Pruritus is a common dermatological condition which may have systemic etiology. Diabetes is one such condition; pruritus is commonly seen in patients with diabetes thus making it a dermatometabolic condition. The present survey aimed to understand the knowledge, attitude, and practice toward pruritus among Indian physicians and patients living with diabetes presenting with pruritus.
A telephonic, cross-sectional, quantitative survey was conducted among consulting physicians (CPs), endocrinologists, and patients across 12 cities in India from October-November 2020. Interviews were conducted using a structured questionnaire and lasted approximately 30 minutes. The collected data was analyzed by simple proportions using descriptive statistics.
Overall, of all the patients treated by physicians, majority of the patients had diabetes and diabetes associated pruritis. Majority CPs and endocrinologist reported redness as the primary sign of pruritus. Overall, most of the physicians recommended for diagnosing pruritus and reported diabetes was the dominant etiology for pruritus and that it affected the quality of life of the patients. Physicians preferred a combination of topical and oral medication as treatment. Majority patients believed that there is a strong association between diabetes and pruritus and emphasized on the importance of counseling. Few patients were recommended treatment for pruritus while most of the patients resorted to self-medication. Some of the physicians preferred proactive and reactive treatment approach for pruritus management, however majority perceived that pruritus is not a major clinical problem for the persons living with diabetes.
The survey concluded that Indian physicians considered diabetes, environmental factors, and stress as the major causes of diabetes associated pruritus, they preferred using diagnostic tests and treatments providing symptomatic benefits. There are a large proportion of persons living with diabetes who choose to self-medicate and need adequate counseling and awareness regarding pruritus as it is a serious dermatometabolic condition.
Quantitative research, Knowledge, Attitude, Physician, Person centered care, Diabetes, Pruritus
CP: Consulting Physician; MD: Doctor of Medicine (physician); DM: Doctor of Medicine (endocrinology); ICMR: Indian Council of Medical Research; HbA1C: Hemoglobin A1c; CKD: Chronic Kidney Disease
Pruritus or itching is a commonly occurring skin condition characterized by an unpleasant sensation of skin which arouses the desire to scratch [1]. The pathophysiology of pruritus can be understood through peripheral mechanisms such as physical stimuli, neural pathways, and chemical mediators or through central mechanisms. Based on anatomical, pathophysiological, and psychological factors, pruritus can be classified into four clinical categories neurogenic, psychogenic, neuropathic, and pruritoceptive [2]. Pruritus is classified on the basis of origin as localized or generalized and as acute (lasting for shorter period) and chronic (lasting for six or more weeks) based on duration of symptoms [3].
Pruritus may have systemic and dermatologic etiology with underlying conditions ranging from endocrine and metabolic diseases, neoplastic and hematological, systemic conditions to inflammatory, genetic, infectious or autoimmune, dermatological disorders [4]. Notably a high proportion of patients presenting with pruritus have an underlying systemic condition [5], so ascertaining the etiology of pruritus is imperative to ensure correct clinical course of action.
Diabetes mellitus is a common endocrine disorder, its underlying pathophysiology predisposes patients to develop impaired skin elasticity and decreased cutaneous sebaceous gland activity leading to cutaneous complications including pruritus [6,7]. Further, in patients with elevated blood glucose there is an increase of advanced glycosylated products in the collagen of the dermis leading to pruritus [6]. Globally, 18.4‑27.5% diabetes patients present with pruritus [8-11]. An Indian cross-sectional study conducted in a tertiary care hospital, reported that 13.3% of the diabetes patients had pruritus without skin lesions. Diabetes patients may present with localized or generalized pruritus, however localized pruritus (scalp, ankles, feet, trunk, or genitalia) is more common [7,9,12].
Current management approach for pruritus includes therapies providing symptomatic relief, such as emollients, topical anti-pruritic agents such as calamine, menthol, capsaicin, corticosteroids, calcineurin inhibitors, local anesthetics, and systemic antipruritic agents such as H1 antihistamines, doxepin, and gabapentin [7]. Broad-band or narrow band ultraviolet B phototherapy can be used to treat generalized chronic pruritus of any cause [13]. Minimizing scratching and other traumas to involved areas can allow lesions to resolve over a period of months. Individual lesions can be managed with topical agents such as keratolytic, retinoids or high-potency steroids [7]. Apart from these agents, lifestyle modifications including physical activity, nutrition therapy, personal hygiene is also recommended [14].
Due to the unawareness in patients, lack of standardized testing and treatments for pruritus [15], patients often have to suffer with the condition. The current treatments for pruritus are largely symptomatic and patients suffering from chronic pruritus do not get a prudent solution [16]. Further due to the multifaceted effects of pruritus patients suffer from various psychological (anxiety, depressive disorders) and social (low self-confidence, social timidity) implications [17,18]. Further currently, there are no global and Indian standard treatment protocols or guidelines for treating diabetes patients presenting with pruritus, thus leading to inconsistencies in the treatment approach [19,20].
