Pseudoxanthoma elasticum (PXE) is an inherited disease of elastic tissue primarily affecting the skin, eyes, and arteries. We report a clinical case to emphasize the need for early diagnosis and follow-up, a multidisciplinary approach and the management of complications. A 62-year-old patient consulted for wrinkled layers of papules typically "shagreen". The skin lesions were disseminated throughout the body but predominated in the folds, abdomen and neck. This generalized form would be due to the delay in diagnosis. The extra cutaneous lesions make all the seriousness of this disease which requires lifelong monitoring, The ophthalmologic manifestations of PXE are potentially the most serious. In any case, they are the most dreaded by patients. There is a risk of reduced visual acuity and sometimes blindness. PXE patients frequently develop early peripheral atherosclerosis, from the fourth decade , manifested by decreased peripheral pulses, and sometimes intermittent claudication. Cardiovascular clinical signs in PXE patients may also include arterial hypertension, and exceptionally signs of angina pectoris. Other attacks are frequent (rheumatological, renal...). No specific treatment is available to date but A number of etiological treatments to prevent complications are currently being developed.
Pseudoxanthoma elasticum, Elastopathy, Angioid streaks
Pseudoxanthoma elasticum (PXE) or systematized elastorrhexia or Gronblad-Strandberg syndrome is an inherited disease of elastic tissue mainly affecting the skin, eyes, arteries and heart [1]. It affects both sexes with a female predominance. Pseudoxanthoma elastica is a hereditary systemic metabolic disease, of autosomal recessive transmission, caused, in the majority of cases, by variants of the ABCC6 gene located on the short arm of chromosome 16. The condition is characterized, on the skin, by the appearance of yellowish plaques, made up of often linear papules, located at the base of the neck, shoulders, armpits and elbow folds [2]. We report a generalized form, to emphasize the need for early diagnosis and follow-up, the multidisciplinary approach and the management of complications.
