Prostatic cancer ranks the second of case fatality rate in males all over the world, second only to lung cancer [1-4]. There are over 540000 new cases diagnosed each year worldwide [5]. The classic, widely used prognostic factors for prostatic cancer are S.PSA (prostate specific antigen) serum levels, Gleason's score and staging represented by TNM system. S.PSA is widely used for prostate cancer screening and has resulted in an overall decrease in prostate cancer metastasis and death.
However, this screening has also led to over-detection and over-treatment, as elevation in S.PSA levels can also be present as a result of infection, chronic inflammation or benign prostatic hyperplasia [1]. Thus, searching for new methods of therapy and prognosis becomes a key task. Diagnosis of prostate adenocarcinoma based on histopathological features alone can be challenging in some situations and immunohistochemistry can aid in the diagnosis.
The present study has been undertaken to compare the immunoexpression of Survivin and Ki67 in biopsy proven tissues of prostate cancer and benign prostatic hyperplasia as well as to determine whether this immunoexpression could correlate with Gleason's score, S.PSA levels.
Objectives:
• To estimate the frequency of expression of Survivin and Ki67 in biopsy proven tissues of prostate cancer and benign prostatic hyperplasia.
• To determine the correlation of Gleason's score and pre-operative S.PSA levels with the frequency of expression of Survivin and Ki67 in the prostate cancer tissue and benign prostatic hyperplasia.
Methodology: This cross-sectional study involves 15 prostatic cases and 15 benign prostatic hyperplasia cases as control. Cases were selected by consecutive sampling from February 2021 to August 2022. Clinical history and clinicopathological parameters were obtained, histomorphological and immunohistochemical evaluation was done and the results were correlated with clinicopathological variables. The IHC panel we used included rabbit monoclonal Survivin antibody and mouse monoclonal ki67 antibody.
Results: In our study, out of the 15 cases of adenocarcinoma prostate, 53.3% show positivity and 46.7% show strong positivity for Survivin. Out of 15 benign prostatic hyperplasia, 66.7% of cases showed weak positivity for Survivin. There was a statistically significant difference in the Survivin score between prostatic cancer patients and benign prostatic hyperplasia cases. Frequency of expression of Survivin in benign prostatic hyperplasia showed a high statistically significant correlation with S.PSA value. None of the benign prostatic hyperplasia cases showed strong positivity for Survivin. Frequency of expression of Survivin in benign prostatic hyperplasia showed a high statistically significant correlation with S.PSA value. All adenocarcinoma cases and 86.7% of benign prostatic hyperplasia showed Ki67 positivity. Higher grades of ki67 expression (3+, 2+, and 1+) are seen in adenocarcinoma cases. The Ki67 expression was more in adenocarcinoma cases more than in benign prostatic hyperplasia. The S.PSA levels were more elevated in adenocarcinoma patients than in benign prostatic hyperplasia. The frequency of expression of Ki67 in prostatic cancer and S.PSA showed a statistically significant correlation. The study did not show any statistically significant correlation between the expression of Survivin in adenocarcinoma prostate and Gleason's score. Thus, Survivin cannot be used as an indicator of the aggressiveness of the tumour. The study didn't show any statistically significant correlation between Ki67 and S.PSA levels in benign prostatic hyperplasia. The study did not show any statistically significant correlation between Ki67 expression and Gleason's score in prostatic adenocarcinoma. There was a highly significant positive correlation between the combined tests (Survivin + Ki67) and the presence of adenocarcinoma prostate.
Conclusion: The study showed that the expression of Survivin and Ki67 is significantly higher in adenocarcinoma prostate than in benign prostatic hyperplasia. While 46.7% of adenocarcinoma prostate showed strong Survivin positivity; none of the benign prostatic hyperplasia cases showed strong positivity for Survivin. Thus, the marker may be used to differentiate between adenocarcinoma prostate and benign prostatic hyperplasia.
Higher grades of Ki67 expression were seen in adenocarcinoma prostate cases than in benign prostatic hyperplasia. There is a statistically significant correlation between Ki67 expression in prostate cancer and S.PSA levels. S.PSA levels were elevated more in adenocarcinoma prostate than in benign prostatic hyperplasia. There was a significantly positive correlation between the combined tests (Survivin + Ki67) and the presence of adenocarcinoma prostate.
The study also proved that even though Survivin expression is higher in adenocarcinoma prostate its expression cannot be used as an indicator of the aggressiveness of the tumour.
Survivin, Ki67, Gleason’s score
AAH: Atypical Adenomatous Hyperplasia; AMACR: Alpha-Methyl Acyl Coenzyme A Racemase; AsAP: Atypical small Acinar Proliferation; BCG: Bacillus Calmette Gurein; BPH: Benign Prostatic Hypotrophy; CXCL8: C-X-C Motif Chemokine Ligand 8; E2F3: E2 F Transcription Factor 3; ELISA: Enzyme-Linked Immunosorbent Assay; HMWCK: High Molecular Weight Cytokeratin; HuPEC: Human Normal Prostate Epithelial Cell Line; IHC: Immunohistochemistry; ING 4: Inhibitor of Growth 4; ISUP: International Society of Urological Pathology; PAH: Post Atrophic Hypoplasia; PAP: Prostrate Acid Phosphatase; PAS: Periodic Acid Schiff; PCNA: Proliferating Cell Nuclear Hg; PIN: Prostate Intraepithelial Neoplasm; S.PSA: Serum Prostate Specific Antigen; S.PSAP: Serum Prostate Specific Acid Phosphatase; SRSF1: Serine/Arginine Rich Splicing Factor 1; TNM; Tumour Nodes and Metastasis; TRUS: Transrectal Ultrasound Scan; TURP: Transurethral Resection of the Prostrate; VEGF: Vascular Endothelial Growth Factor; VMGH: Verumontanum Mucosal Gland Hyperplasia; WHO: World Health Organization
• To estimate the frequency of expression of Survivin and Ki67 in biopsy proven tissues of prostatic carcinoma and BPH.
• To determine the correlation of Gleason’s score and pre-operative serum S.PSA levels with the frequency of expression of Survivin and Ki67 in the Prostate cancer tissue and benign prostatic hyperplasia.
Cross-sectional study.
Department of Pathology, Pushpagiri Institute of Medical Sciences and Research Centre, Thiruvalla.
Considering the proportion of expression of Survivin in prostate cancer (p1) and benign prostatic hyperplasia (p2) from the previous study [1,5] with CI as 95% and power of the study 1-β as 80% the sample size obtained is 13 per group using the formula:
n = [Z (1-α/2) √(2pq)+ Z (1-β) √(p 1 q 1 + p 2 q 2 )] 2 /(p 1 – p 2 ) 2
where, q = 1-p; q 1 = 1-p 1 ; q 2 = 1-p 2
All specimens diagnosed as prostate carcinoma and benign prostatic hyperplasia on histopathology.
All specimens diagnosed as prostate carcinoma and benign prostatic hyperplasia on histopathology received in the Department of Pathology, Pushpagiri Institute of Medical Sciences and Research Centre during the study period.
1. Patients who took therapy prior to the
2. Metastatic tumours to
3. Malignant tumours other than
Consecutive sampling till the desired sample size is obtained.
All specimens received in the Department of Pathology, Pushpagiri Institute of Medical sciences and Research Centre and diagnosed as prostate carcinoma and benign prostatic hyperplasia on histopathology during the study period as per inclusion and exclusion criteria.
18 months from the date of ethical clearance.
Formalin fixed paraffin embedded tissue blocks of prostate cancer cases along with benign prostatic hyperplasia tissues as control was included in the study.
After getting approval from the Institutional Ethics and Research Committee data was collected in a proforma. Patient details were recorded referring the registers and request forms.
Formalin fixed paraffin embedded tissue blocks of adenocarcinoma prostate and benign prostatic hyperplasia was taken. Sections of 4-micron thickness was taken and mounted on the slides. The paraffin embedded tissue sections were stained with Rabbit anti-human Survivin polyclonal antibody.
Cells which show yellow-brown color in cytoplasm or cell nucleus was considered as positive for Survivin.
The expression will be graded according to following staining intensity score.
0 - no expression, if colorless
1+ - weak, if light yellow
2+ - moderate, if clay bank
3+ - strong, if brown
Percentage of positive stained tumour cells:
0: if < 10%
1: if between 10-50%
2: if between 51-75%
3: if more than 75%
Five visual fields in each slide were selected and the proportion of positive cells in 100 cells under microscope was taken as the percentage of positive cells. The product of integral staining intensity and positive cells proportion was used for evaluating the positive degree.
0-1 - Negative
2-4 - weak positive
5-8 - positive
9-12 - strong positive
For Ki67, the tumours are divided in to five groups regarding the percentage of Ki67 positive cells. Cases in which the percentage of stained cells is ≤ 2% was considered negative.
Cases with Ki67 index of:
≤ 25% will be considered 1+
26-50% - 2+
51-75% - 3+
76-100% - 4+
The study will provide frequency of Survivin expression in prostate carcinoma and benign prostatic hyperplasia. This will be correlated with the histopathology score (Gleason’s score) and pre-operative S.PSA levels.
The study will provide frequency of Ki67 positivity in prostate carcinoma and benign prostatic hyperplasia and its correlation to aggressiveness of the tumour.
Data was analyzed and presented as frequency and percentage for categorical data and mean and SD for continuous data. Frequency of expressions of Survivin and Ki67 in prostate cancer and benign prostatic hyperplasia tissue was compared using Chi-square test. Association between Survivin expression and Gleason’s score and pre-operative serum S.PSA levels as well as between Ki67 and aggressiveness was tested for statistical significance using Chi-square test. A p value of less than 0.05 will be considered statistically significant.
Table 1 and Figure 1; Table 2 and Figure 2; Table 3 and Figure 3; Table 4 and Figure 4; Table 5; Table 6 and Figure 5; Table 7 and Figure 6; Table 8; Table 9; Table 10; Table 11; Table 12; Table 13; Table 14
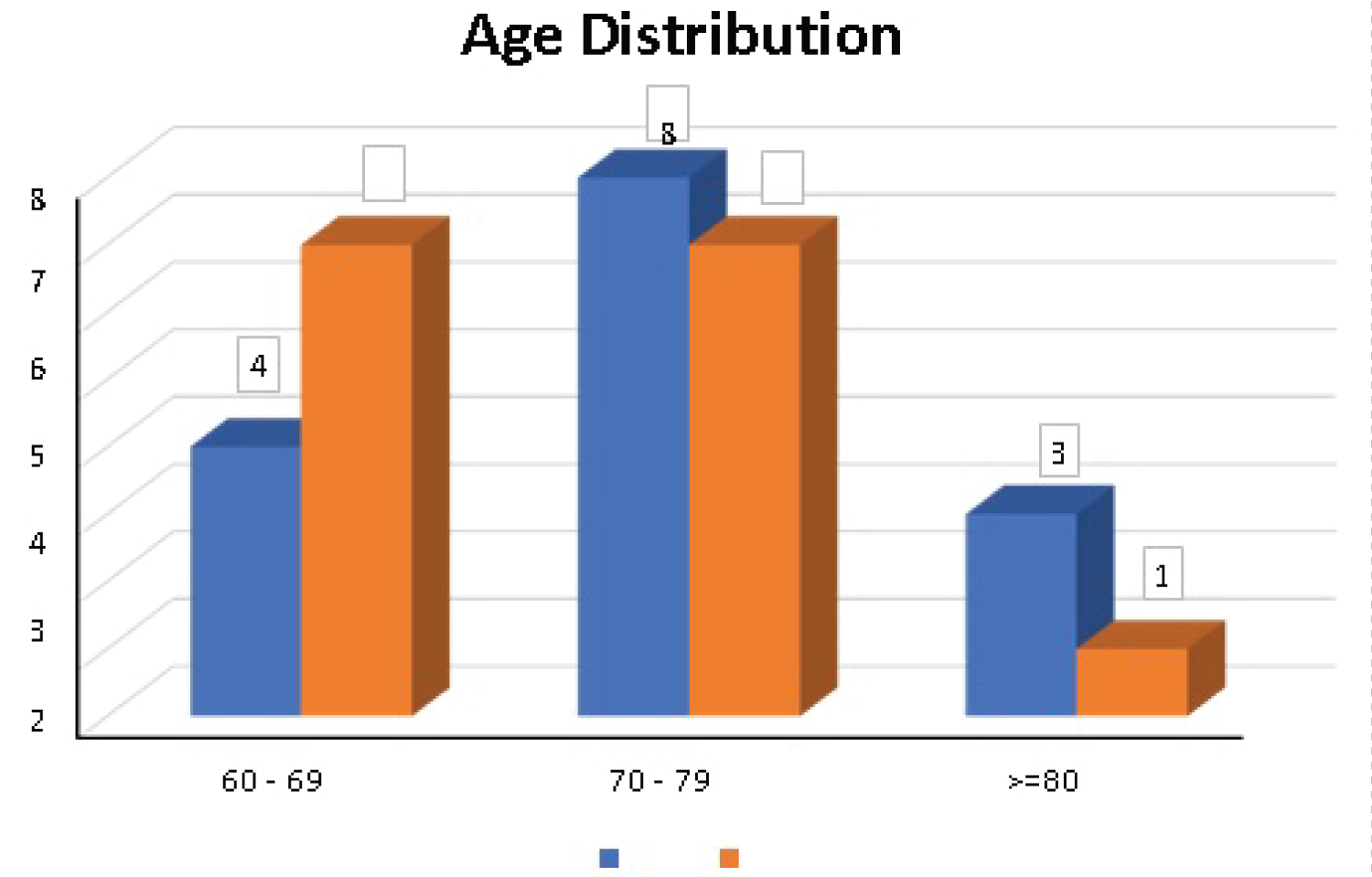 Figure 1: Distribution of age groups.
