Cellular angiofibroma (CA) is an uncommon benign soft tissue tumor and typically arises in genitourinary region. There are only three reported cases at the head and neck region to the best of our knowledge; two different sites at eyelid and buccal mucosa. A 67-year-old man presented to the otorhinolaryngology unit with a painless nodule behind the left ear. Ultrasonography revealed a subcutaneous non-vascular, hyperechoic, homogenous, solid, 15×15 mm mass. The mass was excised and macroscopic examination revealed a well-circumscribed mass with variegated cut surface including firm tan and yellow areas. Microscopically, the tumor was composed of numerous small to medium sized hyalinized thick-walled vessels among spindle-shaped with monotonous bland nuclei and inconspicuous eosinophilic cytoplasm. Hemorrhage, necrosis, nuclear atypia, or mitotic activity were not observed. CD34 was positive and Ki67 proliferation index of 1%, while S100, chromogranin A, synaptophysin and desmin were negative. The final diagnosis was CA. Although, rare CA cases were presented at the head and neck region, this particular case is presented for its unique localization.
Angiofibroma, Cellular, Ear, Soft, Tissue
Cellular angiofibroma (CA) was first described by Nucci, et al. in 1997 as a benign mesenchymal lesion [1]. CA is seen evenly among men and women and usually has a predilection for vulvovaginal or inguinoscrotal regions [2]. Infrequently, extra genital involvement has been reported [3]. Histologically tumor is characterized by randomly distributed short bundles of bland spindle cells, tiny collagen fibers and hyalinized thick-walled vessels [1]. Case reports reveal similar lesions in other sites: subcutaneous tissue of the chest wall [3] and oral mucosa [4]. To the best of our knowledge only three cases have been reported in head and neck localization and no other case has been reported in the ear [4,5]. Herein, we present a new case with posterior auricular location which was unreported up to this time.
