Sinus histiocytosis with massive lymphadenopathy (SHML) (Rosai Dorfman disease) is a disorder first described in lymph nodes but eventually has been described in many organs. Liver involvement is rare and is a great mimicker of infection, metastases or a lymphoma which commonly involve the liver. We describe a case of a middle-aged female who presented with abdominal pain in the emergency. CT scan of the upper abdomen showed multiple hypodense lesions in the liver, pancreas, left sacral ala and multiple enlarged lymph nodes were also noted suggestive of metastases. Excision biopsy revealed the presence of SHML. Since SHML is a great mimicker of other disorders especially malignancy, a high index of suspicion and correlation with tumour markers is necessary to make a correct diagnosis.
Sinus histiocytosis with massive lymphadenopathy (SHML) (Rosai Dorfman disease) is a disorder first described in lymph nodes but eventually has been described in many organs. Liver involvement is rare and it is a great mimicker of infection, metastases or a lymphoma which commonly involve the liver. We describe a case of a middle-aged female who presented with abdominal pain in the emergency. CT scan of the upper abdomen showed multiple hypodense lesions in the liver, pancreas, left sacral ala and multiple enlarged lymph nodes were also noted in the periportal, peripancreatic, precaval and paraaortic region. The above imaging findings were suggestive of metastases. The excision biopsy was done to identify the nature of the tumour which revealed the presence of SHML.
A forty-year-old lady presented with abdominal pain in the emergency. Computed Tomography scan of the upper abdomen showed multiple hypodense lesions (upto 2 cm) in the liver, one in the pancreas (1.5 × 1.2 cm) (Figure 1) and multiple enlarged lymph nodes were also noted in the peri-portal (3 × 2.6 cm), peri-pancreatic, pre-caval and para-aortic region. Also, there was a lytic lesion in the left sacral ala measuring 1.8 × 1.8 cm. The above imaging findings were suggestive of metastases. Her bilirubin levels were normal but her serum gamma glutamyl transpeptidase and alkaline phosphatase levels were increased 113 and 208 U/L respectively. Serology for Hepatitis C virus (HCV), Human immunodeficiency virus (HIV) and Hepatitis B surface antigen (HbsAg) was negative. The tumour markers were within normal limits. Fine needle aspiration cytology was inconclusive. So, an excision biopsy was done to identify the nature of the lesion.
