A literature review reveals that neck pain is more commonly associated with migraine than is nausea, that reduced neck muscle function and reduced cervical range of motion are present in migraineurs that are not documented in those without migraine, and that there is pharmacological overlap in the treatment response of migraine and neck pain associated with migraine.
We report the case of a teenage girl with right-sided migraines without aura whose symptoms resolve over a 3-month period in response to a therapeutic neck exercise program.
A structured therapeutic neck exercise program decreased migraine frequency from 8 migraine days per month to 0 migraine days in the last 11 weeks of our patient's 4-month treatment period. This result raises the question of to what extent a therapeutic neck exercise program might offer similar relief to other migraineurs.
Migraine, Neck pain, Therapeutic neck exercises, Trigeminocervical nucleus, Cervical spine
OB/Gyn: Obstetrician/Gynecologist; mg: milligrams; b.i.d.: twice a day; HIT-6: Headache Impact Test; MSK: musculoskeletal; MRI: Magnetic Resonance Imaging; ROM: Range of Motion; AMA: American Medical Association
Neck pain is more commonly associated with migraine than is nausea, which is considered to be one of the defining characteristics of migraine headache [1]. Many studies document reduced neck muscle function and reduced cervical range of motion in those with migraine [2-5]. And in a study with fascinating implications for the role of neck problems in migraineurs, 75% of 144 patients with migraine with or without aura reported neck pain with their migraines. The neck pain was unilateral in 57% of patients, and 98% of these had neck pain on the same side as their headache. A subset of 30 patients from this study used Sumatriptan or a similar triptan to treat 278 headaches, 231 of which were accompanied by neck pain. The percentage of attacks with a pain-free response 2 hours after dosing was 68% for head pain and 73% for neck pain [6].
Building on these observations, the present case report describes the effect of a structured therapeutic neck exercise program on migraine frequency in a teenaged girl with a 15-month history of right-sided migraine without aura.
A 15-year-old teenage girl was referred by her OB/Gyn to our headache clinic in February 2020 for evaluation of severe right-sided migraines which had caused her to miss 2 weeks of school in February. The patient had initially developed a severe 12-day headache in November 2018. She was evaluated by a pediatric neurologist and was diagnosed and treated for migraine without aura with Topamax. The Topamax significantly reduced her headache frequency at a dose of 50 mg b.i.d., but it gave her symptoms she was unable to live with, including inability to think clearly and marked lethargy. This dose was gradually tapered to 25 mg daily, at which time her headaches increased in frequency and severity in January of 2020. Diamox was added to her treatment by her neurologist, but she did not tolerate side effects. Propranolol was started on 2/17/20, and her headaches were unchanged at the time of her first appointment with us on 2/26/20. A complete medication list can be seen in Table 1.
Table 1: Patient medication use at initial appointment, during treatment and at the end of treatment. View Table 1
The patient described her pain as primarily throbbing in quality. Activity worsened the intensity of her headaches, and headache severity caused her to miss school. Her headaches started in her right temple and then spread to the whole right side of her head from the base of her skull through her head, temple, forehead and into her right eye. Her worst headaches were accompanied by photophobia and dizziness. She denied phonophobia, sensitivity to smell, nausea or focal neurological symptoms. She was getting this type of headache 4 days a week at the time of her initial appointment with us. There was a family history of migraine in her grandmother. If she took sumatriptan 50 mg at the onset of these headaches, it made her go to sleep, and she would waken 2-3 hours later with significant headache relief. She was using 8 sumatriptan per month for her most severe migraines at the time of her initial visit to our clinic.
In addition to headaches, the patient described daily neck tightness. Headache triggers included neck pain or tightness, shoulder tightness, and stress. Her HIT-6 Score (Headache Impact Test) at her first appointment was 76, indicating very severe life impact. Patient and patient's mother consented to participation in this case study report.
The patient's medical history includes neurally mediated syncope, anxiety, iron deficiency anemia and allergic rhinitis. The patient lives with her parents and younger sister and attends high school. She does not drink alcohol, smoke or use non-prescription drugs. She was on the school swim team until she had surgery to repair a left labrum tear (2019). She reports getting at least 8 hours of sleep a night.
Patient was normotensive and afebrile with positive MSK findings indicated in Figure 1. Brain MRI (2018) and C-spine MRI (2020) were normal.
