Despite declining rates for children under five years of age (U5M) in the last ten years, developing countries continue to challenge to meet Sustainability Development Goals (SDG) target, including reducing neonatal mortality to 12 deaths, and U5M to 25 deaths per 1,000 live births, by 2030. Cambodia, located in Southeast Asia, recently been reclassified by the World Bank as a lower middle-income country. Cambodia U5M has declined over the last decade, and Cambodia achieved the Millennium Development Goals; however, reaching the more ambitious SDG targets for child health requires tracking of progress to better focus additional public health efforts. To measure factors associated with U5M in Cambodia, we used data from the 2010 and 2014 demographic and health surveys, the retrospective cohort life table of child births for the five years preceding the surveys, and multivariate Weibull regression. Longer childbirth interval (> 2 years), maternal antenatal care visit at last birth, and children being fully vaccinated were associated with lower U5M; but, older maternal age, and higher education level of the mother associated with higher U5M. The study concludes that Cambodia should continue the current child health interventions, and suggests conduct a study on the association of mother's education and U5M.
Cambodia, Determinants of U5M, Demographic and health survey, Child health
Nearly six million children-under 5-years-old died in 2017 worldwide [1]. More than half of these early child deaths are due to conditions that could be prevented or remedied with access to simple, affordable interventions. Even though child survival has improved over the last ten years, the level of child mortality and morbidity remains unacceptably high, and many lower resource countries continue to face challenges to meet their targets for health-related Sustainable Development Goals (SDGs). For example, in sub-Saharan Africa alone, under-five mortality (U5M) is 15 times that of other developed regions. Responding to this burden, world leaders renewed their commitment for post-2015 "Sustainable Development Goals (SDGs)", which include reducing neonatal mortality to at most 12 deaths per 1,000 live births, and reducing U5M to at most 25 deaths per 1,000 live births, by 2030 [1]. To monitor this commitment, the Inter-agency Group for Child Mortality and the WHO-UNICEF Child Health Epidemiology Reference Group [1] produce annual reports with updated data. They have defined standard categories, methods and data sources for causes of child deaths in three major categories. First, vital registration provides annual data regarding neonatal, infant and under-five mortality rates; second, birth histories, mainly obtained through Demographic Health Surveys (DHS) provide estimates of neonatal, infant mortality rates and U5MR, typically for periods 0-4, 5-9 and 10-14 years prior to the survey; lastly, summary birth histories (DHS, other household surveys such as UNICEF, and population censuses) provide estimates of U5MR for time points covering roughly 2-12 years before the survey [2].
Cambodia, located in Southeast Asia, has an economy that has significantly progressed over the last two decades, with a Gross National Income (GNI) per capita of 1,070 US$ [3], Cambodia has now been reclassified by the World Bank as a lower-middle income country. The country has a mixed health delivery system. In addition to public health services, the private-for-profit sector is an important provider of health services and has grown rapidly over the past years. As of December 2014, there were over 8,000 formal private providers/facilities in the country; these facilities ranged from pharmacies and solo practice to specialized hospitals. Despite the existence of basic legislation, regulation of the private sector remains a challenge, mainly due to the institutional, informational, and financial capacity constraints. The private non-for-profit sector also plays an important role in health service delivery in Cambodia. Most of the local and international organizations work at grassroots levels (district and community) providing a range of services such as community-based health, health education, and health promotion activities [4].
In the last ten years, child health has gradually improved: coverage of complete vaccination (one dose of bacille Calmette-Guerin (BCG), three doses of diphtheria, pertussis (whooping cough), and tetanus (DPT3) and Polio) among children aged 12-23 months increased from 67% in 2005 to 73% in 2014, and Cambodia was certified as "measles free" by World Health Organization in May 2015 [4]. The U5M rate has declined from 117 to 35 per 1,000 live births between 1990 and 2015 [5]. However, this decline further needs public health attention in Cambodia to meet the 2030 SDG targets to include child survival as a part of the national priorities.