View Figure 1
Figure 1: Distribution of age groups.
View Figure 1
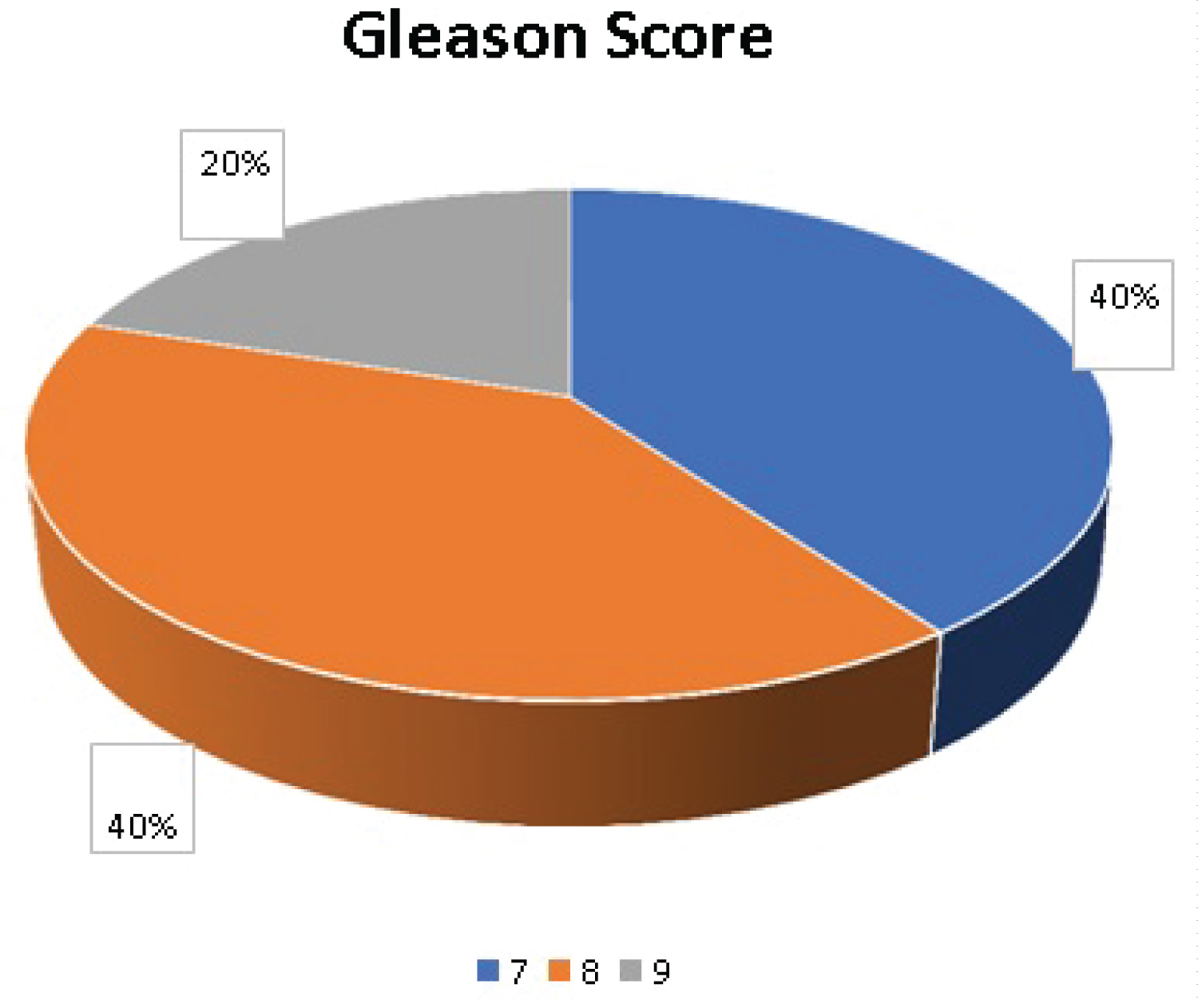 Figure 2: Distribution of cases according to Gleason's score.
View Figure 2
Figure 2: Distribution of cases according to Gleason's score.
View Figure 2
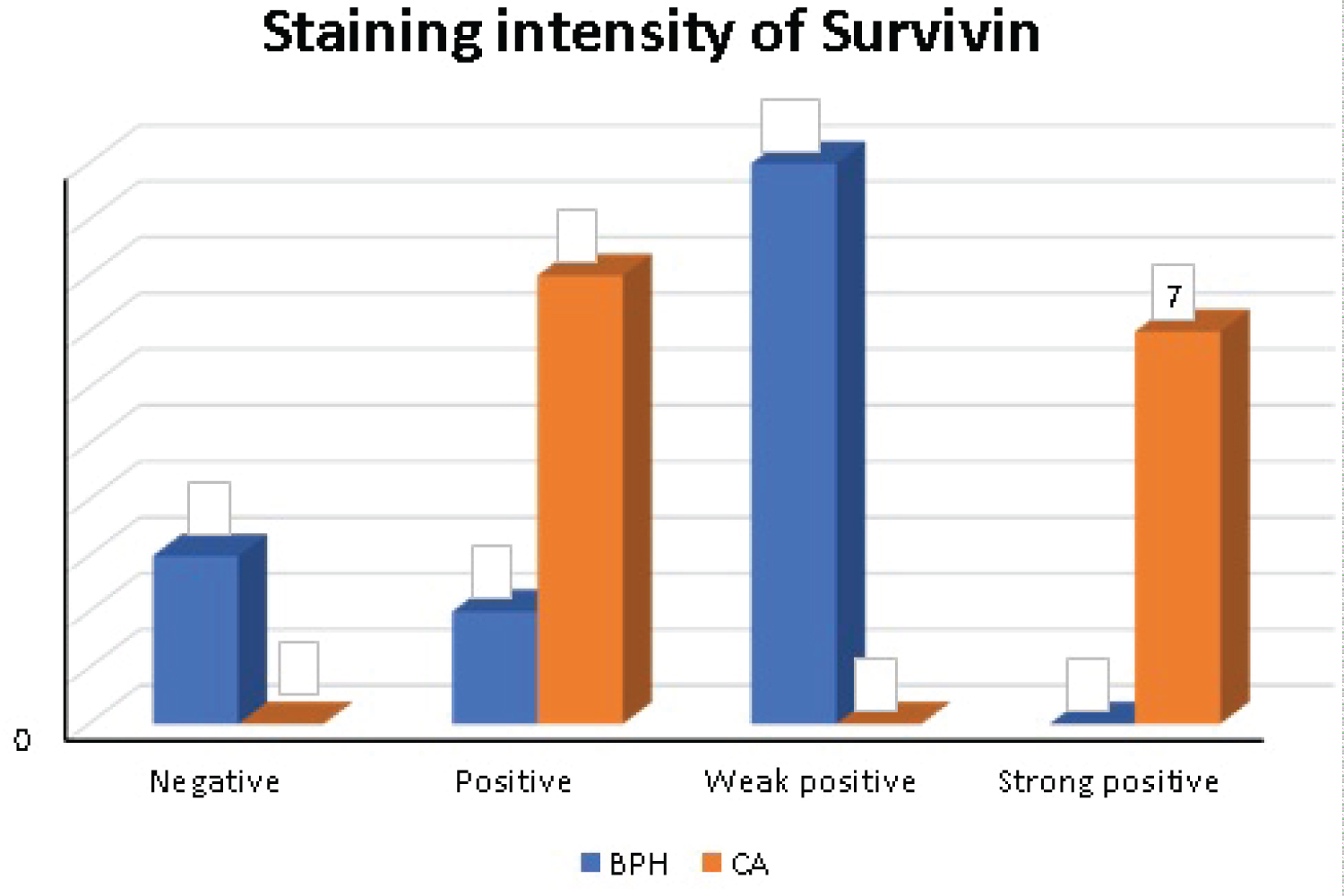 Figure 3: Distribution of cases according to staining intensity of Survivin.
View Figure 3
Figure 3: Distribution of cases according to staining intensity of Survivin.
View Figure 3
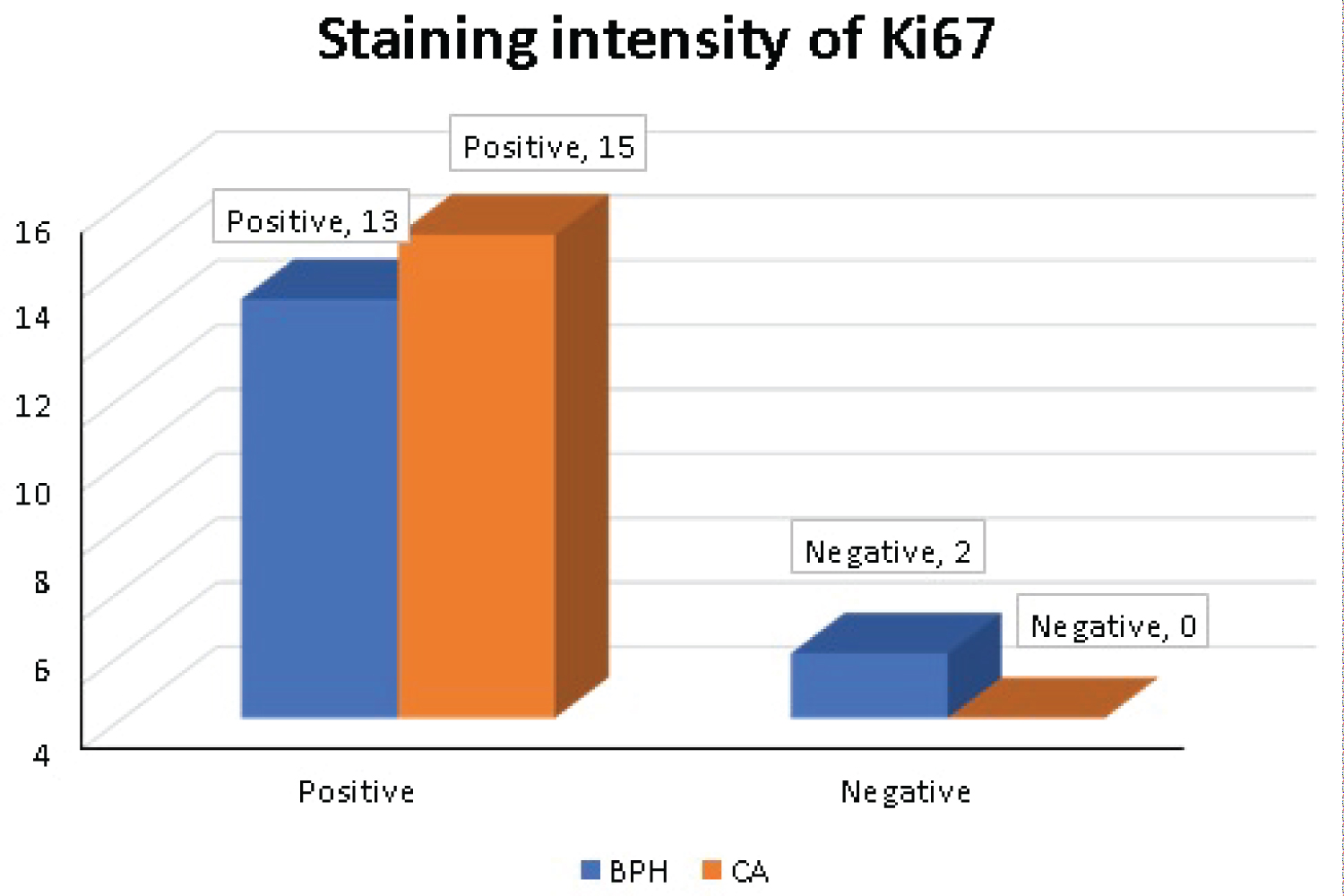 Figure 4: Distribution of cases according to staining intensity of Ki67.