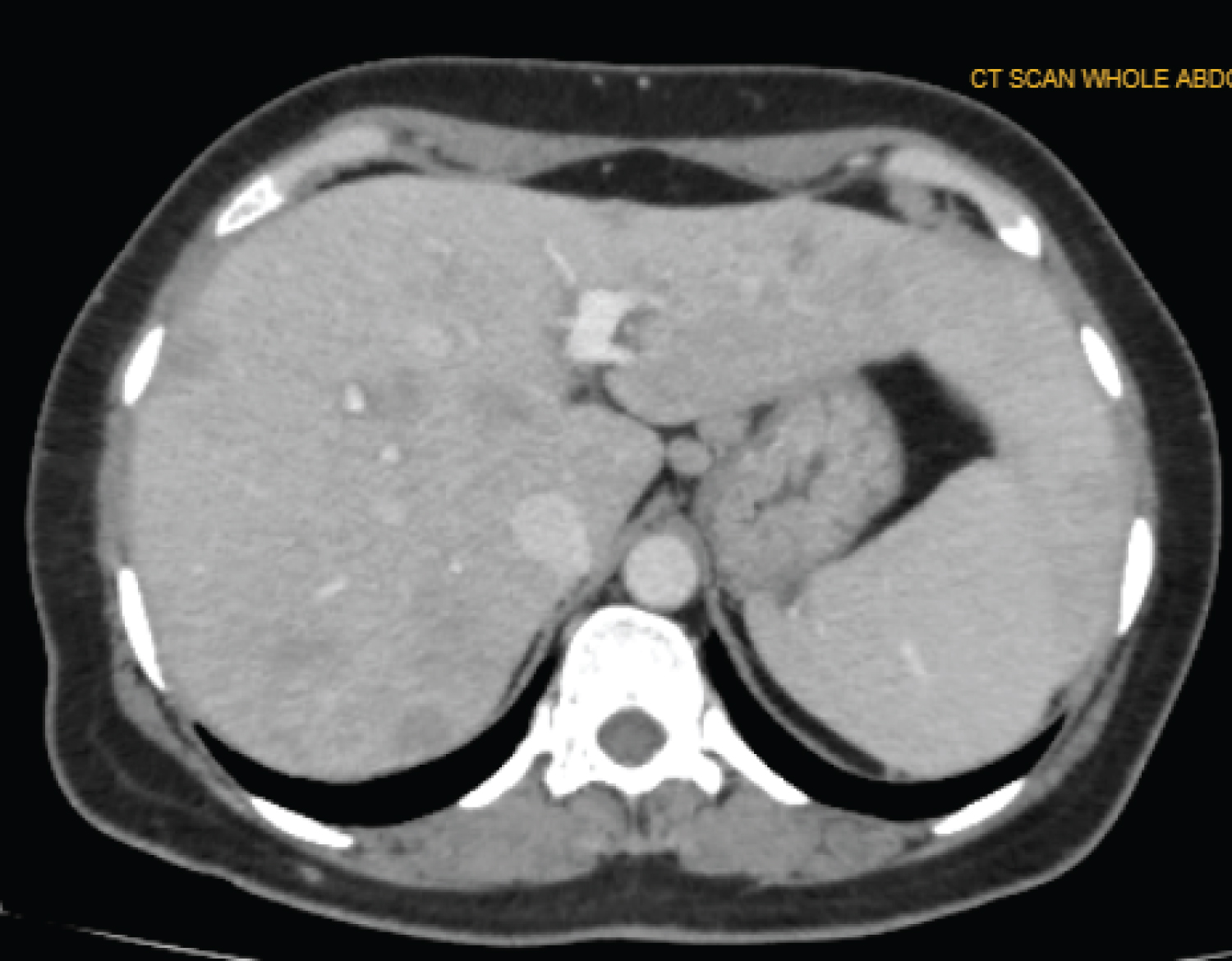 Figure 1: Multiple hypodense lesions in the liver.
View Figure 1
Figure 1: Multiple hypodense lesions in the liver.
View Figure 1
The light microscopy showed plump cells with vesicular nuclei, positive for S100, CD68, and vimentin against a background of neutrophils, lymphocytes and plasma cells (Figure 2). These cells were negative for cytokeratin and CD1a. A diagnosis of SHML was made. Patient was lost to follow-up as she returned back to her hometown.
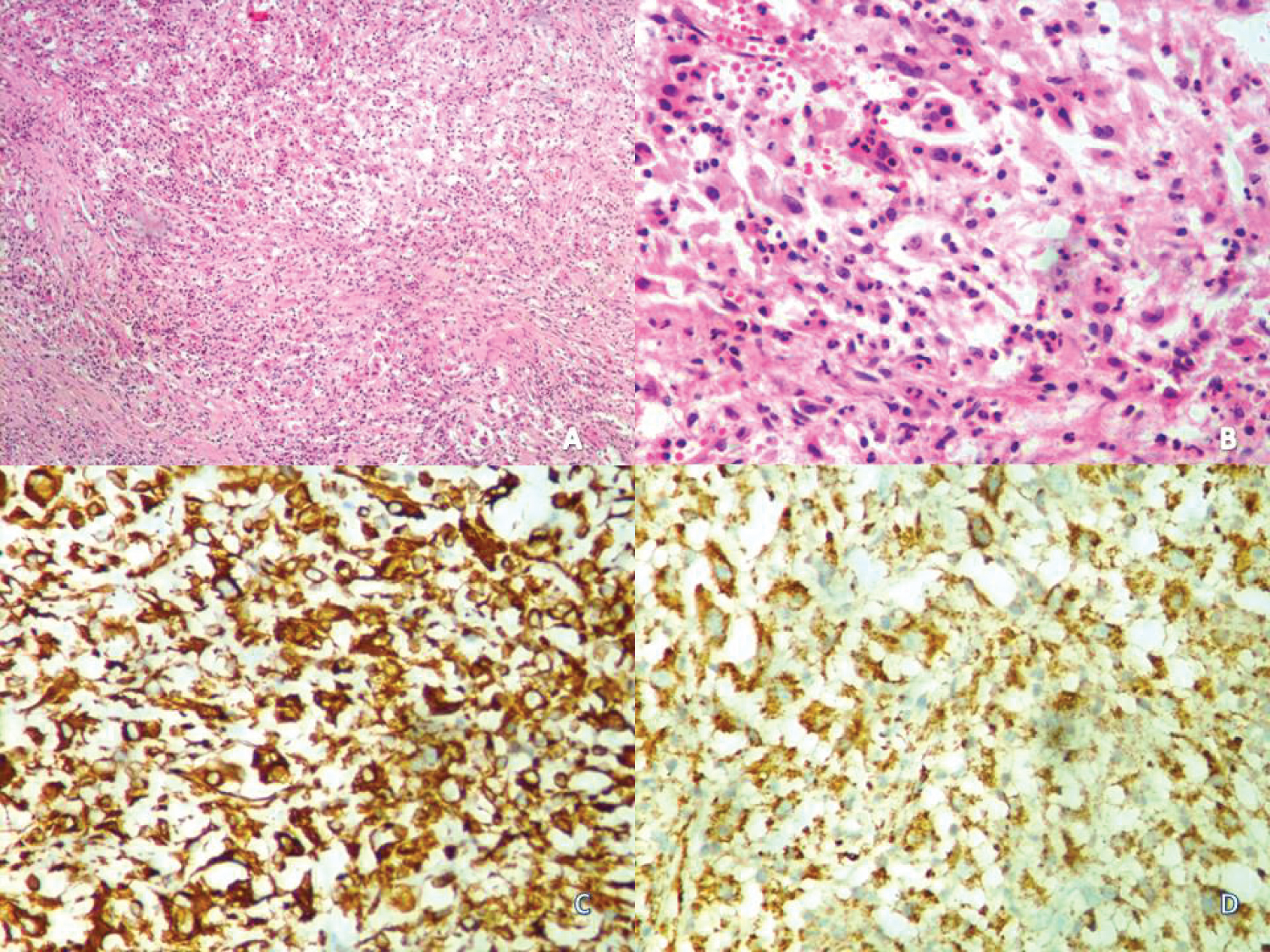 Figure 2: (A) Low power view (× 100) showing plump cells in a background of lymphocytes, plasma cells and emperipolesis; (B) High power view (× 4000) of large histiocyte like cells with emperipolesis; (C) S100 positivity; (D) CD68 positivity.
View Figure 2
Figure 2: (A) Low power view (× 100) showing plump cells in a background of lymphocytes, plasma cells and emperipolesis; (B) High power view (× 4000) of large histiocyte like cells with emperipolesis; (C) S100 positivity; (D) CD68 positivity.
View Figure 2
Sinus histiocytosis with massive lymphadenopathy (Rosai Dorfman disease) was first described by Rosai and Dorfman in the year 1969 [1]. It is caused by proliferation of histiocyte like cells in the sinuses of the lymph node and lymphatics of the extranodal tissue [2]. Liver involvement by SHML is rare but can present as a hypoechoic mass with obstructive symptoms mimicking a neoplasm. Liver can be involved denovo or along with lymph nodes, pancreas and gall bladder [3,4]. Another case of SHML of the liver and gall bladder presented with features suggestive of a cholecystitis but on opening the morphology was suggestive of a tumour; so a wedge biopsy was done which gave out the diagnosis [5]. An interesting case report from Africa depicts SHML presenting as a hepatosplenomegaly with lymphadenopathy in a known case of cirrhosis [6].
