Adenomatoid tumors are benign tumors of mesothelial origin seen in female genitourinary tract, most commonly involving the uterus and rarely fallopian tubes. We herein report a case of 46-year-old female who presented with abnormal vaginal bleeding with complex cyst in left adnexa and multiple leiomyomata upon pelvic imaging. Hysterectomy and bilateral salpingectomy were done. A circumscribed red-tan nodule, measuring 3.0 cm in maximum dimensions was identified on the left fallopian tube with a solid, homogenous yellow-tan cut surface. The histopathological examination revealed features of adenomatoid tumor supported by immunohistochemical stains positive for calretinin and cytokeratin and negative for CD34. This is a benign entity but need to be differentiated from malignant lesions owing to variable histopathological patterns and cytological features. These have good prognosis upon surgical removal with no evidence of recurrence. This case is being presented due to the rarity of adenomatoid tumors in this location along with the discussion of other potential differential diagnosis in this location.
Fallopian tube, Adenomatoid tumor
The Fallopian tube tumors are rare entities accounting for approximately 1-2% of female genital malignancies. According to WHO classification, Fallopian tube tumors are classified as malignant and benign [1]. The adenomatoid tumors are benign mesotheliomas of a female genitourinary tract involving the serosal, sub serosal and intramural aspects of the uterus, the round ligaments, and the fallopian tubes [2]. The common site for adenomatoid tumor in female genitourinary tract include uterine corpus though only few cases involving fallopian tubes have also been reported. These are incidentally seen in the females of reproductive age especially between ages of 26 and 55 years [3,4]. The other common sites of adenomatoid tumor include testis, tunica vaginalis of testis, epididymis, adrenal gland [5,6] small intestine [7] and mediastinum [8]. We hereby present a case of a 46-year-old female with abnormal vaginal bleeding and an incidental finding of adenomatoid tumor in fallopian tube.
A 46-year-old female presented with abnormal vaginal bleeding, polymenorrhea, and menorrhagia. Physical examination revealed pallor. Labs revealed anemia with hemoglobin of 7.8 g/dl. All other labs were unremarkable. The trans-abdominal and trans-vaginal ultrasound of abdomen and pelvis showed enlarged uterus measuring 12.7 × 8.2 × 6.2 cm with an endometrial stripe of 1.2 cm and multiple hypo-echoic lesions in the myometrium with largest measuring 3.0 × 2.8 × 1.7 cm in the posterior aspect of uterus. An anechoic cyst was identified in the left adnexa measuring 3.1 × 2.8 × 2.7 cm. The computerized tomographic scan of abdomen and pelvis showed a low attenuation structure in the left adnexa, possible mildly complex para-ovarian cyst. Based on the imaging, a clinical suspicion of benign adnexal cyst was made. Hysterectomy and bilateral salpingectomy was performed. The ovaries were left intact bilaterally.
The specimen was received for an intra-operative consultation. Grossly, the specimen was received in multiple fragments and showed an enlarged and mildly distorted fallopian tube with nodular red-tan external surface measuring 3.0 × 2.5 × 2.5 cm. It has a solid, yellow-tan and homogenous cut surface. No areas of cystic or necrotic change were identified. The lesion composed predominantly of spindle shaped cells and was diagnosed as atypical spindle cell lesion on frozen section. The histopathological examination of permanent microscopic sections from left fallopian tube showed an un-encapsulated and well circumscribed lesion composed of glands, tubules, and cystic spaces lined by cuboidal to flat epithelial cells surrounded by loose edematous to cellular fibroblastic stroma. The cells have round to oval bland nuclei in moderate eosinophilic cytoplasm. The epithelial cells display vacuolization and signet ring cell appearance. Spindle smooth muscle cells were identified in the stroma. No atypia, mitosis or necrosis was identified (Figure 1).
 Figure 1: Adenomatoid tumor of fallopian tube. A) The cystic spaces (arrows) lined by cuboidal to flat epithelial cells; B) Areas of smooth muscle hyperplasia (arrows). View Figure 1
Figure 1: Adenomatoid tumor of fallopian tube. A) The cystic spaces (arrows) lined by cuboidal to flat epithelial cells; B) Areas of smooth muscle hyperplasia (arrows). View Figure 1
The immunohistochemical stains for Calretinin, Cytokeratin and CD34 were done. The lesional cells were strongly and diffusely positive for Calretinin and Cytokeratin, and negative for CD34 (Figure 2). The immunohistochemical stains supported the histopathological diagnosis of adenomatoid tumor.
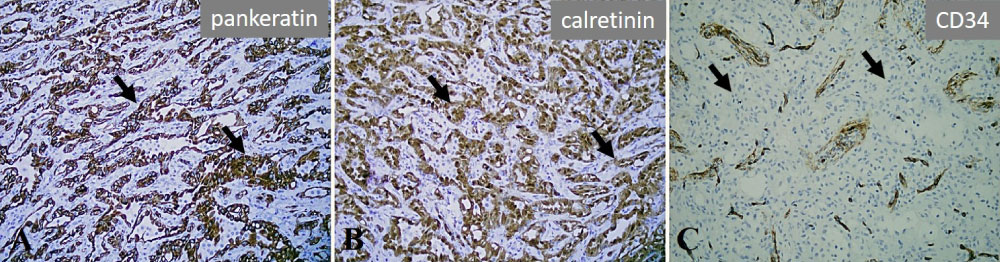 Figure 2: Immunohistochemical stains confirming the diagnosis. A, B and C, Tumor cells are positive for pan Cytokeratin (arrows) and Calretinin (arrows) while negative for CD34 (arrows). View Figure 2
Figure 2: Immunohistochemical stains confirming the diagnosis. A, B and C, Tumor cells are positive for pan Cytokeratin (arrows) and Calretinin (arrows) while negative for CD34 (arrows). View Figure 2
The hysterectomy specimen with right fallopian tube was received separately that showed secretory type endometrium with multiple leiomyomata and adenomyosis. The right fallopian tube showed no significant microscopic abnormalities.