A 62-year-old patient, married and father of five children, with a family history of two 58-year-old brothers, who have been in a specialist follow-up in Belgium for 52 years because of a histologically confirmed elastic pseudoxanthoma, presented in consultation of dermatology with skin lesions dating back to the age of 20.
There were no cardiovascular, metabolic, digestive or renal defects. On clinical examination, there was no pruritus, pain, or inflammatory signs; the patient had a good general condition and the cutaneous signs were represented by small diffuse yellow papules on the level of the neck, torso and abdomen, the skin had an appearance of wrinkled sheets in "shagreen" or "draped" by progressive coalescence of the papules (Figure 1a, Figure 1b, Figure 2 and Figure 3). On palpation, the skin has lost its elasticity. No mucosal lesions were observed.
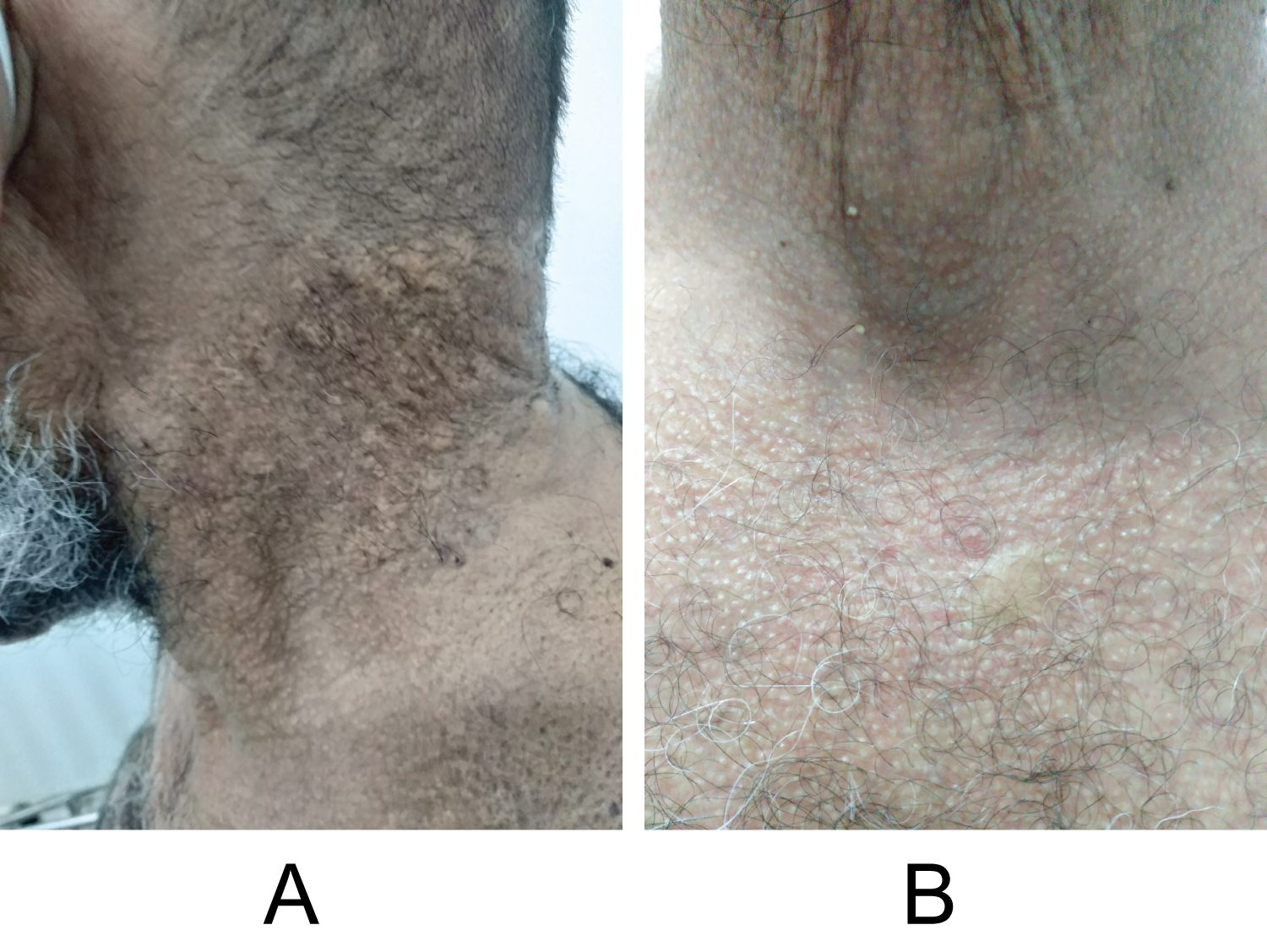 Figure 1(a,b): Pseudoxanthoma elasticum papules of the neck and chest.
View Figure 1
Figure 1(a,b): Pseudoxanthoma elasticum papules of the neck and chest.
View Figure 1
 Figure 2: Elastic pseudoxanthoma. Appearance in crumpled layers next to the folds and on the surrounding skin.
View Figure 2
Figure 2: Elastic pseudoxanthoma. Appearance in crumpled layers next to the folds and on the surrounding skin.
View Figure 2
 Figure 3: Elastic pseudoxanthoma. Appearance in shagreen next to the inguinal folds and on the thighs.
View Figure 3
Figure 3: Elastic pseudoxanthoma. Appearance in shagreen next to the inguinal folds and on the thighs.
View Figure 3
Histology: Slightly acanthotic epidermis, its basal layers are hyperpigmented. Within the middle dermis, presence of fragmented elastic fibers with a pigtail appearance also visualized on orcein staining.
The examination carried out in ophthalmology: found a drop in visual acuity, with angioid streaks (Figure 4). Cardiac echo-Doppler and upper digestive fibroscopy were normal; there was no vascular or digestive involvement. The patient received information about his illness, supportive psychotherapy and a monitoring schedule.
