, extremely aggressive malignancy with a high potential for local recurrence and distant metastasis [2]. Median survival reported at 10 months after diagnosis is 63% [9]. Most CSXPA metastasize to lungs with an occasional case study reporting abdominal metastasis [10]. Treatment modalities include surgery followed by chemoradiation. Both of our cases were primarily treated with surgery followed by radiation of 60Gy for the first case and 50Gy for the second case in 30 fractions. The first case succumbed to illness at 6 months post recurrence and the second patient expired within 4 months of surgery.
In conclusion, CSXPA should be distinguished from carcinoma ex pleomorphic adenoma due to its dismal prognosis and frequent recurrences. We here, report two cases, one with an unusual malignant epithelial component of myoepithelial carcinoma which is hardly reported in Indian literature and both cases with an unusual malignant mesenchymal component, one with osteosarcoma and the other with undifferentiated pleomorphic sarcoma, again both of which account for less than 10 cases reported in Indian literature.
Not applicable.
Dr. C Aparna Devi - collection of case details and writing of manuscript.
Dr Usha Amirtham and Dr Geeta V Patil Okaly - Work up and diagnosis of cases.
Dr Raghavendra H V - Changes and correction in manuscript.