A 67-year-old man presented with painless mass behind the left ear that had developed over 2 years. There were no other symptoms. At palpation, the lesion was painless, firm, well circumscribed with a smooth surface. Ultrasonography revealed a subcutaneous non-vascular, hyperechoic, homogenous, solid, 15×15 mm mass. The mass was completely excised surgically.
Macroscopic examination revealed a well-circumscribed mass that measured 15×15×15 mm. The cut surface was variegated with firm tan and yellow areas. There was no hemorrhage or necrosis.
Microscopically, the tumor was composed of numerous hyalinized thick-walled vessels and spindle-shaped cells (Figure 1). The vessels were small to medium sized and were scattered in an edematous stroma (Figure 2). The spindle-shaped cells exhibited monotonous bland nuclei with inconspicuous eosinophilic cytoplasm (Figure 3). Hemorrhage, necrosis, nuclear atypia, or mitotic activity were not observed. Immunohistochemical analysis revealed positivity for CD34 (Figure 4). S100, chromogranin A, synaptophysin and desmin were negative. Ki67 proliferation index was 1% (Figure 5).
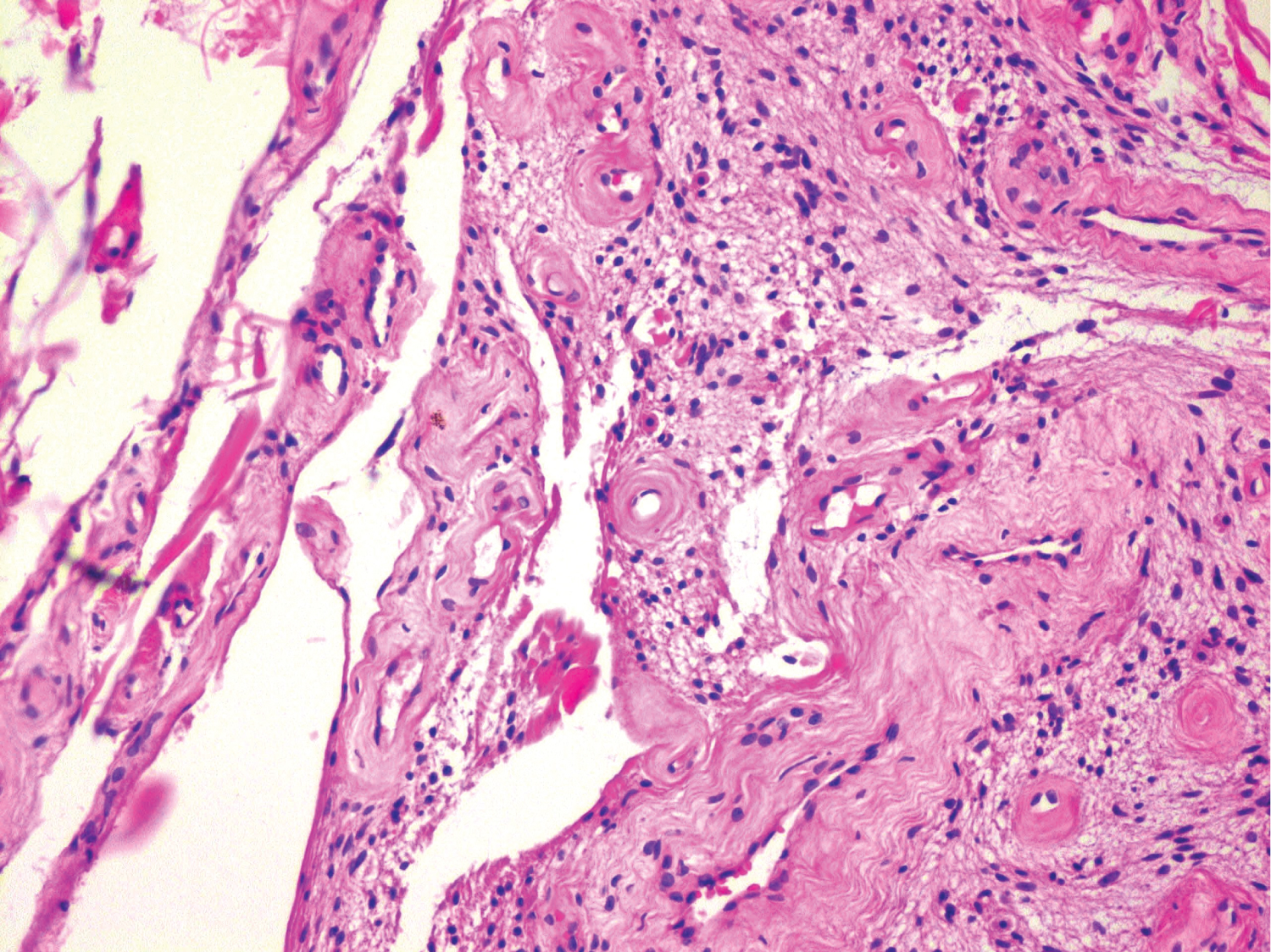 Figure 1: Spindle-shaped cells between hyalinized thick-walled vessels (H-E, original magnification x200).
View Figure 1
Figure 1: Spindle-shaped cells between hyalinized thick-walled vessels (H-E, original magnification x200).
View Figure 1
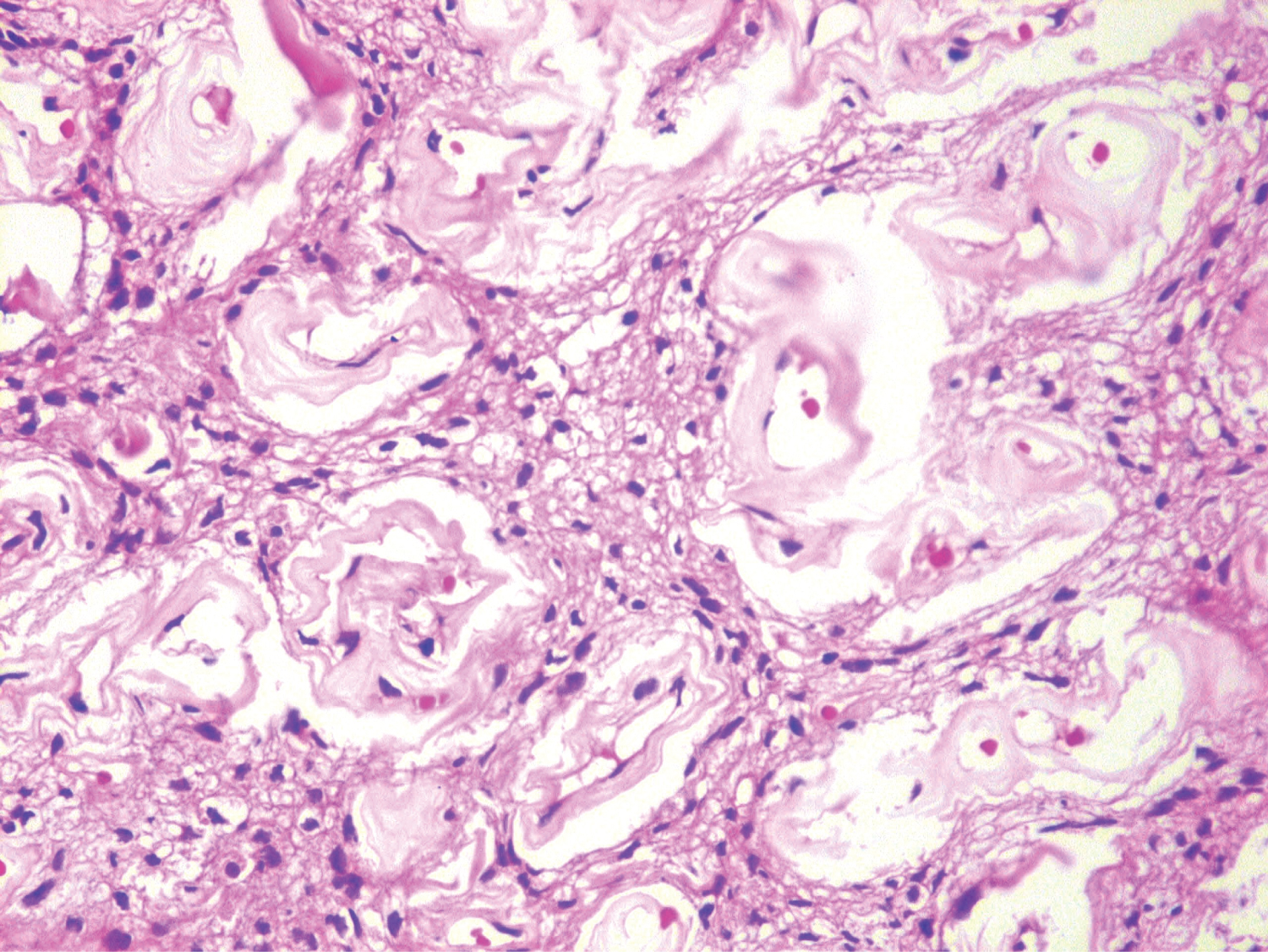 Figure 2: Various sized vessels were dispersed in a loose edematous stroma (H-E, original magnification x200).
View Figure 2
Figure 2: Various sized vessels were dispersed in a loose edematous stroma (H-E, original magnification x200).
View Figure 2
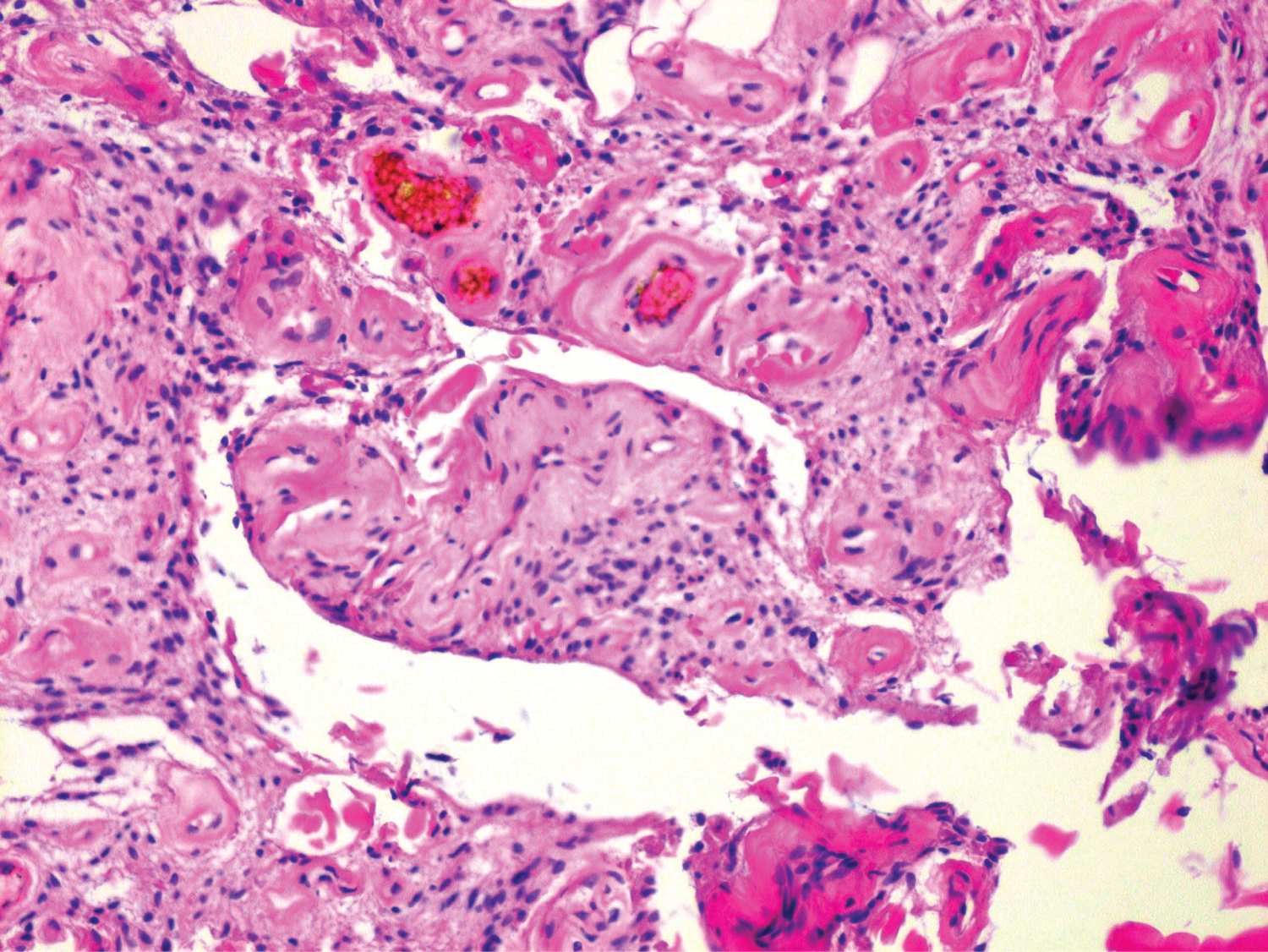 Figure 3: The spindle-shaped cells with monotonous bland nuclei and inconspicuous eosinophilic cytoplasm (H-E, original magnification x400)
View Figure 3
Figure 3: The spindle-shaped cells with monotonous bland nuclei and inconspicuous eosinophilic cytoplasm (H-E, original magnification x400)
View Figure 3
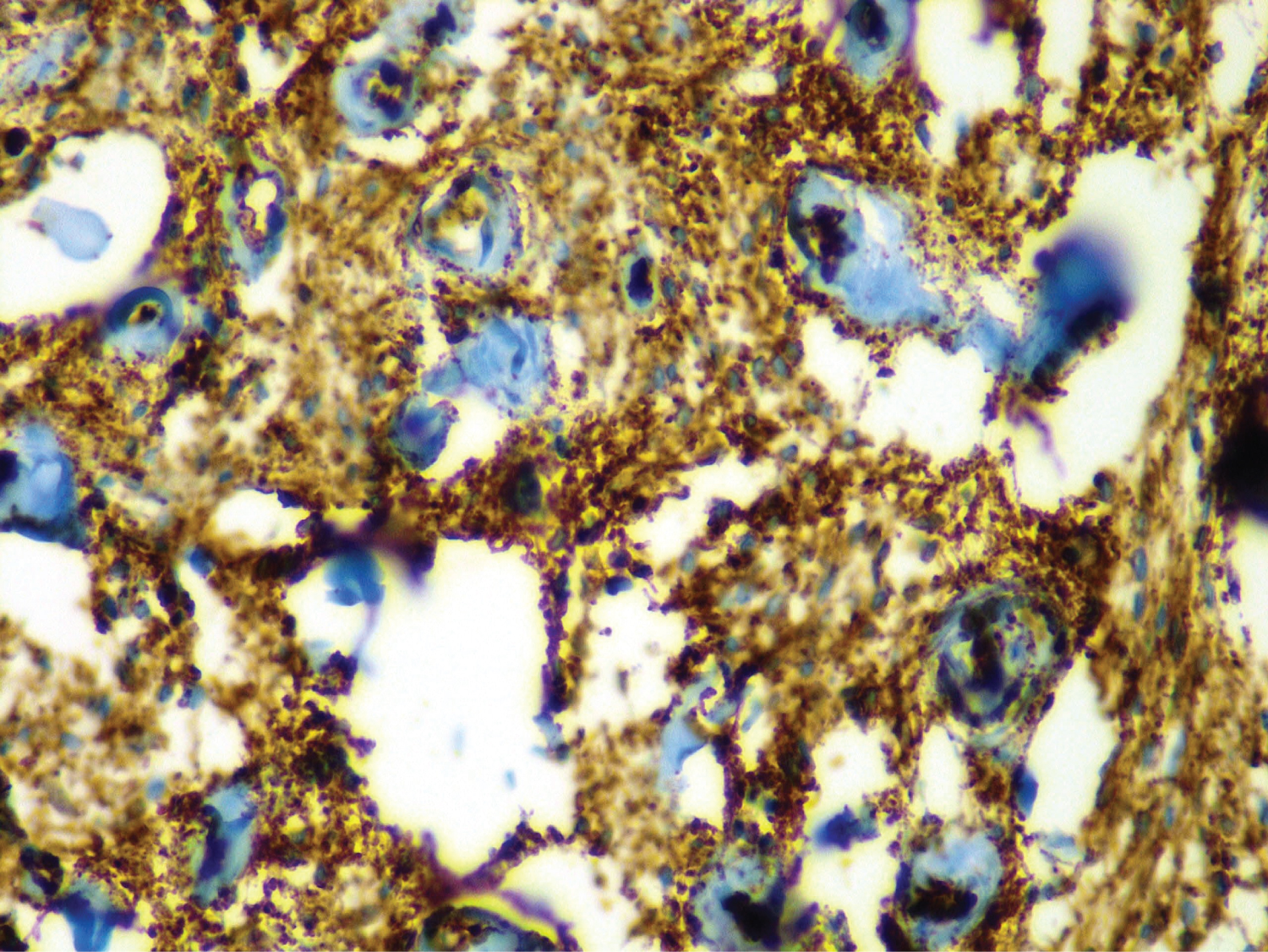 Figure 4: Positive CD34 expression of spindle cells (original magnification x400)
View Figure 4
Figure 4: Positive CD34 expression of spindle cells (original magnification x400)
