Mesenteric lipoma is rare, no more than 50 cases were reported. They usually occur in the superficially trunk or extremities. They are the most common soft tissue tumors and usually asymptomatic. We reported a 60-year-old male with complaint of abdominal fullness and nausea for two days. The image studies showed mesenteric lipoma that caused compression of the intestine and obstruction. After nasogastric tube decompression and fluid supplement, the symptoms relived. We suggested of surgical intervention. However, the patient refused. We report a rare case that mesenteric lipoma induced intestinal obstruction.
Lipoma, Mesenteric lipoma, Intestinal obstruction
Lipoma is a very common benign tumor, occurring throughout the whole body [1]. It may be single or multiple and may occur as a superficial (subcutaneous) or deep-seated tumor. The aim of this paper is to report a case with mesenteric lipoma and cause bowel obstruction.
A 60-year-old male patient complained of abdominal distension and nausea for two days. He had medical history of hypertension, but no surgery.
In our emergency room, physical examination revealed, diffuse tympanic sound while percussion. General laboratory examinations were in normal range. Abdominal plain film showed suspicious of a radiolucent mass (Figure 1, black arrow) and the bowel loops were displaced up and down. The proximal jejunum was dilated (Figure 1, white arrow). Ultrasound of abdomen showed a hypoechoic mass well-margin (Figure 2, arrow). Computed tomography (CT) of abdomen showed a mass-like lesion compressed the intestine and caused proximal bowel loops dilated (Figure 3, arrow). Initially, we though the mass-like lesion as free air. After adjustment of the contrast of CT, we found an encapsulated fatty component mass-like lesion over the mesentery in the lower abdomen (Figure 4, arrow).
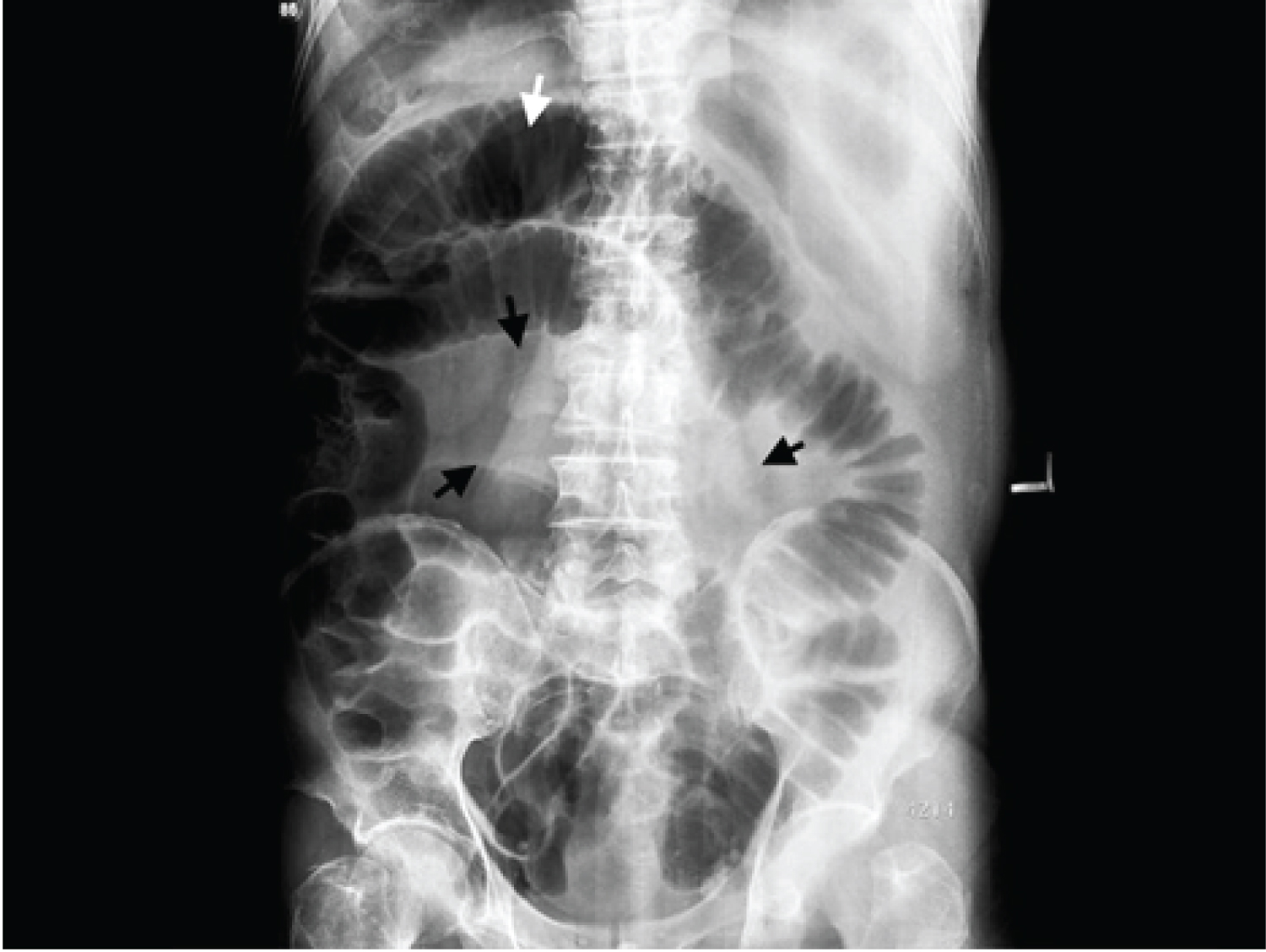 Figure 1: Abdominal plain film showed suspicious of a radiolucent mass (black arrow) and the bowel loops were displaced up and down. The proximal jejunum was dilated (white arrow).
View Figure 1
Figure 1: Abdominal plain film showed suspicious of a radiolucent mass (black arrow) and the bowel loops were displaced up and down. The proximal jejunum was dilated (white arrow).
View Figure 1
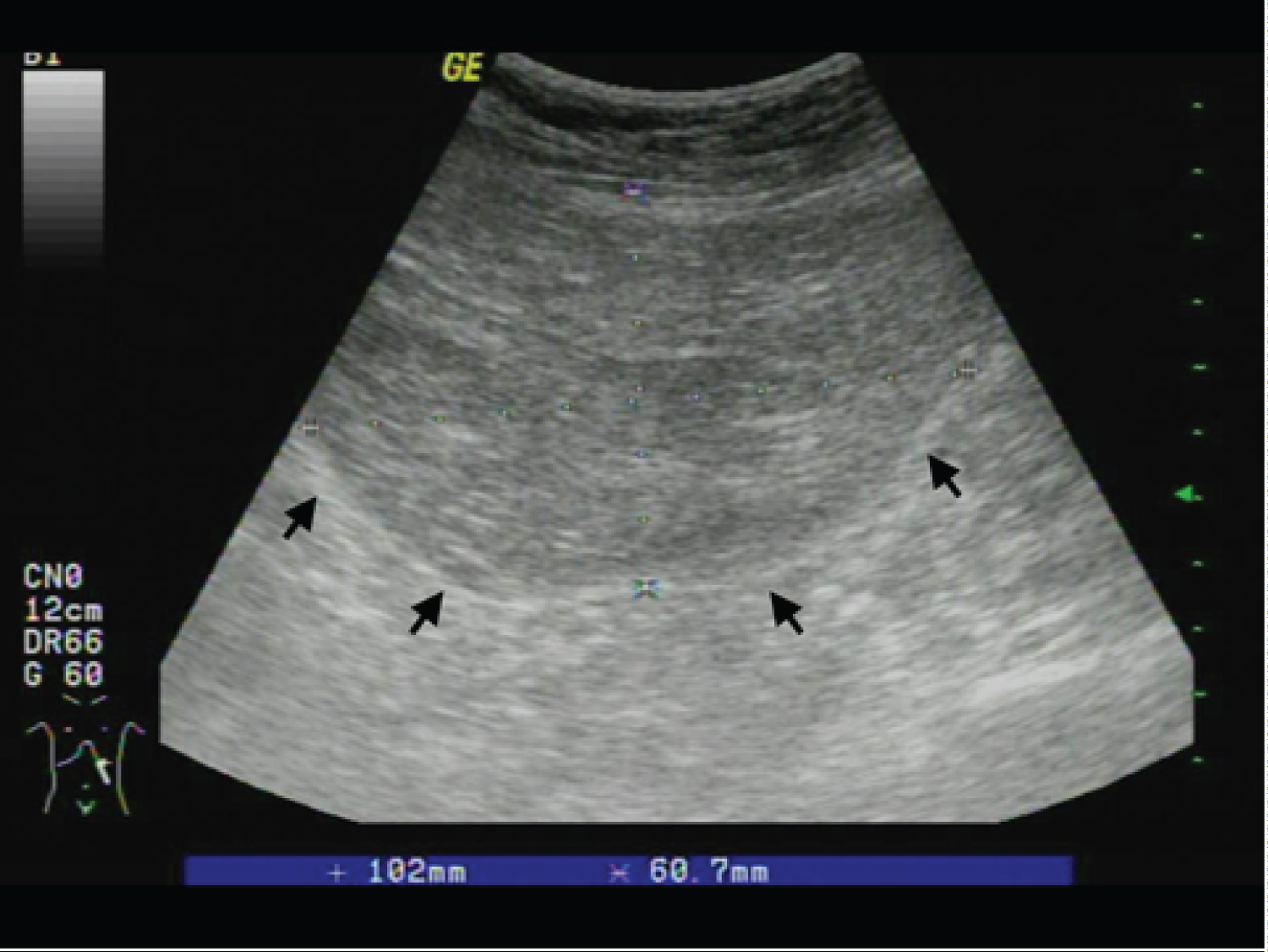 Figure 2: Ultrasound of abdomen showed a hypoechoic mass well-margin (arrow).
View Figure 2
Figure 2: Ultrasound of abdomen showed a hypoechoic mass well-margin (arrow).
View Figure 2
 Figure 3: Computed tomography (CT) of abdomen showed a hypodense lesion compressed the intestine and caused proximal bowel loops dilated (arrow).