View Figure 4
Figure 4: Distribution of cases according to staining intensity of Ki67.
View Figure 4
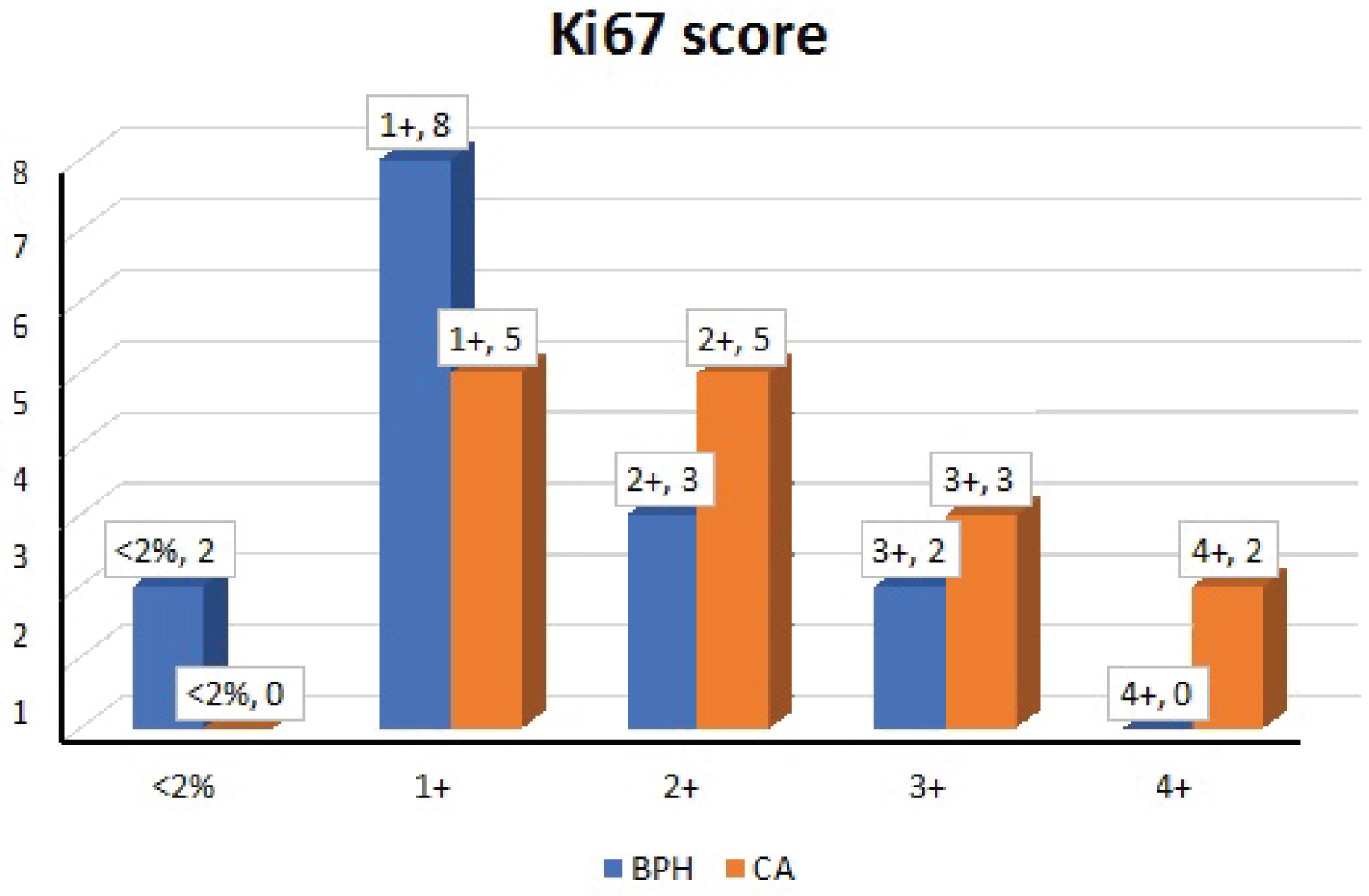 Figure 5: Distribution of cases according to grades of Ki67.
View Figure 5
Figure 5: Distribution of cases according to grades of Ki67.
View Figure 5
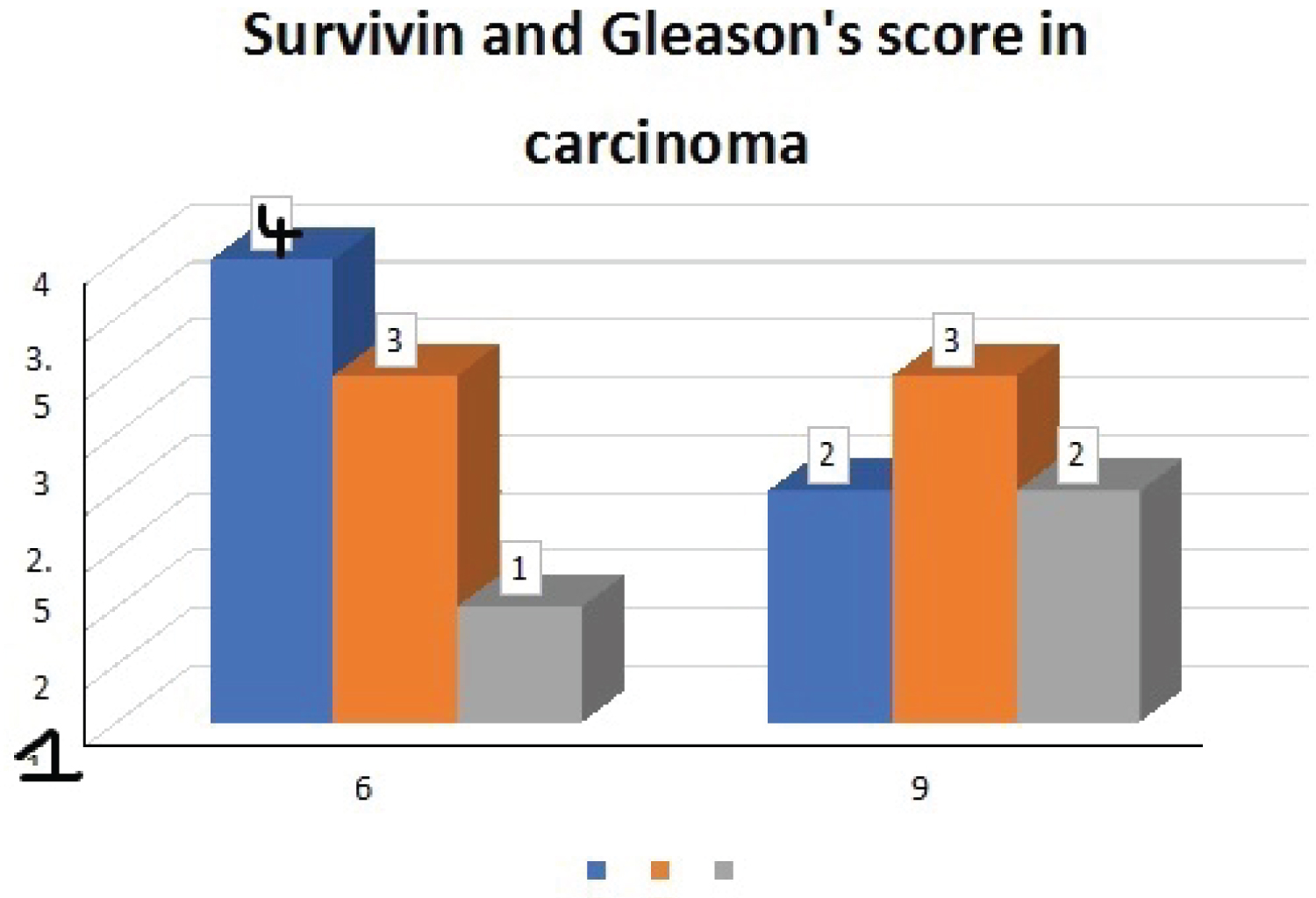 Figure 6: Frequency of expression of Survivin in Prostate cancer and its correlation with Gleason's score.
View Figure 6
Figure 6: Frequency of expression of Survivin in Prostate cancer and its correlation with Gleason's score.
View Figure 6
Table 1: Distribution of age groups. View Table 1
Table 2: Distribution of cases according to Gleason's score. View Table 2
Table 3: Distribution of cases according to staining intensity of Survivin. View Table 3
Table 4: Distribution of cases according to staining intensity of Ki67. View Table 4
Table 5: Distribution of cases according to the grades of Survivin. View Table 5
Table 6: Distribution of cases according to grades of Ki67. View Table 6
Table 7: Frequency of expression of Survivin in Prostate cancer and its correlation with Gleason's score. View Table 7
Table 8: Frequency of expression of Survivin in prostate cancer and its correlation with S.PSA. View Table 8
Table 9: Frequency of expression of Survivin in BPH and its correlation with S.PSA. View Table 9
Table 10: Frequency of expression of Ki67 in BPH and its correlation with S.PSA. View Table 10
Table 11: Frequency of expression of Ki67 in prostatic cancer and its correlation with Gleason's score. View Table 11
Table 12: Frequency of expression of Ki67 in prostatic cancer and its correlation with S.PSA. View Table 12
Table 13: Correlation between Gleason's score and S.PSA. View Table 13
Table 14: Combining 2 diagnostic tests parallel. View Table 14
There was highly significant positive correlation between the combined tests (Survivin + Ki67) and presence of adenocarcinoma prostate. While in case of BPH, there was a negligible negative correlation between the combined tests (Survivin + Ki67) and presence of BPH and it was not statistically significant.
Prostatic carcinoma is an important cause of mortality among elderly men. The use of serum prostate specific antigen (S.PSA) screening to facilitate early detection of prostate cancer has resulted in a dramatic increase in the number of prostate needle biopsies [6,7].
However, this screening has also led to over-detection and over-treatment, as elevation in S.PSA levels can also be present as a result of infection, chronic inflammation, or benign prostatic hyperplasia [1]. Thus, searching for new methods of therapy and prognosis becomes a key task.
Prostate cancer is a slow-growing malignancy that is characterized by an imbalance in the rate of cell division and cell death which mainly depends on apoptosis [1,8]. Survivin is a new and the smallest member of the inhibitor of the apoptosis family and is expressed predominantly in fetal tissue but is also found in many human malignancies.