SHML can be either uni or multifocal, can occur in all ages but more prevalent in children and young adults with a male preponderance. Patients usually present with cervical lymphadenopathy, fever, night sweats, weight loss, malaise and arthralgia may also be present. Our patient presented with abdominal pain. The patients often have associated hypochromic microcytic anaemia, hypergammaglobulinaemia and a raised ESR. Most of the cases undergo spontaneous regression or show persistent localized disease. Few have died, usually with a more widespread disease. They often show evidence of immune deficiency.
Histologically, the lymph nodes show varying degrees of capsular fibrosis, expansion of the sinuses due to histiocytes with abundant, often vacuolated cytoplasm, and rounded nuclei with coarse chromatin and often a single prominent nucleolus. Some of these histiocytes have lymphocytes within their cytoplasm. Erythrocytes, plasma cells and polymorphs can also be seen. The intervening medullary cords show large numbers of plasma cells. Residual reactive germinal centres may be seen but these regress with time. In long-standing cases there is fibrous replacement of the involved nodes and surgery may be needed for cosmetic reasons or to relieve obstruction. The large cells express CD 68, S100 but are negative for CD1a. These are polyclonal [7]. Patients with immunologic defects and SHML involvement of the kidney, liver and lower respiratory tract are associated with a poor prognosis [8].
Extranodal SHML of the liver can arise denovo or along with involvement of the regional lymph nodes and adjacent organs. The presentation can also be vague with abdominal pain or fever. Imaging shows lytic lesions. So, the differentials include a metastatic tumour, lymphoma or infection. Careful investigation of clinical signs, symptoms, lab parameters and imaging along with a high index of suspicion helps in diagnosis.
Extranodal rosai dorfman disease of the liver is a great mimicker of metastases, lymphoma or infection, clinically and radiologically. So, a biopsy is warranted along with high index of clinical suspicion with correlation of imaging with tumour markers and other lab parameters to aid in the correct diagnosis.
There are no conflicts of interest.
Both authors have contributed to the article.
No funds were availed.