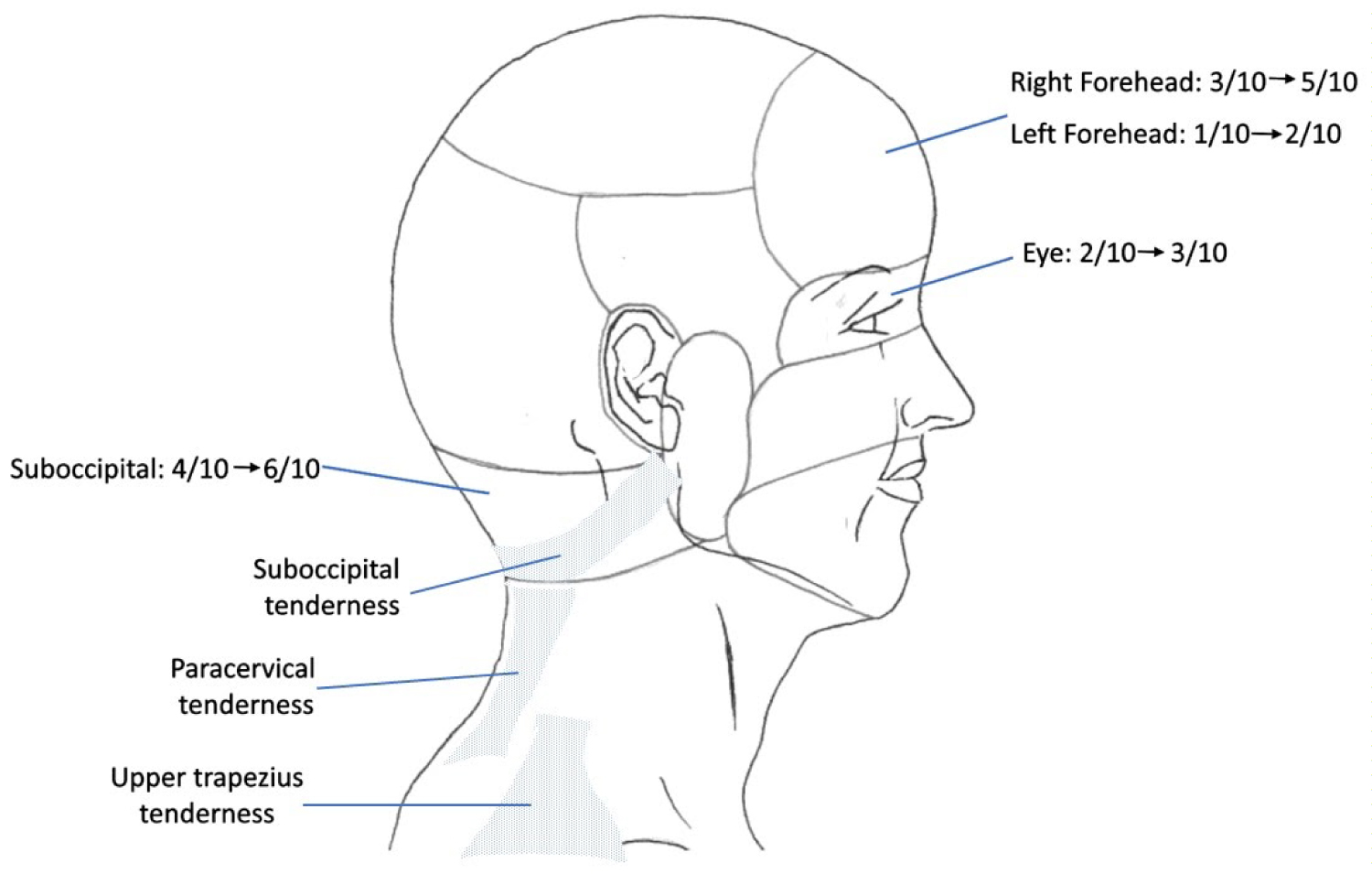 Figure 1: Change in symptom intensity at designated location in response to cervical flexion and protrusion (0-10 verbal pain rating scale), and areas that were tender to palpation (shaded).
View Figure 1
Figure 1: Change in symptom intensity at designated location in response to cervical flexion and protrusion (0-10 verbal pain rating scale), and areas that were tender to palpation (shaded).