Ki67 is a protein found in proliferating cells. Ki67 recognizes a proliferation specific nuclear antigen. Normal prostate cells proliferate slowly with low Ki67 expression.
The current study estimates the frequency of expression of Survivin and Ki67 in biopsy proven tissues of prostate cancer and benign prostatic hyperplasia along with its correlation with Gleason’s score and pre-operative S.PSA levels.
15 cases of histopathologically proven adenocarcinoma prostate and 15 cases of benign prostatic hyperplasia were selected for the study. Immunohistochemistry with Survivin and Ki67 antibodies was done on all cases and controls.
Prostatic cancer is primarily a disease of the elderly with a majority of the cases occurring in men above 65 years of age [2,9].
The age group of patients in this study ranged from 60-79 years, with a mean age group of 70.53 ± 6.42 in the adenocarcinoma group and 73.27 ± 6.51 in the benign prostatic hyperplasia group which was similar to the study done by Mansooreh Eslami, et al. [2] Zhang M, et al. [4] and Danilewicz, et al. [3].
According to the 2014 WHO/ISUP guidelines, all adenocarcinoma cases were assigned Gleason’s score. Cases with Gleason’s score 7 and 8 were the most common in our study, comprising 40% of each Gleason’s score group.
Out of the 15 adenocarcinoma cases, 53.3% (8) cases showed Survivin positivity and 46.7% (7) cases showed strong Survivin positivity.
Out of the 15 benign prostatic hyperplasia, 66.7% (10) cases showed weak positivity, 20% (3) cases showed negative staining and 13.3% (2) cases showed positive staining for Survivin. None of the benign prostatic hyperplasia cases showed strong positivity for Survivin.
There was a statistically significant difference in the Survivin score between prostatic cancer patients and benign prostatic hyperplasia cases in our study, which is similar to the study done by Jufei Gu, et al. [1]. Their study showed a positive expression rate of Survivin in prostatic cancer and benign prostatic hyperplasia tissues of 83.72% (36/43) and 35.29% (6/17), respectively. Both the differences were statistically significant (P < 0.05 and P < 0.01).
Out of 15 adenocarcinoma cases, 50% of the cases had Gleason’s score of 7 and showed Survivin staining intensity of 6. The rest of the cases had a Gleason’s score of 8 and 9 and all of them showed Survivin staining intensity of 6 and 9. As the Gleason’s score increased, the degree of Survivin expression also increased. Even though there was no statistical significance, the findings were similar to the study done by Mansooreh Eslami, et al. [2] which showed that; higher the Gleason’s score, greater the degree of Survivin expression staining. In their study most of the adenocarcinoma samples (60.4 %) with a Gleason grade of ≥ 7 were 3+ positive for Survivin.
In our study, the mean S.PSA level in adenocarcinoma patients was 286.15 ± 497.77 and in benign prostatic hyperplasia was 12.83 ± 19.04.
Among the adenocarcinoma cases, 50% of the cases had Gleason’s score of 7, which is a lower Gleason’s score group when compared to Gleason’s score group 8 and 9. Rest of the 50% of the cases were in Gleason’s score 8 and 9. 53.3% of the total adenocarcinoma cases showed Survivin score of 6, which implies a positive expression of Survivin and rest of the 46.7% cases showed a score of 9 which implies strong Survivin positivity. The cases with strong positive Survivin staining, had a higher S.PSA levels when compared to the cases with positive Survivin staining, even though this finding was not statistically significant. In a similar study done by done by Danilewicz, et al. [3] showed positive correlation between immunoexpression of Survivin and S.PSA levels in adenocarcinoma cases, but it did not reach statistical significance. In their study, the benign prostatic hyperplasia cases also showed correlations; but were weak and not significant.
In our study, the frequency of expression of Survivin in benign prostatic hyperplasia showed a high statistically significant correlation with the S.PSA value.
Even though there was a statistically significant difference in the Survivin score between benign prostatic hyperplasia and adenocarcinoma cases; the study did not show any statistically significant correlation between the expression of Survivin in adenocarcinoma prostate and Gleason’s score. Thus, the marker cannot be used to evaluate the aggressiveness of the adenocarcinoma which is related to Gleason’s score.
A study done by Fengzhi Li, et al. [9] reviewed the current cancer therapeutic strategy using Survivin as a target, which can be classified into five categories: (i) Inhibitors that disrupt Survivin interactions with its partner proteins; (ii) Inhibitors that disrupt Survivin homodimerization; (iii) Inhibitors that decrease Survivin gene transcription; (iv) Inhibitors that induce Survivin mRNA degradation; and (v) Survivin or its peptide for immunotherapy.
Even though the Survivin is not used as an anticancer drug in prostate cancer currently; further research in this area can lead to the discovery of Survivin based targeted therapy for prostatic adenocarcinoma and treatment.
Out of the 15 adenocarcinoma patients, 33.3% of cases showed 2+ and 1+ Ki67 positivity, and out of 15 benign prostatic hyperplasia patients, 53.3% of cases showed 1+ Ki67 positivity.
The Ki67 expression was more in in adenocarcinoma cases more than in benign prostatic hyperplasia.
The frequency of expression of Ki67 in benign prostatic hyperplasia and its correlation with S.PSA showed a P value of 0.855; which implies that there is no significant correlation between the parameters.
Frequency of expression of Ki67 in prostatic cancer and its correlation with S. PSA and Gleason’s score showed a p-value of < 0.05 and 0.277 respectively. The frequency of expression of Ki67 in prostatic cancer showed a statistically significant correlation with S.PSA levels. There was no statistically significant correlation between Ki67 expression and Gleason’s score. In a study done by Siddharth Gangwar, et al. [10] showed that there was no significant (p > 0.05) association of S.PSA levels with Ki67 among prostatic adenocarcinoma cases but showed significant association of Gleason’s score with Ki67 expression. In their study, the frequency of expression of Ki67 is significantly up regulated in prostatic carcinomas and increased expression is usually noted in aggressive and high-grade prostatic tumors.
Our study evaluated the correlation between Gleason’s score and S.PSA levels which showed a P value of 0.363 implying that there is no significant correlation between the parameters.
Our study also evaluated the efficacy of combining the Survivin and Ki67 immunohistochemical markers in evaluating adenocarcinoma prostate and benign prostatic hyperplasia. There was a highly significant positive correlation between the combined tests (Survivin + Ki67) and the presence of adenocarcinoma prostate. While in the case of benign prostatic hyperplasia, there was a negligible negative correlation between the combined tests (Survivin + Ki67) and the presence of benign prostatic hyperplasia and it was not statistically significant (Figure 7, Figure 8, Figure 9, Figure 10, Figure 11, Figure 12, Figure 13, Figure 14, Figure 15, Figure 16, Figure 17, Figure 18, Figure 19 and Figure 20).
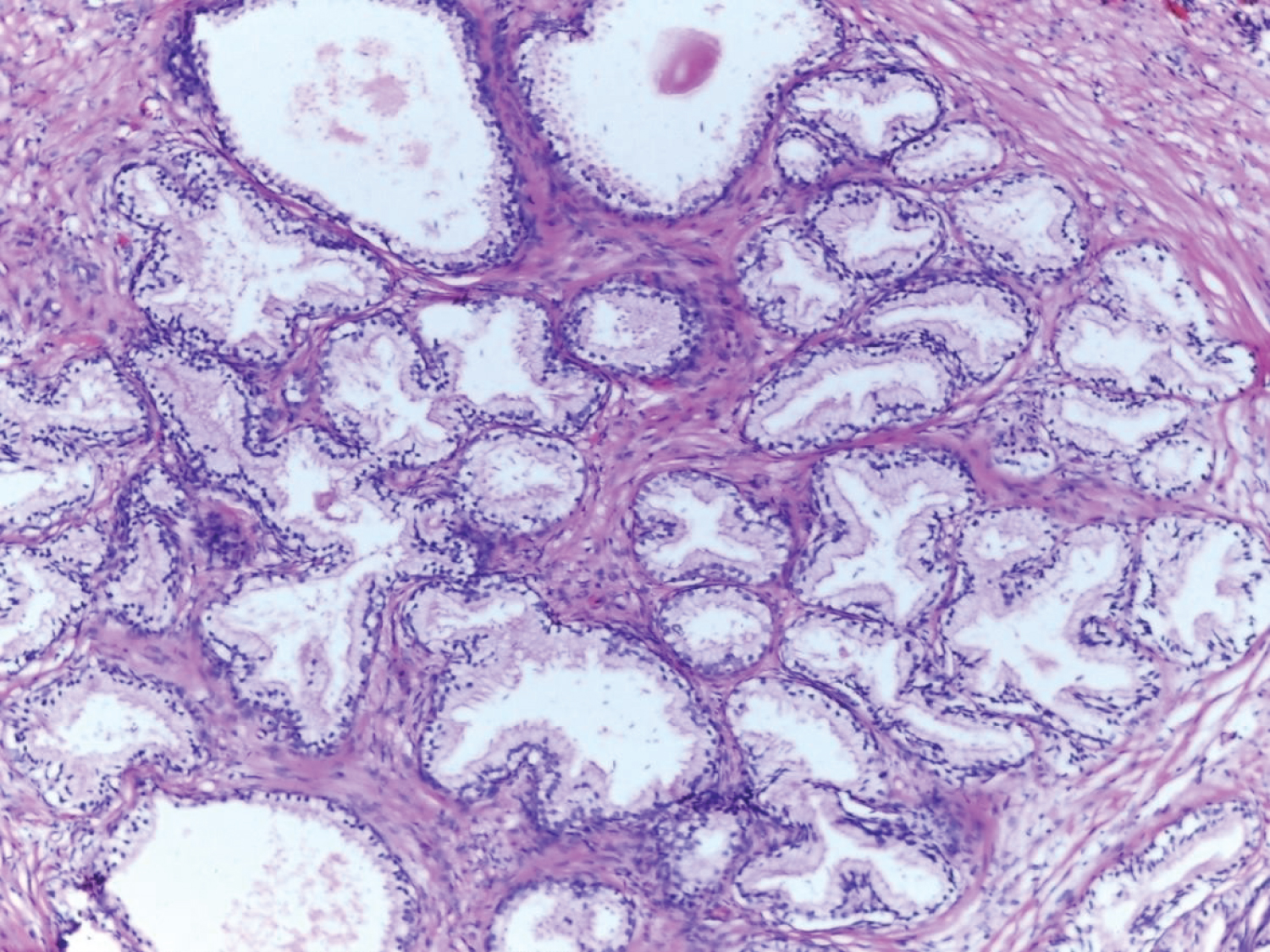 Figure 7: Histology of benign prostatic hyperplasia tissue (10x).
View Figure 7
Figure 7: Histology of benign prostatic hyperplasia tissue (10x).