Several studies have been conducted to identify the determinants of U5M. Four countries in Africa: Ghana [6], Rwanda [7], Tanzania [8], and Zambia [9] used demographic health survey (DHS) to identify the determinants of U5M. They identified the following characteristics as being significantly related to children dying before the age of five: previous birth interval (< 2 years), birth order (> 7), maternal education (no education), and wealth quintile (lowest). Five countries in Asia: India, East-Timor, Lao PDR, Bangladesh and Nepal, have similarly used demographic health surveys to analyze determinants of U5M. India identified two main characteristics associated with of death before the age of five: birth order (> 7), mother's age at birth (< 20 years) [10]. They also found that child sex (boy) and residence (rural) were associated, but less strongly. In East-Timor, mother's age at birth (< 20 years), and wealth quintile (lowest) were associated with increased U5M rate [11]. In Lao PDR, the characteristics of children associated with increased U5M rate were: birth order (> 7), wealth quintile (lowest), previous birth interval (< 2 years), and maternal education (no education) [12]. Sex (boy), and previous birth interval (< 2 years) were also associated with increased U5M rate, but less strongly. In Bangladesh, mother's age at birth (< 20 years), and wealth quintal (lowest) were strongly associated with increased U5M [13]. Finally, in Nepal, previous birth interval (< 2 years), and wealth quintile (lowest) were associated with increased U5M [14].
This study aims to define persistent and emerging factors associated with U5M in Cambodia using demographic and health survey 2010 and 2014.
The 2010 [15] and 2014 [5] Cambodia Demographic and Health Surveys (CDHS) were population-based cross-sectional studies, and followed similar surveys conducted in 2000 and 2005. A total of 15,829 households were selected and 19,237 women were interviewed for the CDHS2010, and 16,356 households were selected, and 18,012 women were interviewed for the CDHS2014. The Woman's Questionnaire in both surveys has respondent background characteristics, reproductive health, including a complete birth and death history of respondents' live births and information on abortion, contraception, pregnancy, postnatal care and women's nutrition, immunization, children's nutrition and early childhood development, marriage and sexual activity, fertility preferences, husbands' background and women's work, domestic violence, HIV/AIDS and others. The details of the Woman's Questionnaire are provided in the CDHS reports [5,15]. Both surveys had response rates of 98 percent.
Approved and authorized by the Cambodia Ministry of Health (The National Institute of Public Health), we used both CDH survey data, "KHKR60FL & KHKR70FL, women files" to analyze the factors associated with U5M in Cambodia.
For both CDHSs, only women between the age of 15 and 49 with complete records of children born and complete maternal birth history were eligible to participate in the survey. Data of all births in the five years preceding the 2010 and 2014 CDHSs were used to create a synthetic cohort life tables for survival analysis. We used weights to restore the representativeness of the sample, and Weibull hazard regression (a multivariate life-table procedure, in STATA version 14). Results are presented as hazard ratios (HR), with HR greater than 1 indicating higher risk of mortality, and a 95% CI not including zero was used as the cutoff for statistical significance.
To guide the analytical plan, the authors used the adapted-Wiley H, Mosley 1984 conceptual framework of social, economic, political, and health system determinants of child survival. The dependent variable is U5M, and the independent variables are divided into four main characteristics, under the proximate factors [16] (Figure1).