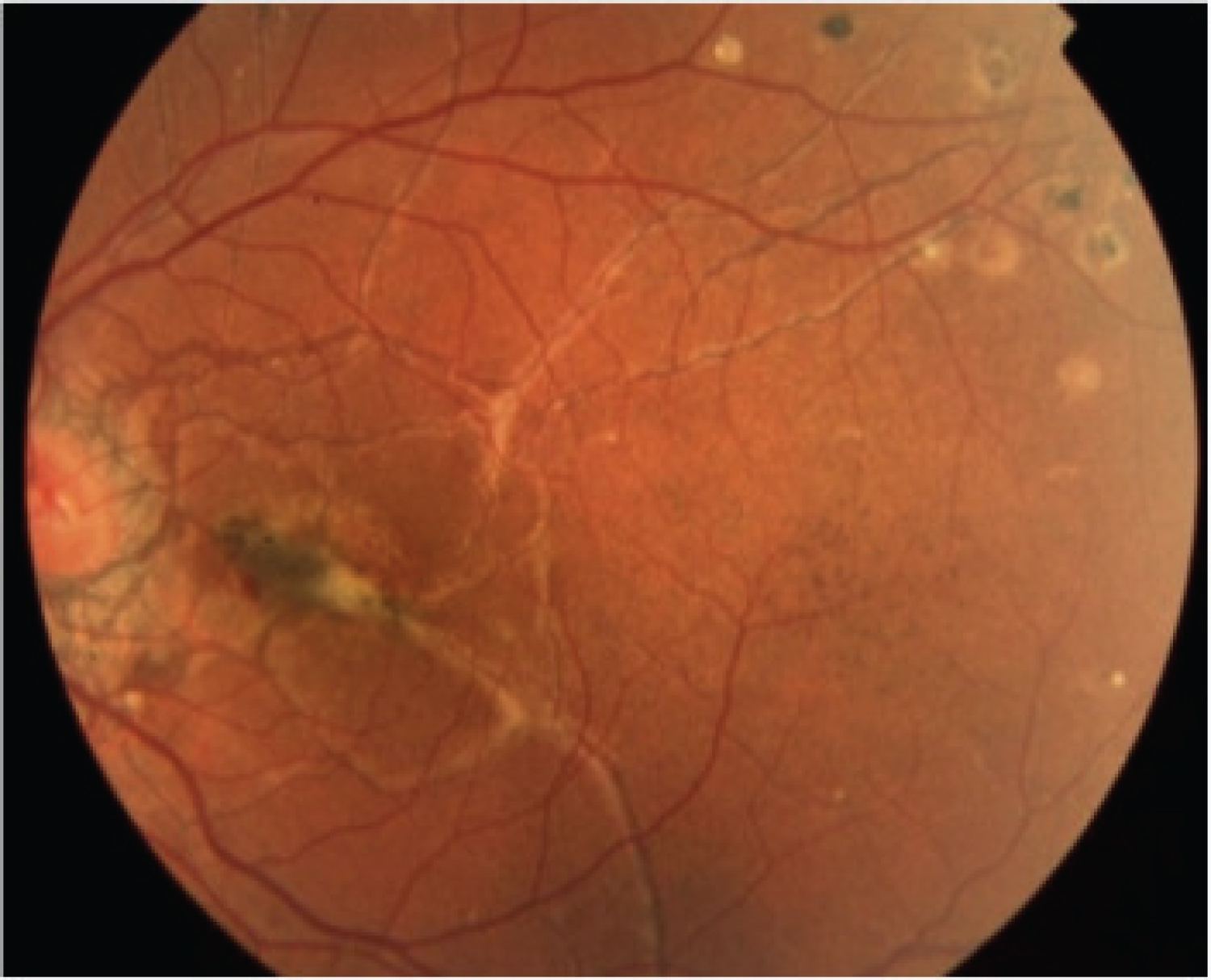 Figure 4: Fluorescein angiography. Note the angiomatous streaks of the eyes.