View Figure 7
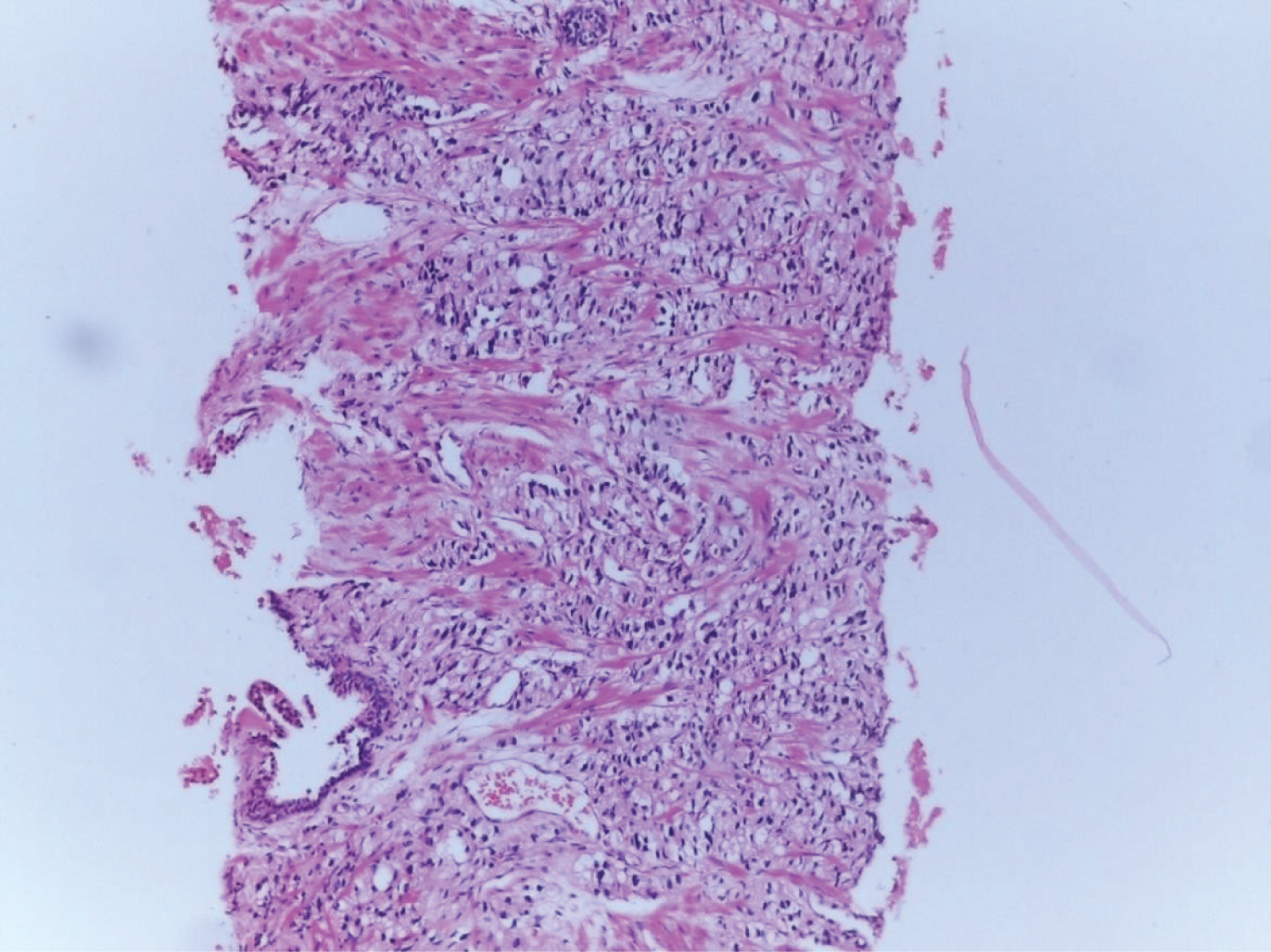 Figure 8: Adenocarcinoma prostate Gleason's score 4 + 4 (10x).
View Figure 8
Figure 8: Adenocarcinoma prostate Gleason's score 4 + 4 (10x).
View Figure 8
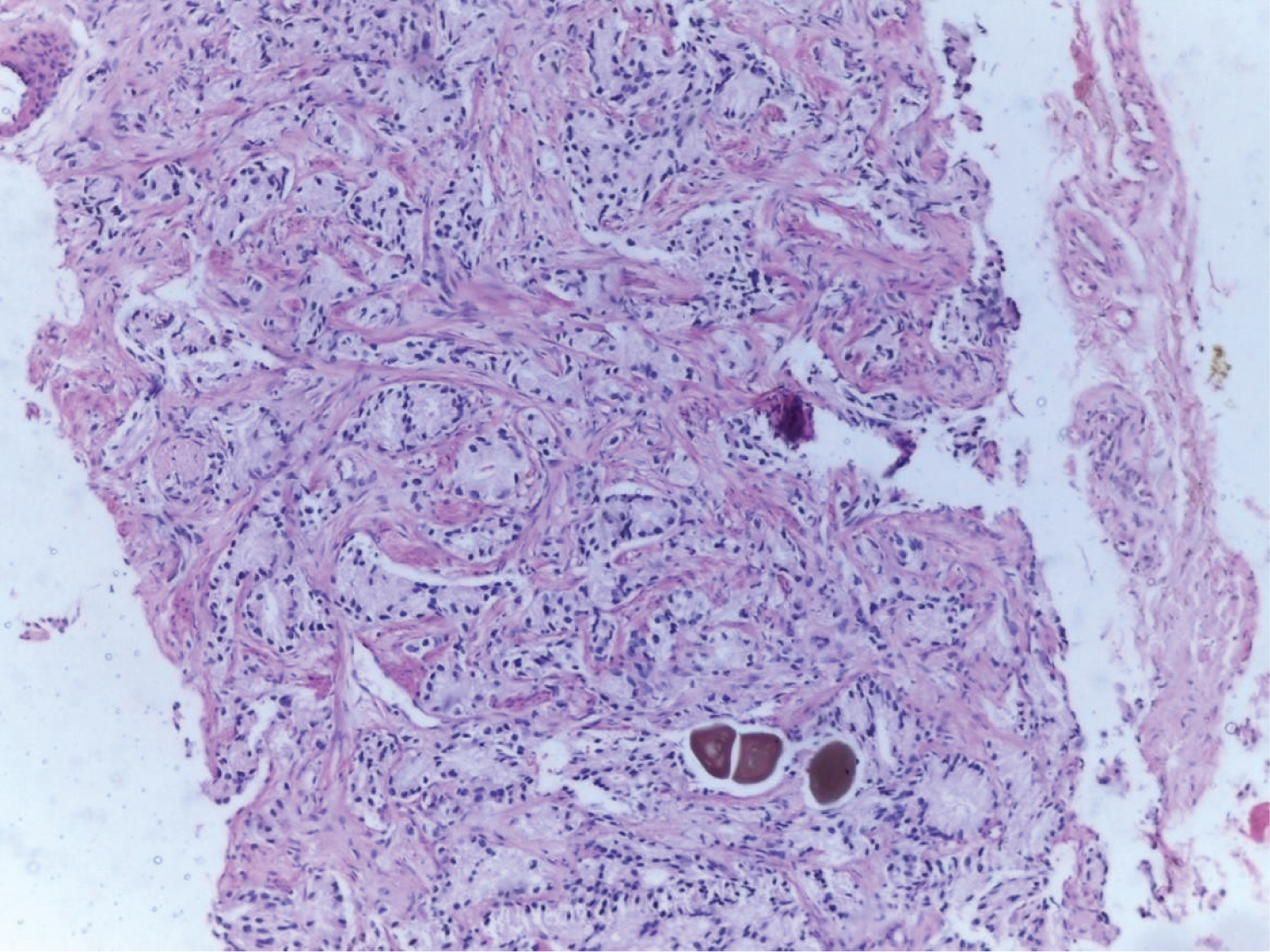 Figure 9: Adenocarcinoma Prostate Gleason's score 4 + 4 = 9.
View Figure 9
Figure 9: Adenocarcinoma Prostate Gleason's score 4 + 4 = 9.
View Figure 9
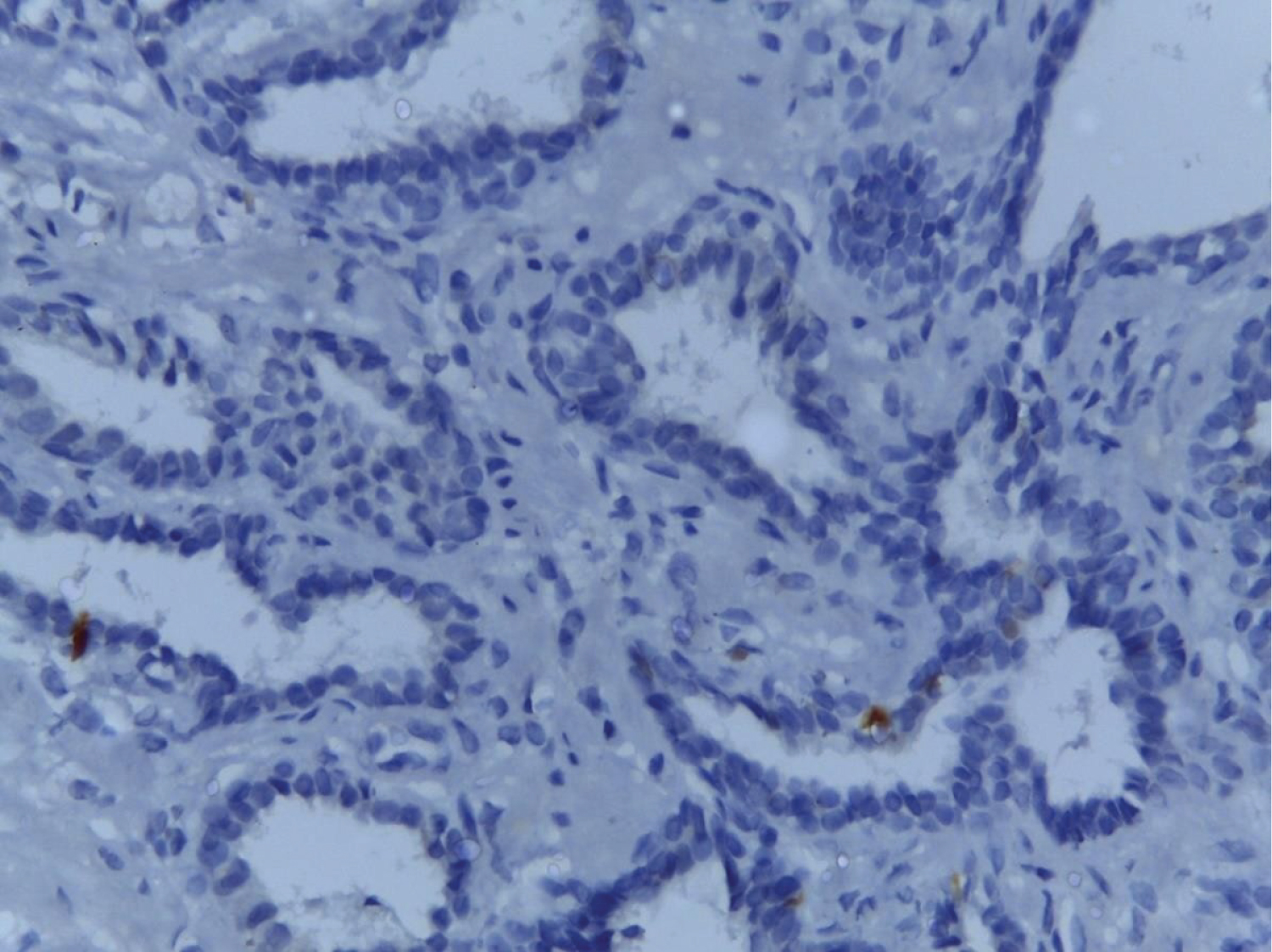 Figure 10: Benign prostatic hyperplasia showing negative Survivin staining-score- 1 (40x).
View Figure 10
Figure 10: Benign prostatic hyperplasia showing negative Survivin staining-score- 1 (40x).