Insert Figure 1 Here
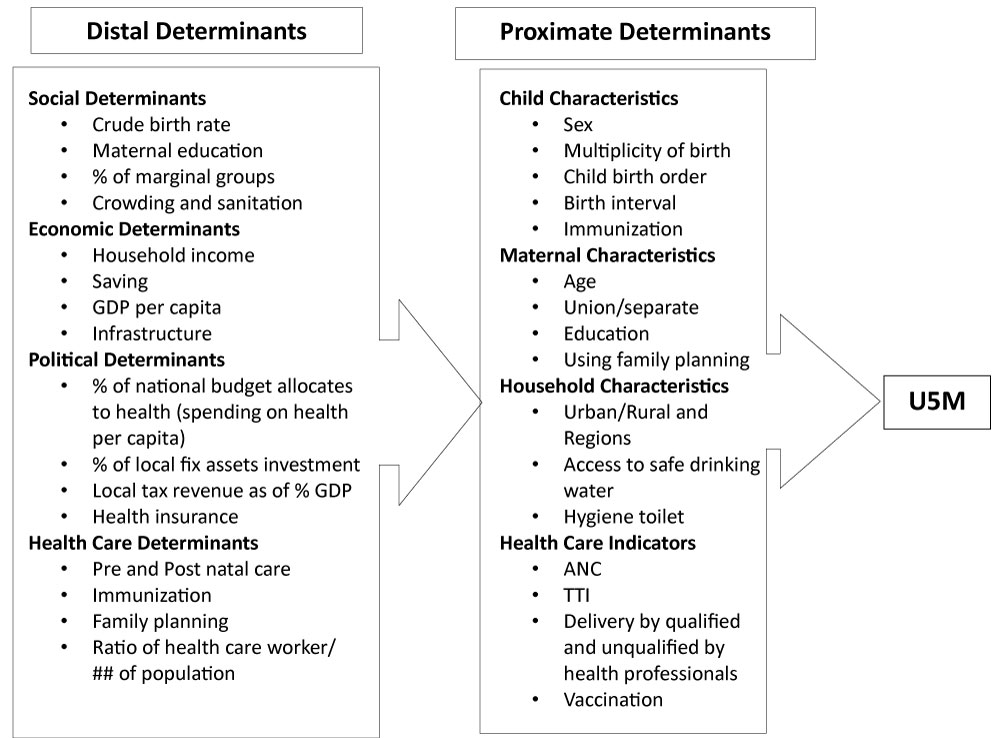 Figure 1: Conceptual framework of social, economic, political, and health system factors of child survival adapted from Wiley H. Mosley (1984). View Figure 1
Figure 1: Conceptual framework of social, economic, political, and health system factors of child survival adapted from Wiley H. Mosley (1984). View Figure 1
CDHS2010 had 8,232 eligible samples to analyze, and among those, 379 children under-five died; whereas CDHS2014 had only 7,165 samples eligible to analyze, and had only 175 children under-five died.
Effects of risk factors and confounders on U5M, (Table 1) present unadjusted and adjusted hazard ratio (HR) estimates of the effects of selected U5M's characteristics of CDHS2010 and CDHS2014. All selected characteristics variables are run in four models: Model 1: Child's Characteristics, Model 2: Child & Mother's Characteristics, Model 3: Child, Mother, Household's Characteristics, and Model 4: Child, Mother, Household and Health Care's Characteristics.
In Model 1 of CDHS2010, girls affected U5M less than boys. However twin baby's birth had almost 3 times greater risk than a single baby birth, and child birth order > 4 affected U5M almost 4 times higher than < 3 birth order. A long birth interval > 2 years had a lower risk of U5M. The results of CDHS2014 were almost similar for the three child characteristics, but differed for twin baby's birth, which had an almost 3.5 times higher risk than single baby birth, and statistically significant.
In Model 2 of CDHS2010 and 2014, the results remained unchanged for children characteristics. The four selected mother's characteristics of children death showed that children born from old mother (> 40-years-old) were almost 3 times more likely to die than children born from younger mothers (statistically significant). Currently in union mothers affected U5M slightly less (0.98 times). Mothers with higher education (secondary and higher) had less effect (0.70 times) on U5M than mothers with no or primary education. Children born from mothers currently using a family planning method had negative risk (0.62 times) compared with mothers not using (statistically significant). Model 2 of CDHS2014 of the four selected mother's characteristics results were nearly similar to those of CDHS2010.
Model 3 shows that the child and mother's characteristics of children death were slightly changed, but not noticeably. Model 3 of CDHS2010 shows that children from mothers who live in rural areas had a 1.53 times greater risk of U5M than mothers who live in urban areas; similarly, children from mothers who live in Plain, Coastal, and Mountain/Plateau regions had from 2-4 times higher risk of U5M than mother who live in Phnom Penh, the capital city of Cambodia. This result is statistically significant for all regions except for the Great lake region. Access to safe drinking water, and toilet facilities reduced the risk to U5M. However, in CDHS 2014, children born from mothers who live in rural areas, had a 3.5 times greater risk of U5M than mothers who live in urban areas (statistically significant), and also children born from mothers who live in Plain, Great lake, Coastal regions, and Mountain/Plateau regions had lower risk to U5M than mothers who live in Phnom Penh (but statistically not significant). Similarly to CDHS2010 results, children born from mothers who have access to safe drinking water, and toilet facility had lower risk to U5M.