View Figure 3
Figure 3: Computed tomography (CT) of abdomen showed a hypodense lesion compressed the intestine and caused proximal bowel loops dilated (arrow).
View Figure 3
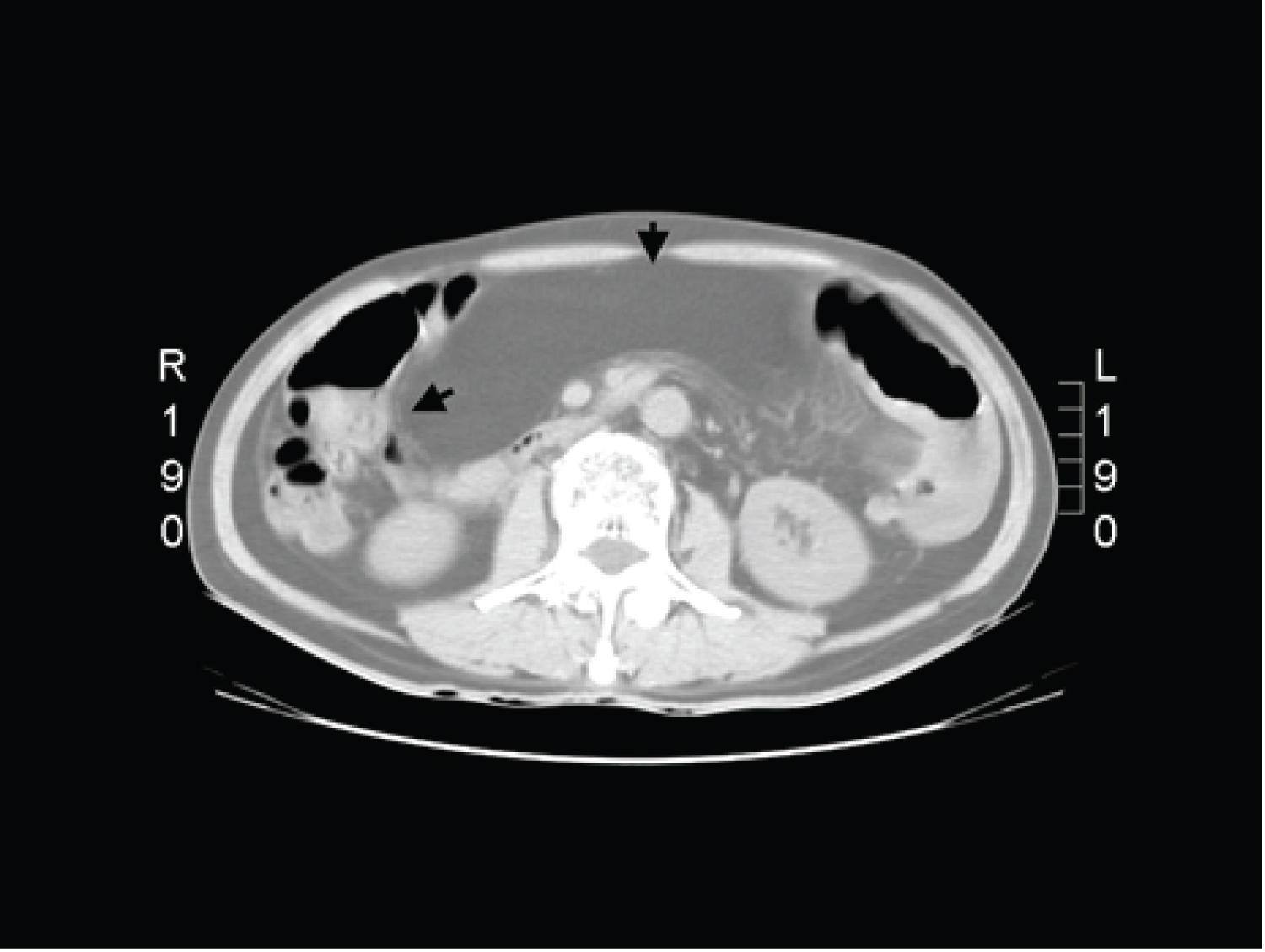 Figure 4: Computed tomography (CT) of abdomen: Initially, we though the mass-like lesion as free air. After adjustment of the contrast of CT, we found an encapsulated fatty component mass-like lesion over the mesentery in the lower abdomen (arrow).
View Figure 4
Figure 4: Computed tomography (CT) of abdomen: Initially, we though the mass-like lesion as free air. After adjustment of the contrast of CT, we found an encapsulated fatty component mass-like lesion over the mesentery in the lower abdomen (arrow).
View Figure 4
Nasogastric decompression was performed. Two days later, the patient's symptoms relieved. We suggested of surgical intervention. However, the patient refused and was discharged three days later.
Mesenteric lipoma is rare. Fewer than 50 cases have been documented [1-8], and those causing bowel obstruction make up only a small percentage [1]. Most of the patients were often hard to be detected because of their slow growth and usually asymptomatic [1].
While the size of tumor is small, it's usually not space-occupied. It would compress the bowel loops once the tumor enlarged enough. The tumor of our patient is over than 10 cm, it compressed the bowel loop. Owing to the tumor is soft and movable, the intestinal obstruction are often partial. Although our patients developed intestinal obstruction, it could be easily relieved by nasogastric tube decompression.
The small tumors may not easily been detected by X-ray and ultrasound. Emergency abdominal CT is now the most common way of identifying extraluminal or intraluminal lesions causing small bowel obstruction [3]. However, we have to check the contrast number of abdominal CT. In Figure 3, we initially misunderstood the lipoma as free air. After adjusting the contrast number shown in Figure 4, we could see a fat contain mass-like lesion. Clinician should pay more attention to the well-defined margin lesion to prevent from misdiagnosis.
Although the patient would not receive surgical intervention and the benign nature of the tumor. We suggested that surgery may be indicated because it sometimes caused volvulus or ischemic change of bowel loops [3].
In conclusion, lipoma may occur in abdomen and can cause intestinal obstruction of ischemic change of bowel. Carefully awareness of the distinctive picture of image is important to prevent from misdiagnosis. Complete resection is the treatment of choice.