View Figure 4
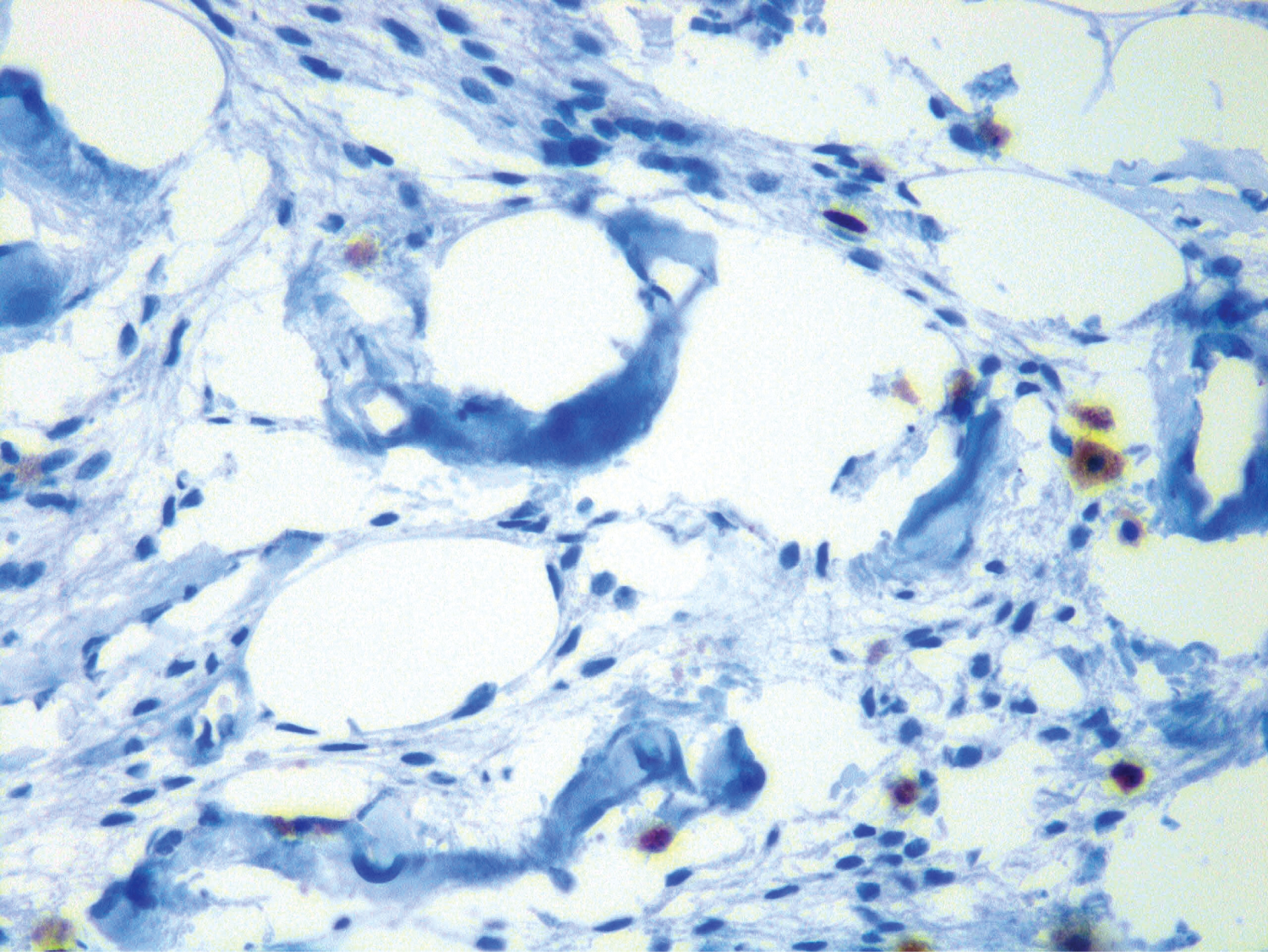 Figure 5: Immunohistochemistry with Ki67 stain showing low proliferation index (original magnification x400).
View Figure 5
Figure 5: Immunohistochemistry with Ki67 stain showing low proliferation index (original magnification x400).
View Figure 5
The histopathologic diagnosis was typical CA.
CA is a rare benign mesenchymal tumor [1]. These tumors most frequently occur in the vulvovaginal and inguinoscrotal regions [6]. Laskin, et al. [7] defined the tumor as "angiomyofibroblastoma-like tumor", in a series of cases comparing the female and male cases. World Health Organization classification of soft tissue tumors has approved the term cellular angiofibroma for these morphologically identic lesions which may be seen in both sexes with similar frequency [8]. The mean age at presentation is 53.5 years. In women they tend to occur earlier, most often in the fifth decade, while men are mostly affected in the seventh decade [6]. Our patient was also a male patient at the 7th decade. Patients usually have painless mass as in our case. The tumors appeared predominantly at the vulvovaginal region for the female and the inguinal as well as scrotal/paratesticular regions for the male patients [3,6,9]. Cases occurring in extragenital locations such as eyelid, oral mucosa, elbow, chest wall, retroperitoneum, knee have also been described, however posterior auricular location was not described previously to the best of our knowledge [3,4,6,10,11]. Average tumor size is 9 (range 3.5-25) cm [3]; much bigger than our case. Lesions were usually located in superficial compartments of soft tissue, similar to our case. Infrequently, involvement of retroperitoneum, pelvis, prostate and urethra have been reported [6,9].
The macroscopic features of our case were typical for CA other than the smaller size. Grossly, the neoplasm is well circumscribed, however focal extension into adjacent soft tissue may be seen [12]. Usually tumor isfirm and has a white/tan color cut surface [6]. Exceptional cases show hemorrhage and foci of necrosis [6].
