Objective: To trace the clinical and epidemiological profile of penile cancer in Rio Grande do Norte/Brazil and relate them to data published in the literature.
Methods: A retrospective cohort study was conducted with 94 patients diagnosed with penile cancer in 2011-2018, treated at the Liga Norte Riograndense Contra o Cancer.
Results: All patients were diagnosed with squamous cell carcinoma, mainly aged over 50 years, from the state's interior, brown, illiterate, or with incomplete primary education. At diagnosis, 68% of patients were classified as having tumors ≥ T2, and 30% had lymph node involvement. Distant metastases were detected in 2.1% of patients at diagnosis. Most patients received the diagnosis in the initial phase of the disease, but 20.2% were diagnosed in stage IV. Partial penectomy was the most performed surgery, and 10% of patients relapsed, mainly in the lymph nodes (87.5%). The mean follow-up of the patients was 18 months, with an estimated overall survival at five years of 59.1%. However, 25% of patients were followed up for up to 3 months, losing follow-up.
Conclusion: The State of Rio Grande do Norte has a high incidence of penile cancer with a high frequency of locally advanced tumors at diagnosis and in younger patients younger than 50. Furthermore, socioeconomic factors interfere with early diagnosis and hinder access to specialized services.
Penile cancer, Squamous cell carcinoma, Epidemiology, Penile diseases
Penile cancer is a rare neoplasm in the United States and Europe, accounting for less than 1% of cancers in men. However, it is more frequent in less developed areas, such as Africa, Asia, and South America, corresponding to 10-20% of all male malignancies [1,2].
There is, then, the contrast between the prevalence in developed and underdeveloped countries, clearly indicating the association of the pathology with local economic conditions [3,4]. Brazil is one of the countries with the highest incidence of penile cancer in the world [5,6] which may correspond to 2.1% of all neoplasms in men, being five times more prevalent in the North and Northeast regions [7], where most of the procedures are performed. penile amputations [6].
Among these regions, Brazilian studies indicate that the State of Maranhão (Northeast of Brazil) has the highest incidence of penile cancer in Brazil, with an age-standardized incidence of 6.15 cases/100,000 habitants, with approximate statistics of one new case every 17 days [6].
Penile cancer is an aggressive and mutilating disease that affects self-esteem, with psychological and functional repercussions, which make rehabilitation and social reintegration difficult [7]. Despite being a complex surgery, studies show that penile reconstruction (phalloplasty) is possible after penectomy when the functional length of the Penis is inadequate for a man to urinate standing up or have sexual intercourse [8-10].
The disease is more common in older men, with a mean age at diagnosis of 60 years, but it can occur in patients younger than 40 years [7,11]. Its risk factors are multiple, but its carcinogenesis is not entirely elucidated.
Phimosis, poor personal hygiene habits, smoking, history of sexually transmitted diseases are the factors most commonly described in the literature, in addition to low educational level and limited access to health services [3,4].
Furthermore, studies describe that the human papillomavirus (HPV), mainly subtypes 16 and 18, is present in 30-100% of cases of penile cancer and that the vaccine against the virus has potential efficacy of > 70% to minimize the occurrence of genital warts and anal intraepithelial neoplasia [3,4,7,12].
Therefore, the Brazilian Penile Cancer Consensus argues that reducing the incidence of this cancer is possible by encouraging intimate hygiene education, neonatal circumcision, smoking cessation, vaccination against HPV among young people, and the use of condoms [4].
Late diagnoses are based on the male chauvinist culture that self-care with men's health configures a role of passivity, dependence, and male fragility, primarily when related to the genital organ. This thought is predominant in northeastern Brazil [3,13].
Unlike women, social stigma generally makes men seek fewer health services or seek them out in situations of already manifest disease, accidents, or injuries, which generates underreporting of cases. Furthermore, there is the fear of being diagnosed with cancer, commonly associated with death, painful treatments, and mutilations [3,13].
Nursing has crucial participation in the direct care of individuals and the health education of a community, mainly through the Family Health Strategy established by the Unified Health System (SUS), through which it can actively act in the promotion, prevention, and the self-care of Men's Health, or even bring it closer to the strategy with family support to instruct how to prevent penile cancer, diagnose it early and have better prognoses [14].
Penile neoplasia usually presents as a verrucous, flat, or ulcerated skin lesion in the genital region. Its diagnosis is made through broad and deep biopsy of the lesion to assess histology and degree of cell differentiation [4,15,16].