Adenomatoid tumors are benign tumors of mesothelial origin most commonly seen in uterus with an incidence of 1.2%. Though found extremely rare in fallopian tube, these are the most common benign tumors involving the fallopian tubes. Our patient is a 46-year-old female who presented with abnormal vaginal bleeding with multiple leiomyomata upon imaging and an incidentally found an-echoic nodule in the left adnexa, diagnosed as adenomatoid tumor upon histopathological examination.
Adenomatoid tumors were first described and termed in 1945 by Golden and Ash [9], who considered this tumor to be of epithelial origin. Regan and Crane concurred with their theory and named them as ‘Adenoma/Tubular Adenoma'. The arrangement of tumor cells in glands and the presence of intracytoplasmic vacuoles favored epithelial differentiation of these cells [10].
There have been various other hypothesis been postulated related to the histogenesis of these tumors including endothelial, mesonephric, mullerian and mesothelial origin [11]. Masson and Evans described that adenomatoid tumors represent a unique variant of benign mesotheliomas restricted to the genital tract [12]. The mesothelial origin has been supported by the histomorphological, ultrastructural and immunohistochemical findings.
The adenomatoid tumors arising in both male and female genital tract are recently been found to be associated with somatic missense mutations in TRAF7 gene mutation encoding E3 ubiquitin ligase leading to phosphorylation of NF-kB and increased expression of L1 cell adhesion molecule. L1CAM, L1 cell adhesion molecule shows immunohistochemical expression in adenomatoid tumors but absent in normal mesothelial cells, malignant peritoneal mesotheliomas and peritoneal inclusion cysts [13].
Macroscopically, these tumors present as a nodule on the external surface of fallopian tube ranging in size from 0.5 to 3.0 cm in size. In the present case, a solid nodule was present in the right fallopian tube measuring 3.0 cm in diameter with solid gray-tan cut surface. Four histopathological patterns have been described upon microscopic examination: Adenoid, angiomatoid, solid, and cystic [8]. In the present case, the tumor cells were predominantly arranged in densely packed small glands and tubules, with focal areas of cyst formation. The cells have intracytoplasmic vacuoles. Signet ring type cells were also present. The lesional cells were not seen to be in continuity with the serosa or the tubal epithelium. The immunohistochemical stains reveal diffuse, strong membranous and cytoplasmic positivity with cytokeratin, positive nuclear and cytoplasmic staining with calretenin and D2-40. The cells are negative for CK 5/6, CK20, EMA, CD31 and CD34 [14].
The ultrastructural features support the mesothelial origin of cells including the presence of microvilli, desmosomes, tonofilaments and tonofilament-like structures and dilated intercellular spaces [15].
The histopathological examination of these tumors may reveal ill-defined and infiltrative margins leading to a mistaken diagnosis of carcinoma, including adenocarcinomas and mesotheliomas but circumscribed gross appearance, bland cytological features and absence of mitotic activity aid in their distinction [16]. These tumors may resemble benign vascular neoplasms like hemangioma and lymphangioma. The positive immunohistochemical staining for epithelial markers and negative staining for CD34 is helpful to differentiate them in difficult cases [17].
These tumors may undergo infarction with large central areas of necrosis and proliferation of reactive fibroblast cells in periphery which may mimic malignancy [18].
Lipo-leiomyoma may also be considered as one of the differentials of adenomatoid tumor. It is a benign tumor that consists of a leiomyoma in combination with adipocytes. It is positive for S-100 and negative for epithelial and mesothelial markers [19].
Well differentiated liposarcoma can also resemble adenomatoid tumor. It consists of mature adipocytes and stromal cells with focal cytologic atypia. Immunohistochemistry can help distinguish it from adenomatoid tumor. Liposarcoma is positive for S-100, MDM2 and CDK4 while it's negative for epithelial and mesothelial markers [20].
Salpingitis isthmic nodosa (SIN) is an acquired lesion in which the tubal epithelium penetrates the muscular layer of the fallopian tube. The glands may undergo a metaplastic change from tubal to endometrial type. The muscular layer shows hypertrophic and hyperplastic change in response. It may resemble adenomatoid tumor on histopathology. Salpingitis isthmic nodosa stains negative for D2-40 and WT1 as opposed to adenomatoid tumor which is positive for these mesothelial markers [21].
Despite being the most common tumors of fallopian tube, adenomatoid tumors are quite rarely encountered in surgical practice and are an incidental gross and microscopic diagnosis. Due to the occasional presence of variable histological patterns including poorly defined, infiltrative margins and occasional bizarre cells, these may mimic other benign and malignant lesions and need to be distinguished from them. Nevertheless, these are benign tumors with excellent prognosis upon resection with no casses of recurrence known so far in literature.