View Figure 4
Figure 4: Fluorescein angiography. Note the angiomatous streaks of the eyes.
View Figure 4
Pseudoxanthoma elasticum (PXE) is a rare genetic disease characterized by damage to connective tissue, mainly affecting the skin, eyes and arterial walls. In 1881, Rigal was the first to describe PXE skin lesions as diffuse xanthelasma. In 1929, ophthalmologist Ester Grönblad and dermatologist James Strandberg independently described the frequent association between skin lesions and angioid striae [3]. This case confirmed this observation. In our patient, the cutaneous involvement was evocative made up of yellowish papules, with an aspect of wrinkled layers in "shagreen skin" by progressive coalescence of the papules, willingly taking on a "draped" aspect according to Mahé [4]. The cutaneous signs in our patient confirmed this assertion (Figure 1a, Figure 1b, Figure 2, Figure 3 and Figure 4). These lesions sometimes pose a major aesthetic problem for patients. Histologically, there is elastorrhexy of the elastic fibers with accumulation of pleomorphic elastic structures in the middle dermis. The presence of calcifications is essential for the definitive diagnosis of PXE. Histological examination of the skin under an optical microscope allows the diagnosis of PXE and the exclusion of differential diagnoses. For this, elastin is stained with the Verhoeff–van Gieson reagent and calcium deposits are revealed during von Kossa or Alizarin red staining. The elastic fibers of the middle dermis are short, fragmented, grouped and calcified. These features are quasi-pathognomonic for PXE. Clumping and calcification of elastic fibers are typically present only in clinically affected skin in ABCC6 homozygotes or composite heterozygotes [5]. The extra cutaneous lesions make all the seriousness of this disease; these are mainly eye damage that can lead to blindness, The ophthalmologic features of PXE mainly include orange peel appearance, comet-tail atrophies, angioid streaks, choroidal neovascularization, retinal hemorrhages, and irreversible retinal atrophic scar formation. Iconic ocular manifestations are angioid streaks, due to thickening and calcification of Bruch's membrane - the deepest and most elastic layer of the retina but also vascular damage with atheromatosis and rupture of arterioles responsible for bleeding [5]. In our patient, it was ocular vascular damage such as ocular angioid streaks which are frequent, but not specific: indeed, such lesions are encountered during sickle cell disease according to Alabi, et al. [6]. Vascular occlusion accidents should also be feared [5]. The cardiologist is thus an essential player in the usual clinical monitoring; Regarding drug treatment, a study of 1747 patients with PXE showed that one-third were taking or had taken cholesterol-lowering agents. Statin treatment could be discussed in case of associated cardiovascular risk factors in a patient with PXE but has not been specifically validated. our patient underwent a clinical and paraclinical examination (cardiac echo-Doppler). The differential diagnoses arise with dermal elastolysis or white cervical papulosis due to a focal disappearance of the elastic fibers of the superficial dermis without elastorrhexy; PXE also differs with citrein skin of the neck, which is an actinic elastosis of the elderly subject; it will also occur with exogenous PXEs where the elastic fibers are altered by contact with a chemical product [1,7]. It is important to note that skin lesions may be absent in a few very rare cases, with cardiovascular damage dominating the clinical picture [8].
In Morocco, the delay in the consultation is very frequent and the patients come to a stage of complications. From a dermatological therapeutic point of view, plastic surgery is not indicated because of the extent of the lesions and the fact that there is no psychological impact in our patient. The only global prognostic data available are those provided by McKusick who put forward the figure of 50% mortality due to the disease before the age of 50 [9]. The prognosis is therefore favorable in this 62-year-old patient.
PXE requires a multidisciplinary approach for genetic counseling, for the management of proven lesions and for surveillance associated with self-monitoring of vascular complications. No specific treatment is available to date.
The authors declare no conflict of interest.
All authors contributed to this work and read and approved the final version of the manuscript.