The predominant histologic types of penile cancer are penile squamous cell carcinoma (SCC), melanoma, lymphoma, sarcoma, and basal cell carcinoma. For the staging (study of the extension of the disease) of cancer, the TNM system of the American Joint Committee on Cancer (AJCC) is considered, in which the T indicates the size of the primary tumor and if it has spread to other areas; o N, if there is the dissemination of the disease to regional lymph nodes; and M if there is metastasis in other parts of the body; higher numbers between I and IV mean that the condition is more advanced [4,15,16].
Independent prognostic factors for penile cancer are the stage of the neoplasm (favorable < T1), the volume of the lesion (favorable < 2 cm), the degree of cell differentiation, and the presence of vascular/lymphatic invasion in the primary lesion (metastases are more frequent when there is microvascular invasion) [4,15,16].
Prospective epidemiological studies on penile cancer are scarce and small. And, despite the high incidence, Brazil has few studies on the subject. Then, the guiding problem of the study arose: What is the epidemiological and clinical profile of penile carcinoma in the Potiguar territory?
In this regard, when considering the taboo related to diseases involving the male genital organ, it is essential that each state traces the epidemiological profile of penile cancer so that the topic is more discussed in society, men realize the importance of early diagnosis and, thus, data close to the real are obtained regarding the prevalence of the disease in the state and country and the male population is benefited.
The main objective of the present study was to outline the clinical and epidemiological profile of penile cancer in the Potiguar territory and relate them to data published in the literature.
A retrospective cohort study was carried out following the verifications of the STROBE Guidelines [17]. The study sample consisted of 94 patients diagnosed with penile cancer from January 2011 to December 2018 and treated at the Liga Norteriograndense Contra o cancer. It is a highly complex oncological center in Rio Grande do Norte and the main reference center for the treatment of penile cancer in the state, whose population is 3,168,027 inhabitants, according to data from the last census, carried out in 2010 by the Brazilian Institute of Geography and Statistics (IBGE). Data were obtained from the collection of data from physical and electronic medical records of all patients with an anatomopathological diagnosis of penile cancer. The variables studied were age, color, education level, origin, histological type, tumor grade, TMN AJCC 8 th Edition system staging, type of surgery, lymphadenectomy, chemotherapy, radiotherapy, and palliative treatment. Data were stored in the Microsoft Excel spreadsheet editor. The software SPSS 24 for Windows (Statistical Package for Social Sciences; IBM, USA) was the computational resource used, in which exploratory data analysis, association tests between variables, and overall survival analysis were performed. Fisher's Exact Test was used to verify associations between variables. Survival analyses were performed using the Kaplan-Meier method and the Log-Rank test to verify the existence of significant differences in the estimated curves. The significance threshold was p ≤ 0.05 with a 95% confidence interval. The age-standardized incidence was calculated using the standard world population proposed by Segi and modified by Doll, et al. [18]. The Cancer Incidence in the Five Continents method of the International Agency for Research on Cancer (IARC) was also applied, in which the number of cases in each five-year age group was divided by the size of the population in each age group. As other smaller cancer centers receive patients with penile cancer in Rio Grande do Norte, the estimated incidence from the data presented here provides an approximate estimate of reality. The study was carried out by the principles of the Declaration of Helsinki and approved by the Research Ethics Committee of the Liga Norte Riograndense Contra o Cancer (process number 02089218.6.0000.5293), and informed consent was waived.
From 2011 to 2018, 94 patients were diagnosed with penile cancer, resulting in an average of 11.7 new cases yearly. The age-standardized incidence recorded in this study was 6.38 cases/100,000 inhabitants (Table 1), exceeding previously published rates.
Table 1: Age-standardized incidence of patients diagnosed in Liga Norte Riograndense Contra o Cancer. View Table 1
According to the analysis, 72.2% of the patients came from the state's interior, while 27.8% came from the capital (Table 2). The majority, 67.8%, were brown (Table 2).
Table 2: Distribution of cases, according to origin, age group, skin color, education, TNM classification, clinical staging, surgical treatment, chemotherapy and radiotherapy treatment and relapse (%), of patients diagnosed in the Liga Norte Riograndense Contra o Câncer. View Table 2
Similar to data from the world literature, most patients (84.1%) were illiterate or had incomplete primary education, and 81.4% were diagnosed with penile cancer aged 50 years or older (Table 2). The mean age at diagnosis was 63 years.