View Figure 1
The patient went through a therapeutic neck exercise protocol (outlined in Appendix A) starting 3/17/20, spending approximately 45 minutes in the office at each visit. At each appointment, the current location and intensity of the patient's head and face pain was recorded for each of 10 locations (Figure 2) corresponding to a map that divided the head and face into 10 different areas. Then, under the instruction of the physician, the patient was instructed to perform repeated neck movements and/or sustained neck positions. As the patient performed these neck movements and positions in the office, the zone distal-most from the neck was observed (zone 10 is most distal from the neck). If the patient-reported intensity of the distal-most zone was decreased or abolished, this was viewed as a favorable response. The neck movements and positions that resulted in this therapeutic response were then assigned to the patient as a home exercise program. Neck exercise progression was determined through the use of an algorithm which was driven by patient symptom response. Changes in sleep posture were suggested to avoid neck-unfriendly positions, including sustained cervical rotation (i.e. as in prone sleeping, which was to be strictly avoided).
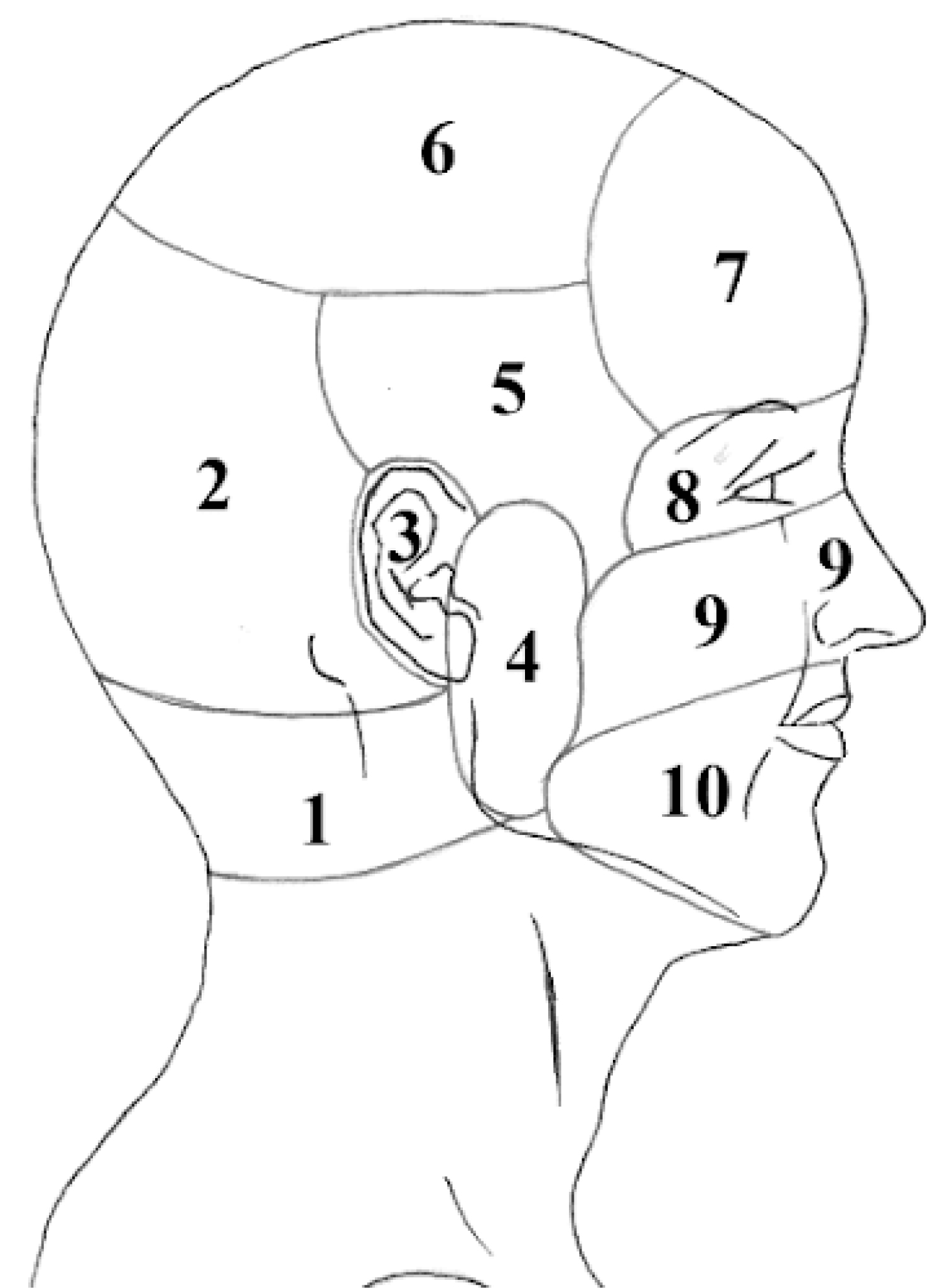 Figure 2: 10 Zones of Pain Relief. Used with permission from Angelo DiMaggio, PT, Dip.MDT, Spine Therapist, whose treatment approach forms the foundation of our neck exercise treatment protocol.
