A perineurioma is a rare benign peripheral nerve sheath tumor derived from perineurial cells. Based on clinical and pathologic features, perineuriomas can be classified into two subtypes: Intraneural perineurioma and the extraneural perineurioma. Soft tissue perineuriomas are rare. Herein, we report a case of Extraneural perineurioma localized in the back.
Extraneural perineurioma, Benign peripheral nerve sheath tumor
The perineurioma is an uncommon, nearly always benign peripheral nerve-sheath lesion arising from perineurial cells. Typically divided into the intraneural or the extraneural (soft tissue) variants, That includes three forms: The sclerosing form, the reticular form and the the soft tissue form. The perineurioma is thought to represent a clonal proliferation of perineurial cells that surround the periphery of nerve fascicles. The extraneural perineurioma is typically unassociated with peripheral nerves and presents as a solitary nodule or subcutaneous mass [1]. Herein, we report a case of perineurioma localized in the back.
A 54-year-old male presented with a firm, painless nodule of several months duration that had been slowly increasing in size. There was no history of trauma or previous surgery. The nodule was easily moveable. The lesion was approximately 10 mm in greatest dimension and the overlying surface was smooth and pink. An excisional biopsy of the nodule was performed (Figure 1).
 Figure 1: A raised erythematous telangiectatic nodule of the lower back.
View Figure 1
Figure 1: A raised erythematous telangiectatic nodule of the lower back.
View Figure 1
Histologic examination revealed a circumscribed but unencapsulated nodular proliferation of small spindle to oval epitheliod cells with indistinct cell borders forming ill-defined fascicles in a dense sclerotic collagenous matrix (Figure 2). Immunohistochemical analysis performed as previously, 4-6 revealed immunoreactivity of the neoplastic cells for Vimentin, EMA, CD34, and their negativity for S100, CD117.
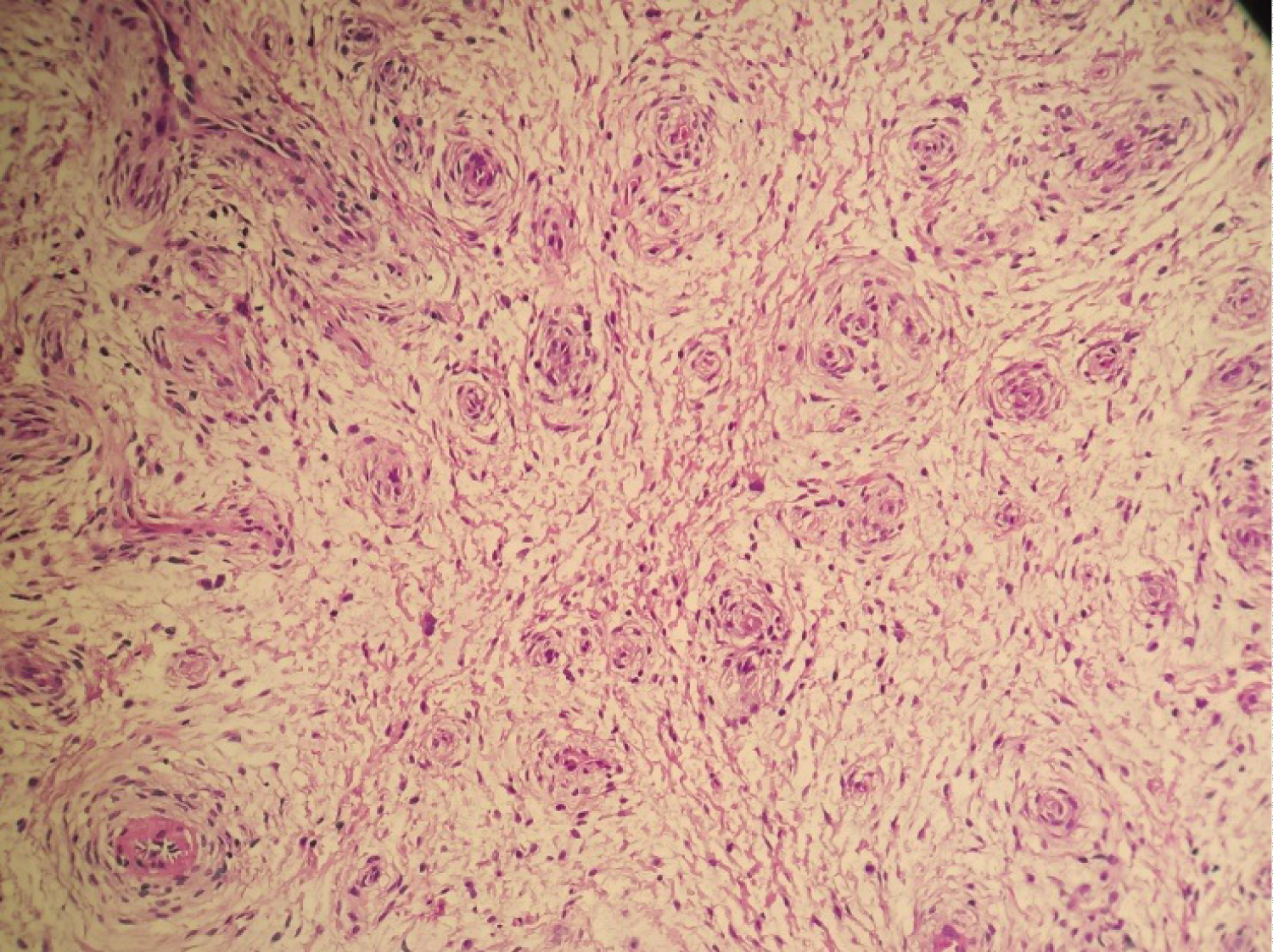 Figure 2: Spindle cell proliferation in a stroma rich in vasacules (HE ×40).
View Figure 2
Figure 2: Spindle cell proliferation in a stroma rich in vasacules (HE ×40).
View Figure 2
The patient had an uncomplicated postoperative recovery and showed no signs of recurrence at a 2-years follow-up appointment.