View Figure 10
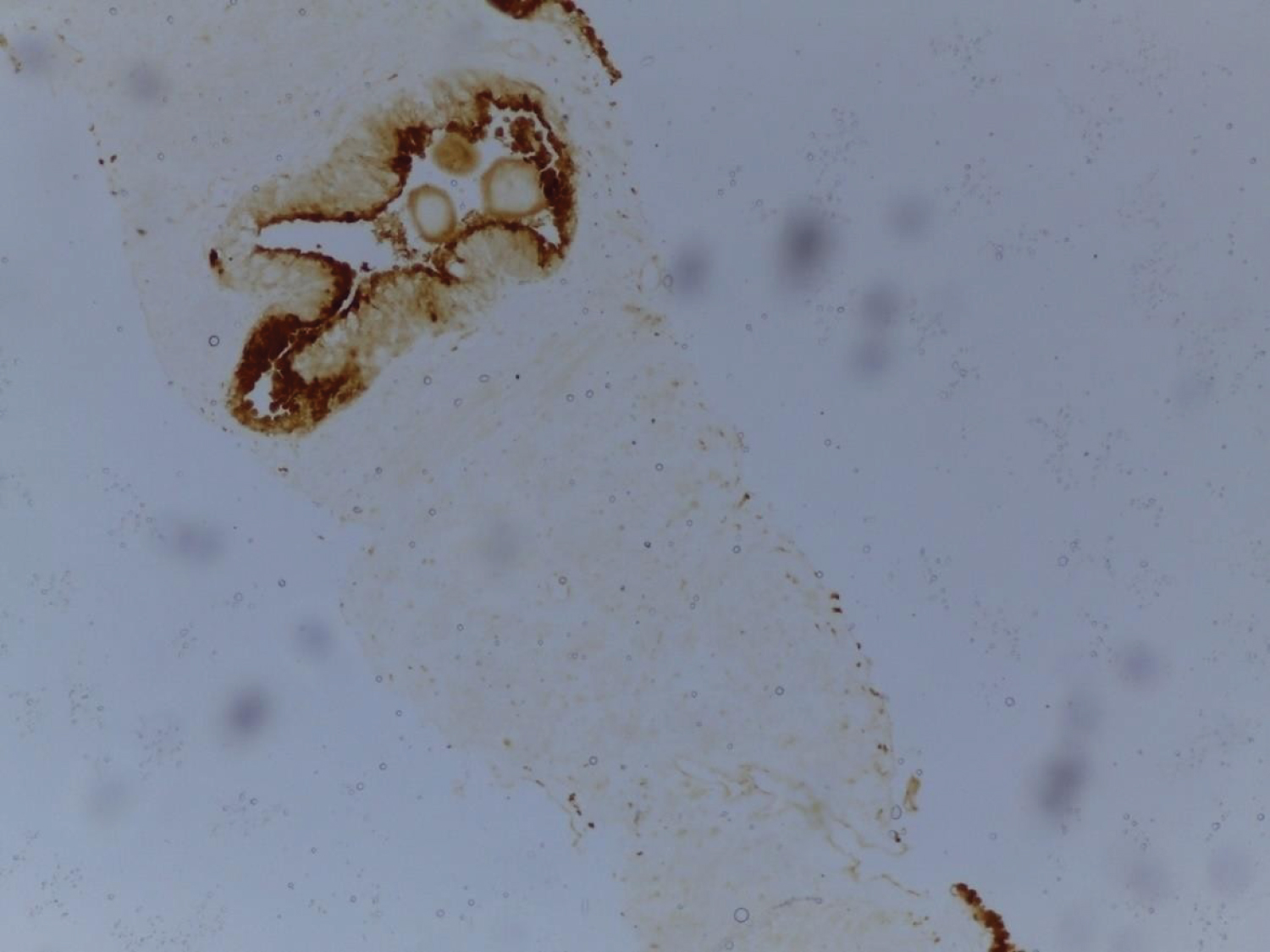 Figure 11: Benign prostatic hyperplasia showing weak positive Survivin staining; score- 2.
View Figure 11
Figure 11: Benign prostatic hyperplasia showing weak positive Survivin staining; score- 2.
View Figure 11
 Figure 12: Benign prostatic hyperplasia showing positive Survivin staining; score- 3.
View Figure 12
Figure 12: Benign prostatic hyperplasia showing positive Survivin staining; score- 3.
View Figure 12
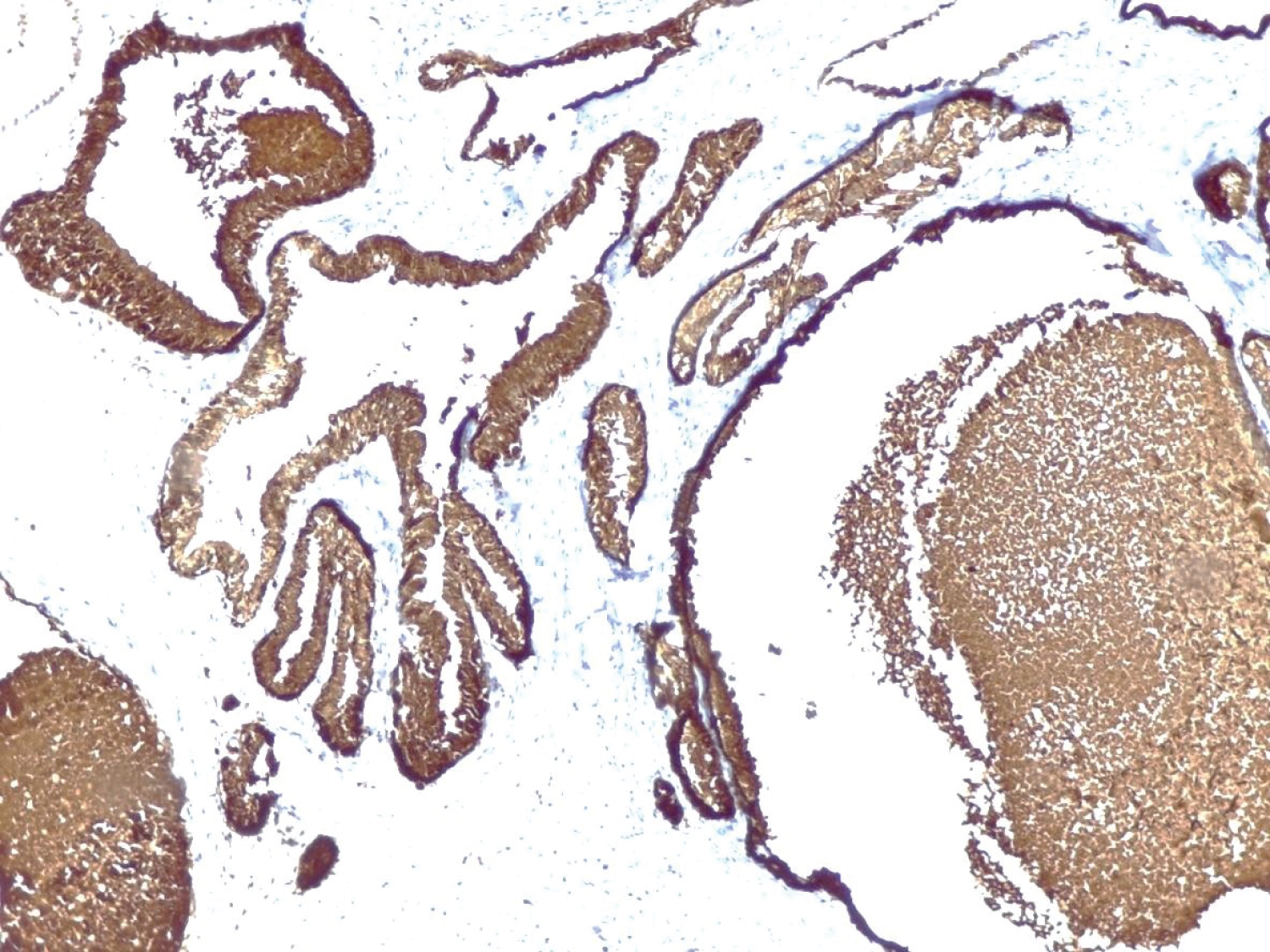 Figure 13: Benign prostatic hyperplasia showing positive Survivin staining; score- 4.
View Figure 13
Figure 13: Benign prostatic hyperplasia showing positive Survivin staining; score- 4.
View Figure 13
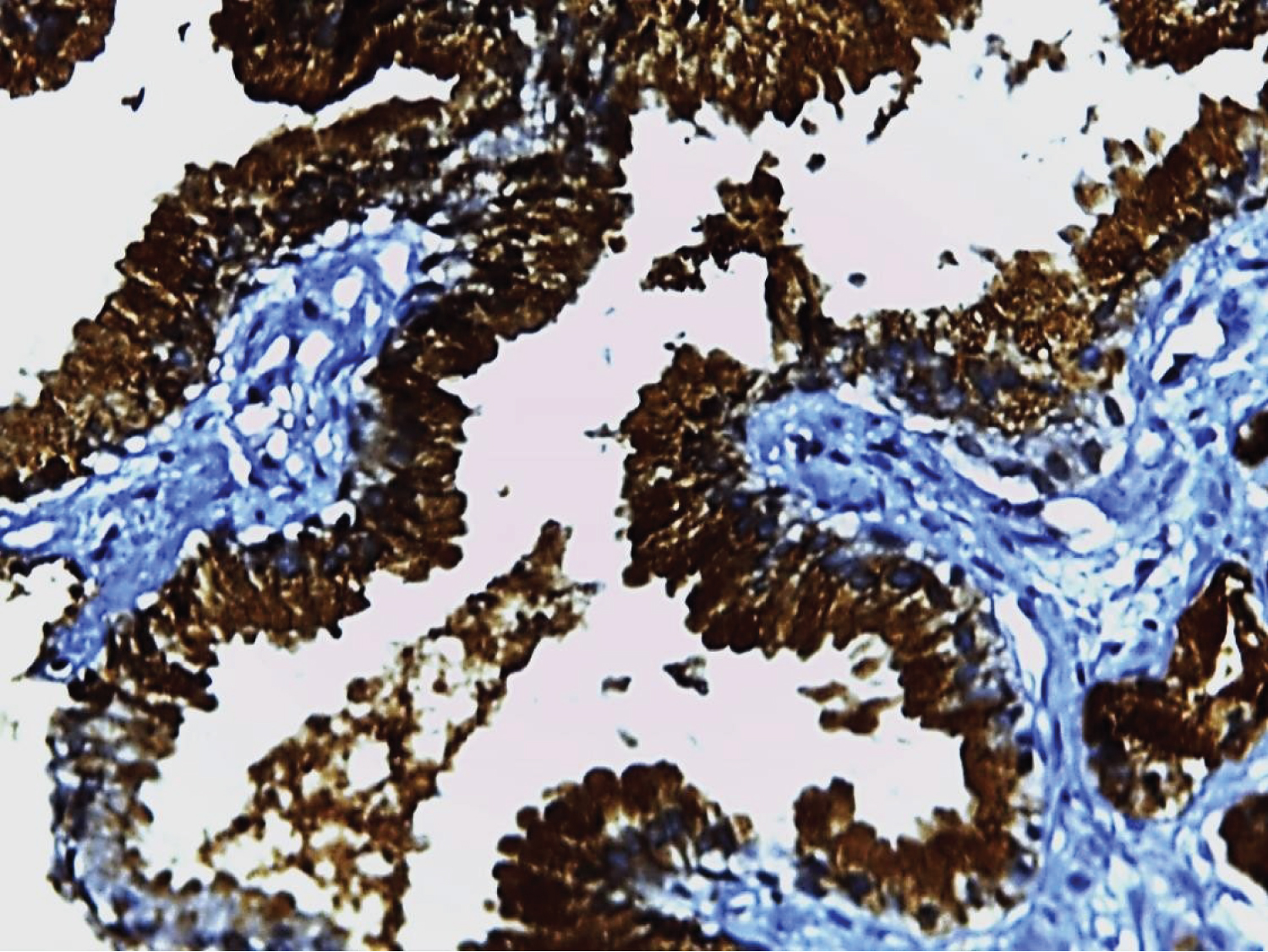 Figure 14: Adenocarcinoma Prostate Gleason's score 3 + 4 = 7; Survivin staining score - 6.
View Figure 14
Figure 14: Adenocarcinoma Prostate Gleason's score 3 + 4 = 7; Survivin staining score - 6.