View Figure 2
Figure 2: 10 Zones of Pain Relief. Used with permission from Angelo DiMaggio, PT, Dip.MDT, Spine Therapist, whose treatment approach forms the foundation of our neck exercise treatment protocol.
View Figure 2
Adherence: The patient reports completing their assigned neck exercises an average of 5 out of 6 times per day for the duration of treatment.
Adverse events: The patient was able to tolerate all of the assigned neck exercises without any discomfort or adverse events.
We advise the use of ginger for acute migraine treatment in our practice based on a double-blind, randomized clinical trial of 100 migraine headache patients which showed that ginger was equally as effective as 50 mg of Imitrex in achieving migraine headache relief within 2 hours after ingestion [7]. Two other studies by Cady, et al. [8] and Aurora, et al. [9] demonstrate the effectiveness of migraine relief with ginger and feverfew preparations.
As with treatment for any other chronic condition, education was provided regarding important lifestyle factors such as sleep, diet, exercise and stress management. The treatment period has been 17 weeks.
The patient reported 16 migraine days in the 30 days preceding the start of her neck exercise program. She reported 0 migraine days in the last 30 days of treatment. She had been migraine free for a total of 11.4 weeks at the time of her most recent appointment on 06/23/2020.
Our patient first replaced her acute migraine and headache medications, Sumatriptan and Tylenol, with ginger, which provided effective acute headache relief. The improvement in migraine frequency that she experienced with her therapeutic neck exercise program allowed her to discontinue ginger, Tylenol and Sumatriptan in the final 7.8 weeks of treatment (see Table 1). The patient did not experience any adverse events from the recommended change in medications.
The patient's initial HIT-6 score of 76 (severe life impact) decreased to a score of 55 (some life impact).
The patient's pain-free cervical extension ROM, measured using dual digital inclinometers according to AMA guidelines, increased from 35 degrees to 62 degrees over the course of her therapeutic neck exercise program.
While current thinking has evolved beyond the idea that vascular dysregulation is the cause of migraine, newer theories are still focused on brain-based causal mechanisms for migraine, specifically on brain neuron dysfunction as the underlying cause in migraine pathophysiology. Reflecting this focus is a comment in a recent review of the pathophysiology of migraine which states that therapeutic efforts for migraine prevention are likely to face a large challenge "given that migraine can originate in an unknown number of brain areas, and is associated with generalized functional and structural brain abnormalities" [10].
Nothing in the current understanding of brain-based causality of migraine can explain the unilaterality of migraine pain. Unilateral neck problems, however, have been demonstrated to cause unilateral headaches [11,12], and unilateral neck pain has been correlated with migraine, with both migraine pain and neck pain decreasing in intensity upon treatment with a triptan [6].
This case report documents the effectiveness of a structured therapeutic neck exercise program in reducing migraine days from 16 days per month to 0 days per month over a 17-week course of treatment in a therapeutic neck exercise program. The patient was able to discontinue use of her acute headache relief medications: Sumatriptan 50 mg, Tylenol, and ginger. The patient's pain-free cervical extension ROM increased from 35 to 62 degrees, and her daily neck pain resolved.
These results invite further investigation into the role of cervical structures in migraine pathophysiology. Progression through the therapeutic neck exercise treatment algorithm is what we believe is responsible for not just the decrease in head and face pain that we saw and recorded at each appointment (see description in Therapeutic neck exercise program), but also for the final decrease in migraine frequency that we document in this case report. These results encourage further investigation into the role of the cervical spine in generating migraines.
Nasha Holt, MD, sees patients in a headache practice that uses the therapeutic neck exercise method that is being analyzed in this study. Codie Kurka, MS, has no conflict of interest to report.
We gratefully acknowledge the expertise and dedication of Angelo DiMaggio, PT, Dip.MDT, Spine Therapist, whose treatment approach forms the foundation of our neck exercise treatment protocol, and of his protégé, Jeff Turner, DPT, Dip. MDT, who has collaborated with us in patient care for many years.