A perineurioma (PN) is a rare benign peripheral nerve sheath tumor derived from perineurial cells, which was first described in 1978 by Lazarus and Trombetta. Based on clinical and pathologic features, PNs can be classified into two major subtypes: Intraneural perineurioma (IPN) and the extraneural perineurioma (EPN). IPNs enlarge the affected peripheral nerve and can cause sensory and motor deficits. In particular, they exhibit a predilection for the major peripheral nerves of the upper limbs. In contrast, EPNs are not associated with peripheral nerves and most often present as an asymptomatic, subcutaneous nodule or mass [2].
Unusual EPN variants include the sclerosing type, the reticular type and the soft tissue type.
Extraneural soft tissue perineurioma usually occurs in young to middle-aged adults predominantly female. Clinically, it presents as in our patient as a painless skin nodule that has been evolving for several years. It is most often found on the extremities, especially on the fingers,as well as on the trunk. The head and neck may be affected, including the oral cavity [3].
Peripheral nerves are made up of a set of fascicles within which the nerve fibers are distributed. The fascicle is limited by the perineurium, which consists of of layers of perineural cells of fibroblastic origin separated by collagen bundles. Perineuromas derive from the perineural cells of the perineurium [4,5].
The differential diagnosis of soft tissue perineuriomas is essentially with peripheral nerve sheath tumors, notably schwannomas and neurofibromas.
Histologically, the tumor is made of a more or less dense proliferation of elongated spindle cells, with fine wavy nuclei, well limited but not encapsulated. The cells are usually thin, with eosinophilic cytoplasm. They are arranged in short bundles with cellular coils, and sometimes a storiform or lamellar arrangement. Immunohistochemically, the tumor cells express EMA and do not express EMA and S100 protein [6].
There are malignant forms of perineurioma They represent less than 5% of malignant tumors of the peripheral nerve sheaths and essentially pose a problem of differential diagnosis with soft tissue sarcomas.
The standard treatment for perineurioma is surgery; the outcome is usually favorable without recurrence after total removal of the nodule. Cutaneous metastases and recurrences are rare [7].
We reported here the clinicopathologic findings of an uncommon benign tumor; PNs are peripheral nerve sheath tumors derived from perineurial cells Because their features mimic other benign and malignant soft tissue lesions, histopathology is needed for definitive diagnosis.
None of the authors has a conflict of interest to declare.