All patients were diagnosed with squamous cell carcinoma, 80.9% of which had histological grade 2. Angiolymphatic invasion and perineural invasion, factors known to have a worse prognosis [19], were present in 87.7% and 83% of cases, respectively.
Risk factors related to penile cancer, such as phimosis, smoking, alcoholism, history of sexually transmitted diseases, human papillomavirus (HPV) infection, and presence of pre-neoplastic diseases, could not be evaluated the study due to a deficit in filling out medical records.
By the AJCC 8th edition TNM classification system, 68% of the patients were classified as ≥ T2 (Table 2). Lymph node involvement at diagnosis was present in 30% of patients and distributed as follows: N1 in 7.4%, N2 in 4.3%, and N3 in 18.1% (Table 2), and distant metastases were detected in 2.1% of patients at diagnosis, with bones and lungs being the main sites affected.
Most patients were diagnosed in the early stages of the disease, in clinical stages I (21.3%), IIA (27.7%), and IIB (19.1%). 20.2% of the disease was diagnosed in stage IV (Table 2).
Regarding surgical procedures, approximately half of the patients (48.9%) underwent partial penectomy exclusively, 20.2% partial penectomy with radical inguinal lymphadenectomy, and 9.6% total penectomy. Among the patients who underwent lymphadenectomy, 76.4% underwent bilateral lymphadenectomy, and 23.6% underwent unilateral lymphadenectomy (Table 2).
About 5.4% received adjuvant chemotherapy alone, and 3.3% received adjuvant radiotherapy alone. At the same time, 2.1% underwent adjuvant chemo and radiotherapy. Furthermore, 10% of patients relapsed, mainly in lymph nodes (87.5%), lungs, and bones (12.5%).
Mortality significantly worsened with staging. While 12.5% of patients in stage I died, 33.3% of patients in stage IV died in the same period (Table 3). The mean follow-up of the patients was 18 months, with an estimated overall survival at five years of 59.1% (Figure 1). However, 25% of patients were followed for up to 3 months.
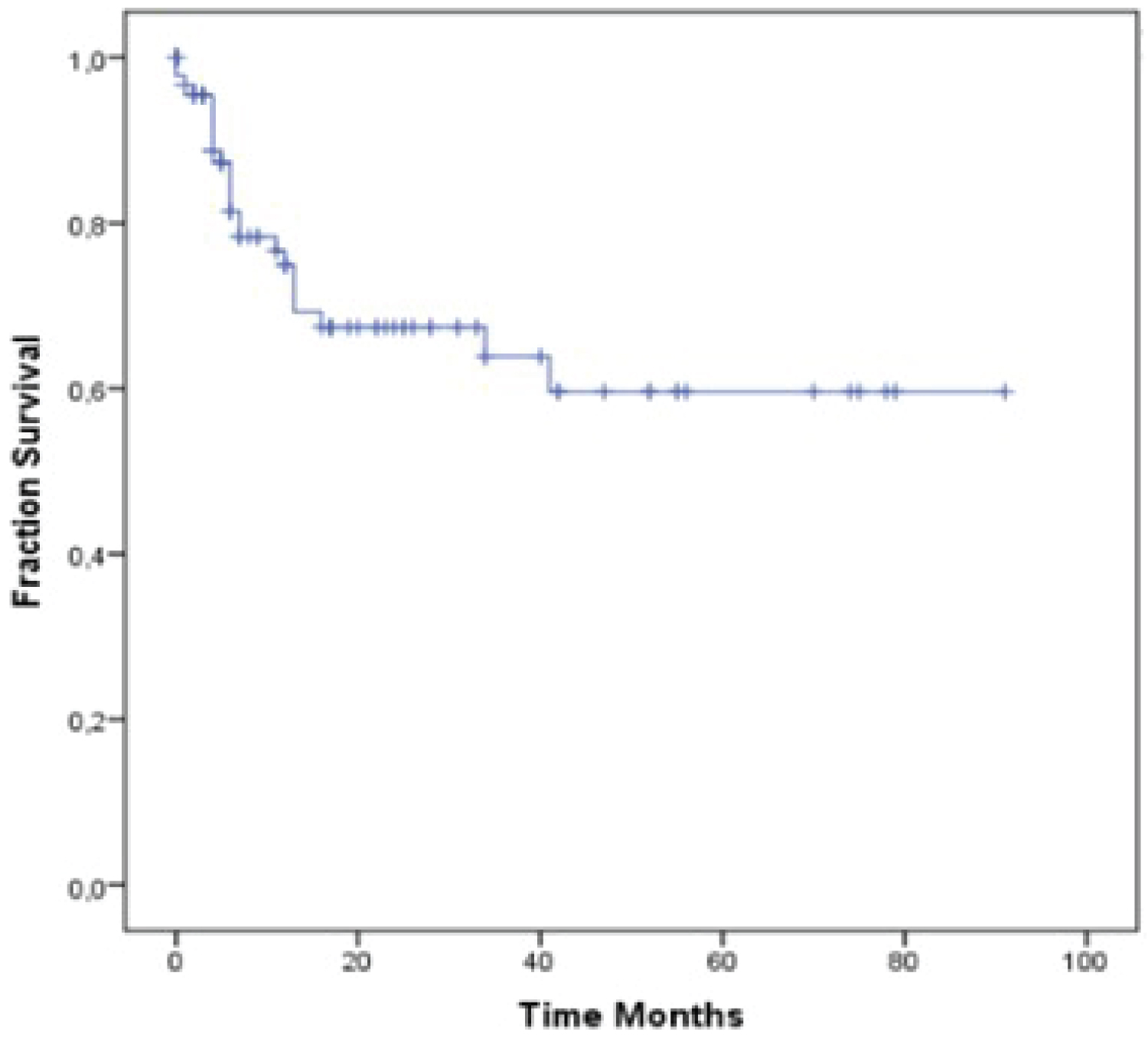 Figure 1: Overall survival estimated by Kaplan-Meier, in 5 years, of patients diagnosed in the Liga Norte Riograndense Contra o Cancer.
Figure 1: Overall survival estimated by Kaplan-Meier, in 5 years, of patients diagnosed in the Liga Norte Riograndense Contra o Cancer.
Source: Authors (2022).
View Figure 1
Table 3: Association between staging at diagnosis and mortality of patients followed by Liga Norte Riograndense Contra o Cancer. View Table 3
One of the world's highest incidences of penile cancer is found in India, with rates of 3.32/100,000 habitants, and the lowest is in Jews born in Israel, with an index close to zero, which is related to neonatal circumcisions [7,20].