Histologically, tumor is composed of bland spindled cells, tiny collagen bundles and numerous small to medium sized often hyalinized thick-walled vessels. Some cases obtain mature adipocytes also lobule of fat formation [6, 12].
The spindle cell component is prominent and haphazardly scattered throughout the lesion [6]. The spindle cells usually have short, fusiform, ovoid nuclei with inconspicuous nucleoli, pale eosinophilic cytoplasm with indistinct borders. Nuclear groove and intranuclear inclusions are usually seen [11]. Limited inflammatory cells, such as lymphocytes and rarely neutrophils, are distributed throughout the stroma [7]. Also mast cells are commonly seen. Mitotic activity is variable, abnormal mitotic activity and cytologic atypia are rarely observed [6]. Also, mast cells are commonly seen. Mitotic activity is variable, abnormal mitotic activity and cytologic atypia are rarely observed [2].
Chen, et al. reported that atypia or sarcomatous transformation can be seen in CA [2]. Our case lacked significant atypia, Ki67 proliferative index was low and the abundance of thick-walled vascular structures was striking, with typical spindle-shaped cells.
Immunohistochemically, the tumor cells express vimentin, CD34 (50-60%) and actin (21%), but they do not express desmin, S100 protein, keratin and epithelial membrane antigen [6,11,12].
Differential diagnosis of cellular angiofibroma depends on localization of the tumor. The morphology and clinical features of CA is different from typical angiofibroma which are located at the nasopharynx of the young male patients, and should not be included at the differential diagnosis of such cases. For our case, like other extragenital CA cases, the differential diagnosis included angiofibroma of soft tissue, spindle cell/pleomorphic lipoma,solitary fibrous tumor, smooth muscle tumors, benign nerve sheath tumors, and superficial angiomyxoma [3].
Angiofibroma of soft tissue is a benign fibrovascular tumor. This tumor commonly arises as a soft tissue mass of the extremities. Microscopically, the tumor has spindle-shaped cells in a myxoid or collagenous stroma and in contrast to CA, has a characteristic branching thin-walled blood vessels. Angiofibroma of soft tissue expresses CD34 and SMA with lower frequency (14%) than CA [13]. Anatomic localization of tumor and the component of prominent hyalinized thick-walled vessels provided to rule out this diagnosis from our differential diagnosis checklist.
Spindle cell/pleomorphic lipomas are mostly seen in head and neck localization. They are composed of bland spindled cells, mast cells, multinuclear giant cells, have minimal/no adipocytes, ropey collagen and sparse thin-walled vessels. The latter two are helpful findings distinguishing CA from spindle cell lipoma which has thick-walled vessels and wispy collagen fibrils are not thick in contrast to the ropey collagen typical for the spindle cell lipoma [12]. Solitary fibrous tumors (SFT) may arise in any anatomical part of body and are characterized by CD34-positive spindled cells arranged in a paternlesspatern, variably hypo-hypercellular areas, stromal hyalinization, hemangiopericytoma-like vascular pattern which differs from the more rounded, thick-walled vessels seen in cellular angiofibroma [14]. Smooth muscle tumors can be distinguished from CA by the typical morphology of spindle cells with cigar-shaped nuclei and abundant eosinophilic fibrillary cytoplasm [15]. CA shows generally desmin and caldesmon negativity unlike smooth muscle tumors [12]. Benign nerve sheath tumors, such schwannoma and neurofibroma, have spindle cells with wavy nuclei and S100 positivity. CA can be distinguished from nerve sheath tumors by S100 protein negativity [11,15]. Superficial angiomyxoma composed of spindle-stellate shaped cells and small thin-walled vascular channels within a myxoid stroma. Stromal neutrophils are diagnostic clue [12].
Our case had typical morphological features of CA. CD34 positive, desmin and S100 negative immunohistochemical profile was helpful in the differential diagnosis.
Iwasa and Fletcher's study [6] showed that CA has a benign course without any risk for recurrence or metastasis. In a series of 14 patients, Flucke, et al. [11] reported neither local recurrence nor metastasis. No cases with local recurrence or metastasis was reported in Nucci and Fletcher's experience [12]. This typical case of CA, located in this previously unreported location highlights the possibility of these lesions at the head and neck region, which should be kept in mind in differential diagnosis.
The authors have no conflicts of interest to declare.
The authors declared that this study has received no financial support.