Model 4 of CDHS2010 shows that child, mother, household's characteristics of children death are slightly changed. Girls had lower risk of U5M than boys (HR = 0.95; 95% CI: 0.74-1.22). Twin baby remained at risk to U5M (HR = 2.08; 95% CI: 1.05-4.13). Children born in the 3rd birth order had lower risk than other birth orders (HR = 0.80; 95% CI: 0.46-1.40), and children born from a long birth interval 2-3 years and > 3 years had lower risk than a birth interval < 2 years (HR = 0.49; 95% CI: 0.32-0.76), and (HR = 0.59; 95% CI: 0.41-0.86). Children born from an older mother (> 40-years-old) were still highly associated with U5M (HR = 3.55; 95% CI: 1.80-7.03). Currently in union mothers affected U5M slightly less (HR=0.88; 95% CI: 0.51-1.54). However, mothers with primary education (1.4 times) and secondary and higher education (1.8 times) had more association with U5M than mothers who had no education with statistical significant (95% CI: 1.04-1.91) and (95% CI: 1.16-2.97). Children born from mothers who are currently using a family planning method had slightly lower risk (HR = 0.94; 95% CI: 0.71-1.24). Children born from mothers who live in rural areas had greater risk of U5M (HR = 1.37; 95% CI: 0.91-2.06), similarly in Plain region they had higher risk of U5M compares to other regions (HR = 2.92; 95% CI: 1.15-7.39). Children born from mothers who have access to safe drinking water had slightly lower risk of U5M (HR = 0.90; 95% CI: 0.68-1.19), but children born from family who had a toilet facility had a slightly higher risk of U5M (HR = 1.29; 95% CI: 0.90-1.84). Children from mothers who seek ANC had a negative association with U5M (HR = 0.42; 95% CI: 0.29-0.62), and mothers who received one dose of tetanus toxoid TT (HR = 0.70; 95% CI: 0.41-1.17) and two doses (HR = 0.66; 95% CI: 0.45-0.97), and whose babies were delivered by qualified trained health professionals (HR = 0.98; 95% CI: 0.71-1.35). Children without full immunization were associated with U5M (HR = 1.64; 95% CI: 1.40-1.93). Children from family with or without health insurance had no association with U5M.
Model 4 of CDHS2014's results changed slightly. Girls had less risk to U5M than boys (HR = 0.74; 95% CI: 0.50-1.08). Twin babies were more at risk (HR = 1.93; 95% CI: 0.87-4.25). Children with childbirth order 2, 3 and > 4 had greater U5M risk (around 2 times) than the 1st birth order (but statistically not significant). Long birth interval 2-3 years, and > 3 years had lower risk than birth interval < 2 years (HR = 0.48; 95% CI: 0.24-0.95), and (HR = 0.47; 95% CI: 0.25-0.87). Children from older mothers (> 40-years-old) had a higher risk than children from younger mothers (HR = 3.21; 95% CI: 1.13-9.08). Currently in union mothers affected U5M slightly less (HR=0.94; 95% CI: 0.43-2.06). However, children from mothers who have secondary and higher education were associated with U5M around 2 times that of mothers with no education (statistically significant 95% CI: 1.05-3.62). Children born from mothers currently using a family planning method had lower risk (HR = 0.64; 95% CI: 0.44-0.94), but had greater risk from mothers who live in rural areas (HR = 2.99; 95% CI: 1.28-6.97). However, children born from mothers who live in Phnom Penh had higher risk than living in the four regions. Children born from mothers who have access to safe drinking water had slightly risk to U5M (HR = 1.05; 95% CI: 0.69-1.59); however, children born from mothers whose household has toilet facilities had a slightly lower risk to U5M (HR = 0.75; 95% CI: 0.46-1.23). Children from mothers who seek antenatal care (ANC) had a much lower risk (HR = 0.33; 95% CI: 0.18-0.59). However, children from mothers who received > 2 doses of TT and were delivered by qualified trained health professional had higher risk to U5M around 1.5 times (but statistically not significant). Immunization affected U5M, it is 4 times higher than children who do not have immunization, with 95% CI: 3.13-4.86. Children from family with health insurance had association with U5M, but statistically not significant.