The frequency of penile cancer in Brazil varies according to each region and is directly related to local socioeconomic conditions. The general relative incidence is 2.1% of male neoplasms, reaching 5.7% in the Northeast region, 5.3% in the North region, 3.8% in the Midwest region, 1.4% in the Southeast region, and 1.2% in the South region [7].
In this study, 72.2% of patients come from the state's interior, and 84.1% are illiterate or with incomplete primary education, presenting epidemiological characteristics similar to those described in other studies, especially those from developing regions whose socioeconomic reality is identical to that of Rio Grande do Norte State [1,2,21-23].
Unfortunately, the risk factors related to penile cancer could not be evaluated in the study due to a lack of data in medical records, which constitutes a constructive criticism of a complete patient anamnesis and history, not only for scientific collaboration but for better and comprehensive understanding and care for the patient, serving as a warning to health institutions about the importance of this [13,24-26].
Even so, we agree with the literature regarding the participation of phimosis, lack of adequate intimate hygiene, and smoking in develop and aggravation of penile cancer [3,4,13,20].
Although penile cancer is more frequent in the sixth decade of life [11] in this study, 18.5% of patients were diagnosed under 50. The occurrence of this neoplasm in earlier age groups serves as an alert to the importance of its research in younger patients with suspicious lesions [4,20].
Of note, 68% of patients were classified as T2 or higher, and 30% with lymph node involvement at diagnosis. These data are worrying, as it is well established that the advanced stage strongly correlates with the degree of invasion and the likelihood of regional and systemic metastases, leading to a worse prognosis for these patients [7,26].
Results of the analysis of the primary tumor were similar to those of Brazilian studies presented by Coelho, et al. (2018) (66.4%), Favorito, et al. (2008) (57.9%), and Couto, et al. (2014) (63.6%). However, these data are higher than those found in studies in developed countries, such as the United States (45.9 and 50.6%) [19,22].
The scarcity of publications reflects the low incidence of the disease in rich countries, and consequently, most of the works come from isolated institutions and with small casuistry. Thus, relevant questions regarding the clinical management of penile cancer remain open, including, until now, we do not have a Brazilian consensus [5].