View Figure 14
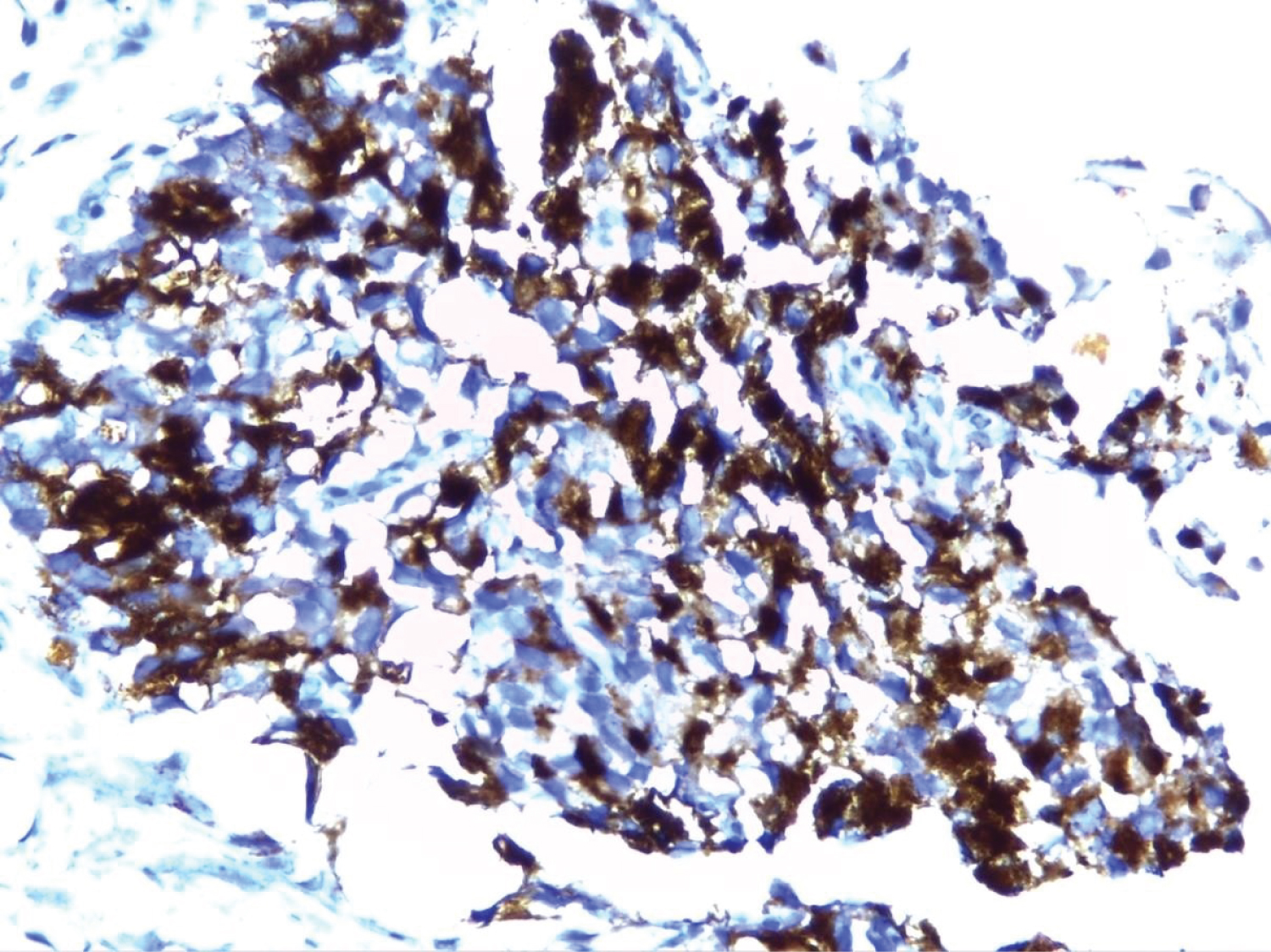 Figure 15: Adenocarcinoma Prostate Gleason's score 4 + 5 = 9; Survivin staining score- 9.
View Figure 15
Figure 15: Adenocarcinoma Prostate Gleason's score 4 + 5 = 9; Survivin staining score- 9.
View Figure 15
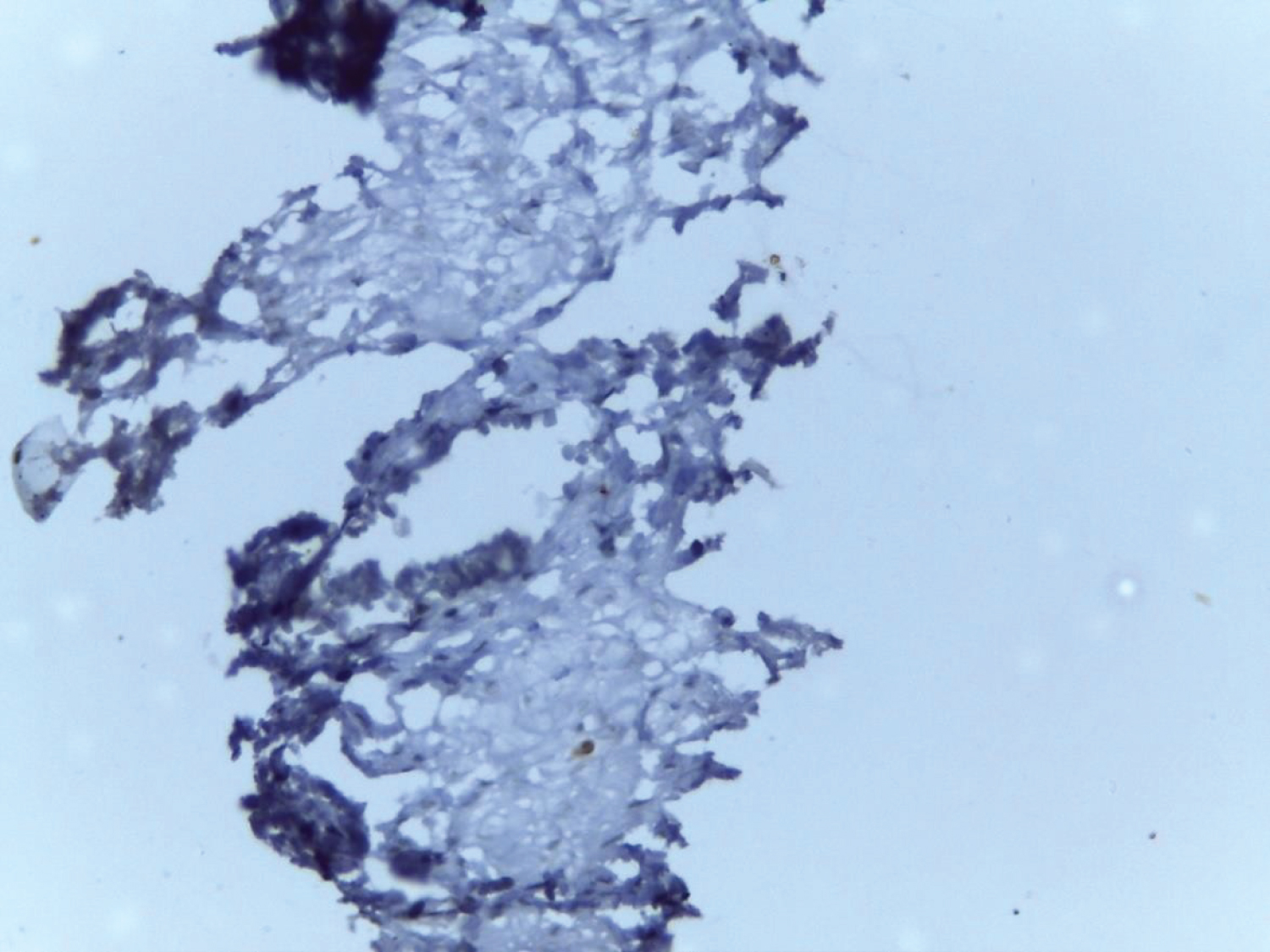 Figure 16: Benign prostatic hyperplasia showing negative Ki67 (10x).
View Figure 16
Figure 16: Benign prostatic hyperplasia showing negative Ki67 (10x).
View Figure 16
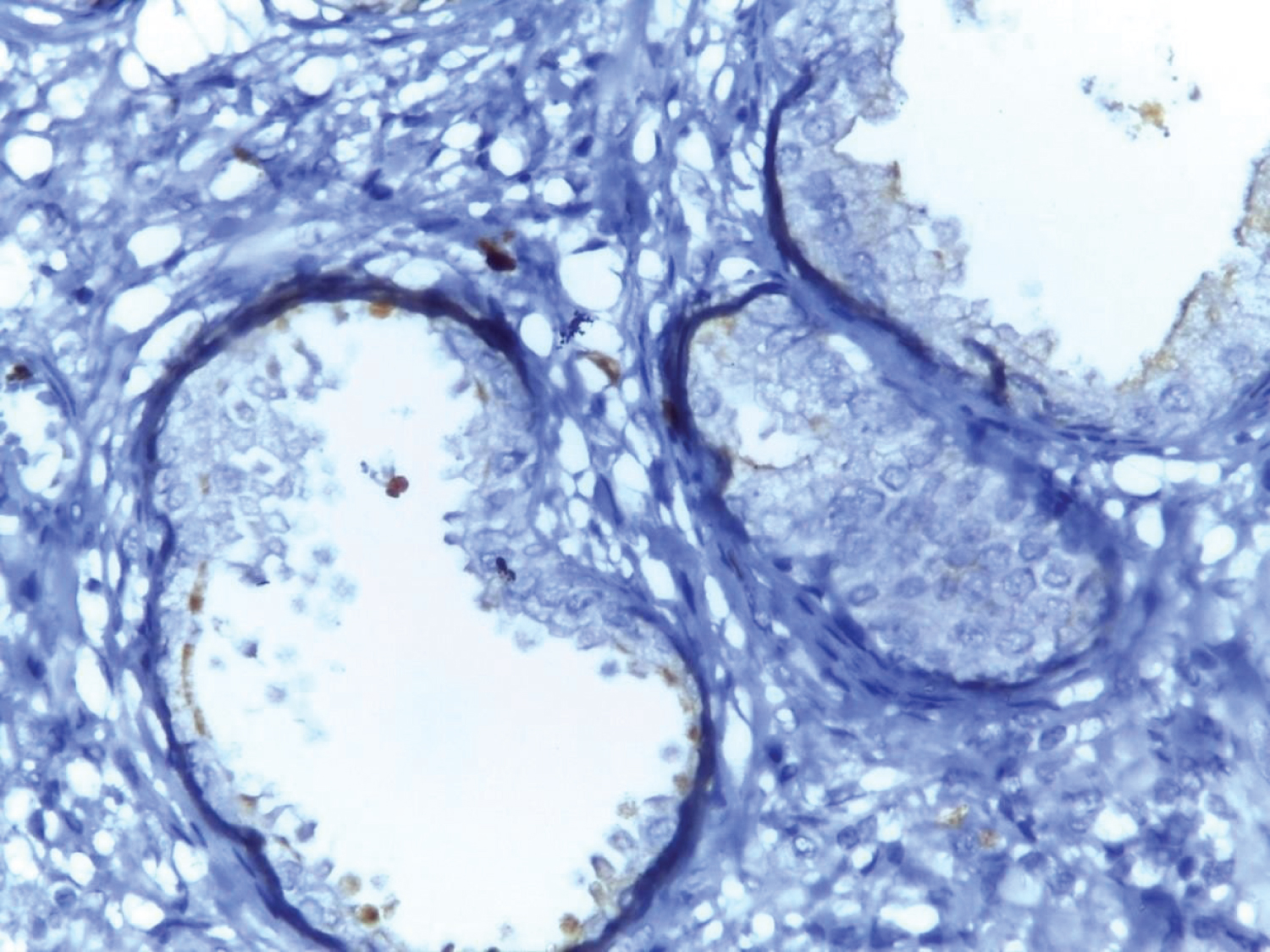 Figure 17: Benign prostatic hyperplasia showing 1 + Ki67 positivity (10x).
View Figure 17
Figure 17: Benign prostatic hyperplasia showing 1 + Ki67 positivity (10x).