Insert Table 1 Here
Table 1: Unadjusted and Adjusted Hazard Ratio Estimates of the Effects of Selected Under-five Mortality's Characteristics among Children who born in the Five-year Period Preceding the Survey, CDHS2010 and CDHS2014. View Table 1
The results of the CDHS2010 and CDHS2014 show that U5M in Cambodia has declined, and met millennium development goal. The analysis of the two surveys presents that among proximate factors of the study's conceptual framework (adapted from Mosley and Chan-1984), some factors are persistent from 2010 to 2014 and some are emerging factors in the 2014 survey.
Persistent factors are associated with U5M, including child birth intervals 2-3 years and > 3 years are statistically significant and negatively associated with U5M, which is similar to the study's results using DHS data from 52 DH surveys conducted from 2000 through 2005, the risk of dying decreases with increasing birth interval lengths up to 36 months [17].
Older maternal age (> 40-years-old) is associated with increased U5M. Old mothers have biological and physical disadvantages during gestation and also childbearing, which lead to increased U5M. Our study findings are consistent with the results of many studies [17,18].
In most of the studies, mother's education has lower risk of U5M [19,20], which is contrast with the study results. One possible explanation of this result is having a proper health education will lead to proper knowledge and practices, however within the last ten years, Cambodia has opened its economic horizon and has limited ways to control the health education contents in media, especially social media from private sector. The second explanation is the study collects only children death but does not review the results of recovering sick children from mother with primary and secondary education levels.
Health seeking mothers, especially during pregnancy have been shown to have positive impact on child survival, mothers gain from taking care of her health and her baby, through getting a health education "mother class" that also addresses problems of her gestation. In previous studies, the association of antenatal care with lower childhood mortality has been documented [18,21], which is similar to the survey's findings.
Children not fully immunized were at a greater risk of U5M, in CDHS2010 only almost 2 times, but it increased to almost 4 times in CHS2014. These results are consistent with several studies [22-24].
Emerging determinants to U5M, children from mothers who are currently using a family planning method had lower risk to U5M, which is similar with a few studies' results [25-27].
Children from mothers who live in rural areas were associated with high U5M compared to those who live in urban areas. Similar results are presented in these studies [7-9]. In CDHS2014 children born from mothers who live in Phnom Penh had higher risk of U5M than mothers who lived in other regions; this may be associated with a migration issue.
DHS dataset was collected for live births during the five years preceding the surveys, so the analysis is limited to only variables in the data set. Changes of socioeconomic status and health and health care indicators may also help to explain the declines in U5M in recent years but were not available for the analysis. DHS is the cross-sectional and retrospective study design, rather than panel data designed for a prospective longitudinal analysis. The CDHS was conducted at five-year intervals, and completely different women were sampled in the 2010, 2014 surveys. The mortality data are retrospective cohort data, so some of the covariates are associated directly with the time of the child's birth and not the time of death (multiplicity of birth, delivery assistance, and mother's age at childbirth). Others reflect conditions at the time of survey that are not the same at the time of the child's birth or death (mother's level of education, marital status, use of contraceptive, household sources of water, type of toilet). To overcome these limitations, the analysis used changes (differences) in covariates between two surveys as the predictors changes between 2010 and 2014. Moreover, even though data are not panel data designed for longitudinal analysis, all samples are very large and representative at national, urban-rural, and regional levels, with statistical power sufficient for the finding to be generalized, and the use of Weibull regression model analysis helps address these limitations.
No doubt that U5M rate in Cambodia dropped significantly from 2010 to 2014. However to continue the trend, in addition to the current interventions and services, we need to pay more attention to the persistent and emerging determinants, and to mothers who live in rural areas. In particular, the government needs to make more efforts to minimize the gap of health services and living conditions between rural and urban areas, and to address issues of Phnom Penh's migrants. Because mother's education has been one of persistent determinants in 2010 to 2014 surveys and the results are contrast with the some studies that affect U5M, an in-depth study focus on this topic is suggested.
The authors would like to thank to Mr. Jean-Luch Lebrun and Dr. Robert Newman for the review and edition the English and the content of the manuscript.
No conflict of interest.