As for the treatment, more than 90% of the patients underwent some surgical treatment with total or partial penectomy with or without inguinal lymphadenectomy. Furthermore, approximately 25% of patients were diagnosed with locally advanced or metastatic disease. These data demonstrate late diagnosis and delay in referral to specialized services, leading to more mutilating surgeries and palliative treatments [5,10,13].
None of the patients underwent neoadjuvant chemotherapy, a treatment reserved for adjuvant or palliative purposes only, although 18% of patients had classification N3 at diagnosis. The main chemotherapeutic agents used were cisplatin and 5-fluorouracil. Platinum- based triple regimens, until then considered standard, were used in isolated cases [23,24].
Lymph node involvement was present in 30% of the patients. However, only 6.5% underwent adjuvant radiotherapy. In unresectable local or locoregional recurrence cases, the most used treatment was radiotherapy with or without radiosensitizing chemotherapy. About 10% of patients relapsed, and 87.5% of cases for lymph nodes. Studies show that lymph node recurrence is one of the main factors of a worse prognosis in penile cancer [25,26].
In Table 2, we observe that mortality significantly worsened with staging. In that study, which had an average follow-up of 18 months, 12.5% of patients in stage I died, while 33.3% of patients in stage IV died in the same period, which more than doubled.
In addition, the socioeconomic and cultural profile of the carriers corroborates the fact that 25% of them were lost to follow-up after three months of diagnosis.
This neoplasm mainly affects men of low social class and education level, whose access to the reference health service is more complex. When they get medical care again, local and loco-regional recurrences are common [14].
Although the Liga Norte Riograndense is a philanthropic institution and has more than 90% of its patients from the public service network and, theoretically, the data from this study are overestimated for this population, this disease tends to affect patients with more precarious socioeconomic conditions, which makes early diagnosis and access to specialized services difficult [4,14].
To change this devastating scenario, national campaigns are essential, especially in the North and Northeast, to educate the population about this currently unknown neoplasm and alert Brazilian authorities about the importance of the topic.
In addition, the training of health professionals themselves and a diagnosis and treatment flowchart should also be prioritized, since in addition to the lack of knowledge related to the disease, the patient also finds it difficult to be diagnosed and obtain adequate follow-up and treatment, mainly through the SUS network (Sistema Único de Saúde) [13,14].
Nursing, within its competencies, plays a fundamental role in the promotion, prevention, and self-care of Men's Health, emphasizing primary care, where qualified listening is more present, and it is possible to interact, raise awareness and educate the community [14].
Considering only data from a single treatment center, Rio Grande do Norte has a high incidence of penile cancer with a high frequency of locally advanced tumors at diagnosis and in younger patients younger than 50. Since American and European studies describe penile cancer as a rare neoplasm.
Although most patients were diagnosed at an early stage of the disease, approximately 25% were diagnosed with locally advanced or metastatic disease, negatively influencing mortality outcomes.
Penile cancer is related to a low socioeconomic and educational level, which interferes with early diagnosis, and hinders access to specialized services, completion of treatment, and adequate follow-up. In addition, the lack of data collection records makes it impossible to elucidate the epidemiological profile of cancer better.
Due to the importance of Brazil in the world scenario for penile cancer, it is necessary to implement measures that allow prevention, early diagnosis, and treatment in addition to the role of leading clinical research to understand carcinogenesis better and obtain more effective therapies.
The authors thank the Federal University of Rio Grande do Norte, Potiguar University, and Liga Contra o Cancer for supporting this study.
Pro-Rectory of Postgraduate Studies - Federal University of Rio Grande do Norte - Natal - Brazil.
The authors declare that there is no conflict of interest.
Not declared.
Not applicable.
Research Ethics Committee of the North Riograndense Against Cancer League: 02089218.6.0000.5293.
We thank the entire multidisciplinary team involved in the study, the team that worked directly with the patients, and those who conducted this study. It is the science that moves the answers that the world needs, so we also thank everyone who moves scientific knowledge.
Thais Cristina Loyola da Silva and Érika Gabrielle Pinheiro Ximenes: Project writing, data collection, and final article writing; Ythalo Hugo da Silva Santos: Statistical data processing; Rodrigo Jerônimo Araújo, Eurides Araújo Bezerra de Macedo, Irami Araújo-Filho and Kleyton Santos de Medeiros: Study co-advisors; Tirzah Braz Petta: study advisor.