View Figure 17
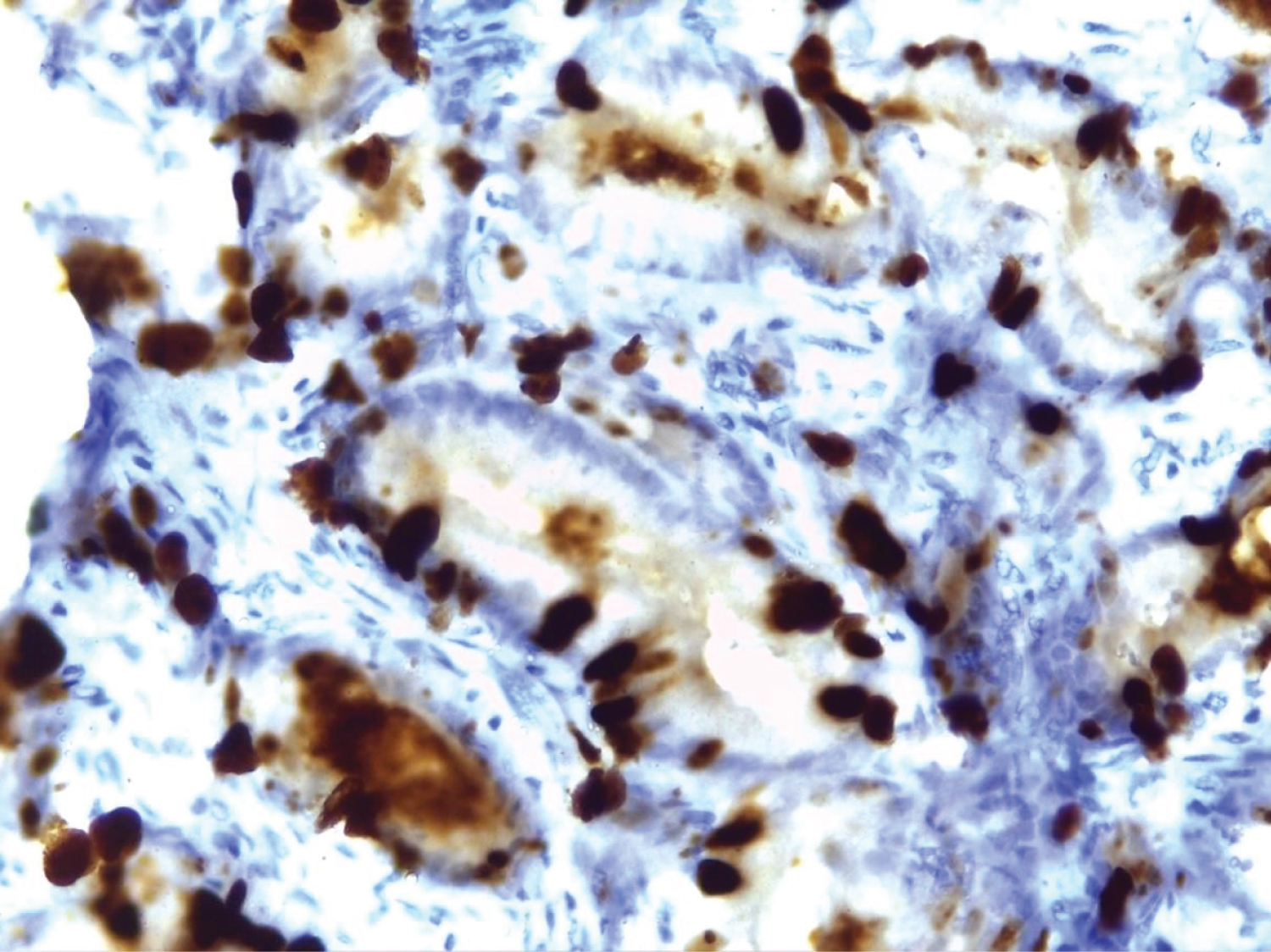 Figure 18: Benign prostatic hyperplasia showing 2 + Ki67 positivity (40x).
View Figure 18
Figure 18: Benign prostatic hyperplasia showing 2 + Ki67 positivity (40x).
View Figure 18
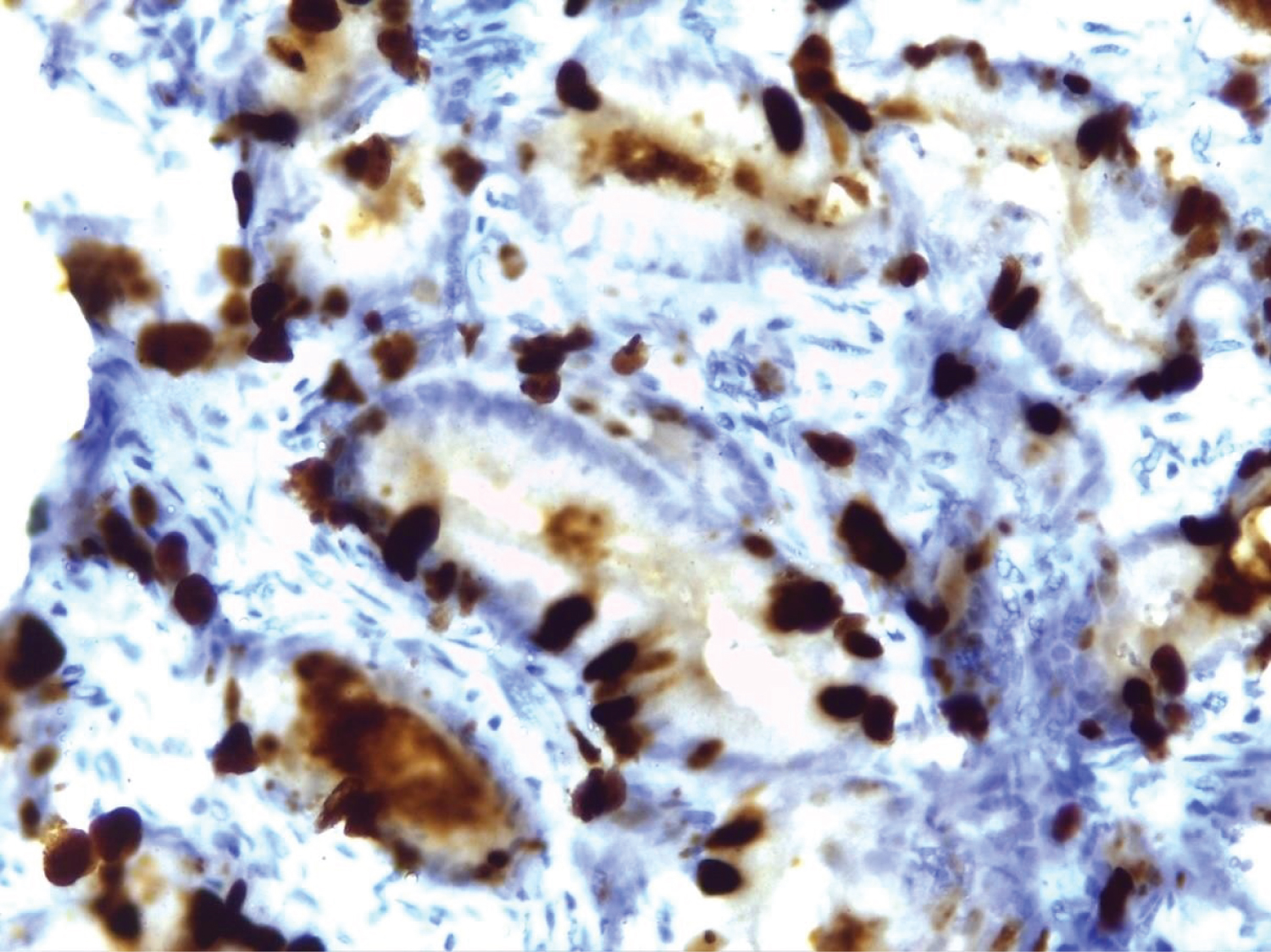 Figure 19: Adenocarcinoma prostate showing 3 + Ki67 positivity (10x).
View Figure 19
Figure 19: Adenocarcinoma prostate showing 3 + Ki67 positivity (10x).
View Figure 19
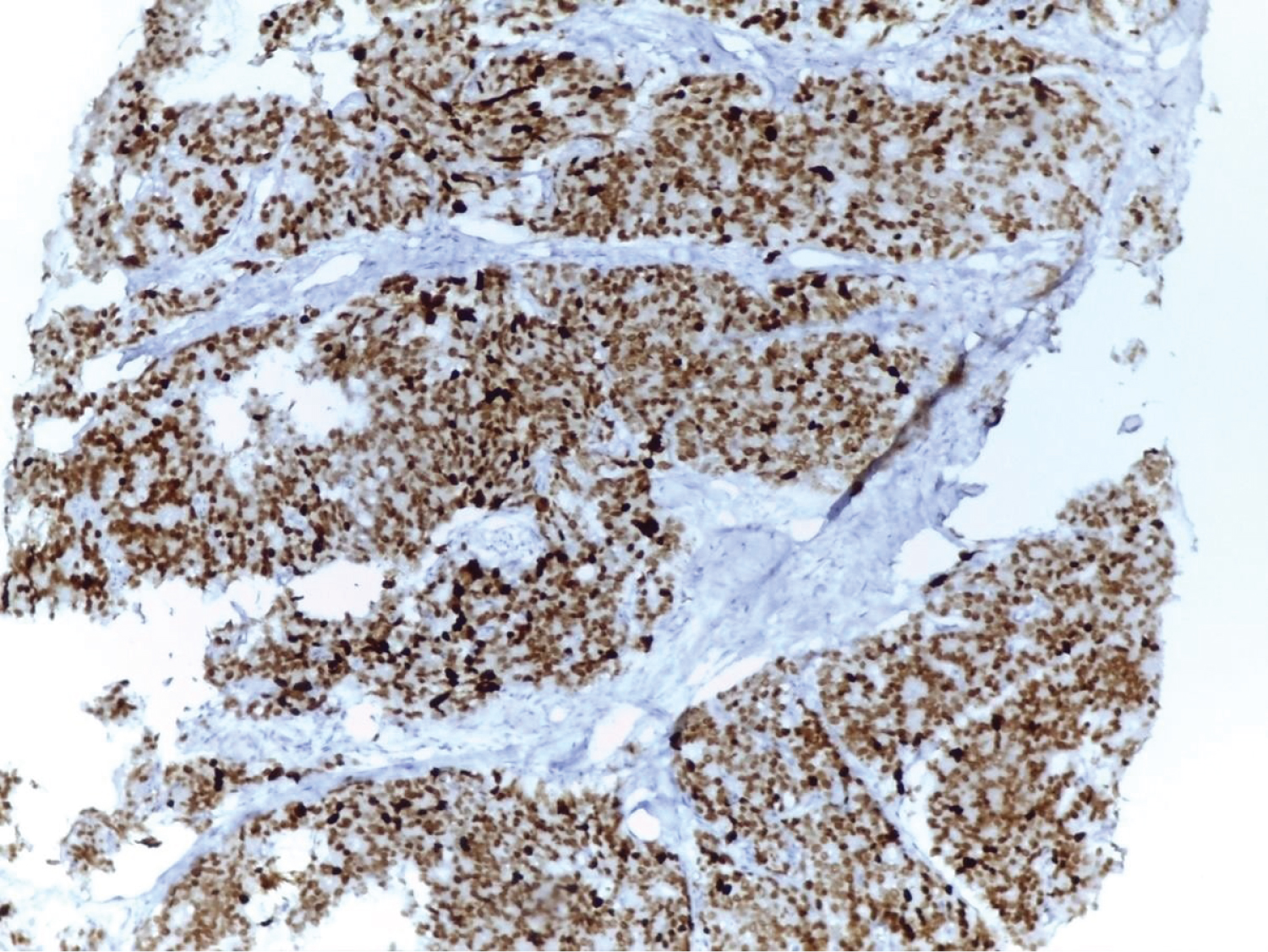 Figure 20: Adenocarcinoma prostate showing 4 + Ki67 positivity (10x).
View Figure 20
Figure 20: Adenocarcinoma prostate showing 4 + Ki67 positivity (10x).
View Figure 20
Less number of sample size.
None.
No external funds Received.