The present quantitative survey was conducted to assess knowledge, attitude and practice among consulting physicians (CPs), endocrinologists and persons living with diabetes in India to understand their current level of knowledge, practice approaches and need gaps in management of pruritus associated with diabetes.
A cross-sectional, multicenter, quantitative survey was conducted from October-November 2020 in 12 cities (Delhi, Jaipur, Lucknow, Kolkata, Patna, Bhubaneshwar, Mumbai, Pune, Ahmedabad, Bangalore, Hyderabad, and Chennai) across the four zones of India. The survey included a total of 300 doctors (180 CPs and 120 endocrinologists) and 300 patients. The participants for the study (CP, endocrinologist, patients) were identified using the IQVIA OneKey®. The participants were selected for the study based on predefined screening criteria. The inclusion criteria for the CPs and endocrinologists were-Doctor of Medicine (MD) physician/ Doctor of Medicine (DM) Endocrinology treating diabetes, practicing for more than 10 years, and treating more than 100 patients per month. The inclusion criteria for the patient were male or female patient aged between 18-65 years with diabetes for more than five years, having pruritus or itch and with other itch-producing diseases ruled out.
The survey was conducted in accordance with the requirements of ICH E6 (R2) 'Guideline for Good Clinical Practice, ICMR Guidelines (2017) as applicable for the conduct of surveys. It was approved by Conscience Independent Ethics Committee, Ahmedabad, and Gujrat, India. The survey conduct followed the Market Research Society's Code of Conduct. A verbal consent was obtained from the CPs, endocrinologists, and patients prior to conducting the interview. All personal data of the patients including identification was considered confidential and was not collected for the study. Results of the study were made available for review by authorized representatives of Sponsor and the ethics committee. All communications relating to participants identified each participant by their unique identification number only. The participants were compensated for their time in accordance with the Market Research Society of India [21] and IQVIA standard practices.
One on one structured interviews were conducted by a representative of the contract research organization IQVIA with CPs, endocrinologists, and patients. The survey was carried out through an online survey platform. The interview duration was approximately 30 minutes. The questionnaire used for the survey was developed based on the findings from qualitative phase of the study. The questionnaire was validated by subject matter experts and updated as per their suggestions. The questionnaire included direct questions (single response and multiple response questions) and questions with a scaled response i.e. a scale of 1 to 5 where the scales were defined as per the specific question. The questionnaires are provided in the supplementary material.
The CPs and endocrinologists were enquired regarding their practice settings, knowledge around pruritus associated diabetes, attitude toward management of pruritus associated diabetes and management of pruritus. The patients were enquired about their current knowledge with respect to pruritus associated with diabetes, their seriousness perception around pruritus associated with diabetes and their journey from the time they were diagnosed until their condition was managed.
The responses from the participants were scrutinized, and 30% responses were back checked. The collected data was analyzed by simple proportions, using descriptive statistics including frequency, proportion, and percentage. The identified themes were divided on the basis of knowledge, attitude and practice, and challenges related to pruritus associated with diabetes for physicians and patients respectively.
A total of 300 physicians (CP and endocrinologists) including 180 CPs and 120 endocrinologists were included in the survey. Overall, the CPs and endocrinologists treated around 517 patients per month with significantly higher patient load seen by CP (544 patients) than endocrinologists (476 patients). Overall, 65% (n = 336) patients had diabetes, amongst the patients with diabetes, 14% (n = 46) patients had pruritus. However, only 58% of the patients (n = 27) were recommended treatment for pruritus, of which 49% (n = 13) were adherent to the treatment (Table 1).
Table 1: Average total number of patient seen by physician in a month. View Table 1
Overall majority of the patients were follow up patients 64% (n = 215), endocrinologists had 68% (n = 304) follow up patients as compared to CP with 61% (n = 149) follow up patients. Overall majority of the patients were directly approached physicians 63% (n = 212) and 37% (n = 124) were referred patients. Among endocrinologists and CP, CP had more direct patients 65% (n = 159) and 59% (n = 264) respectively. Majority of the patients referred to endocrinologists came from dermatologists 48% (n = 58), followed by CPs 32% (n = 38) patients. Endocrinologists referred majority of the patients 50% (n = 16) to dermatologists. The CPs treated 73% (n = 131) patients for pruritus themselves and referred 27% (n = 49) patients to other specialties, with highest proportion referred to dermatologists 54% (n = 26) followed by endocrinologists 17% (n = 8).
Symptoms and frequency of symptoms in diabetes patients with pruritus: Overall, 35% (n = 105) and 54% (n = 162) persons living with diabetes had skin complaints once a month and twice a month respectively. According to the surveyed physicians the persons living with diabetes had a range of dermatological conditions primarily dry red itchy patches 86% (n = 258), followed by dry scaly thick plaques that are not itchy 61% (n = 183), and itching redness blisters swelling and scabbing 56% (n = 168). Additionally, the major presentation (or sign) were redness 88% (n = 264) and dry cracked skin 70% (n = 210) typically experienced by most patient twice a month 47% (n = 141). Majority of the CPs 89% (n = 160) and endocrinologist 85% (n = 102) reported redness as the primary presentation of pruritus (Figure 1).
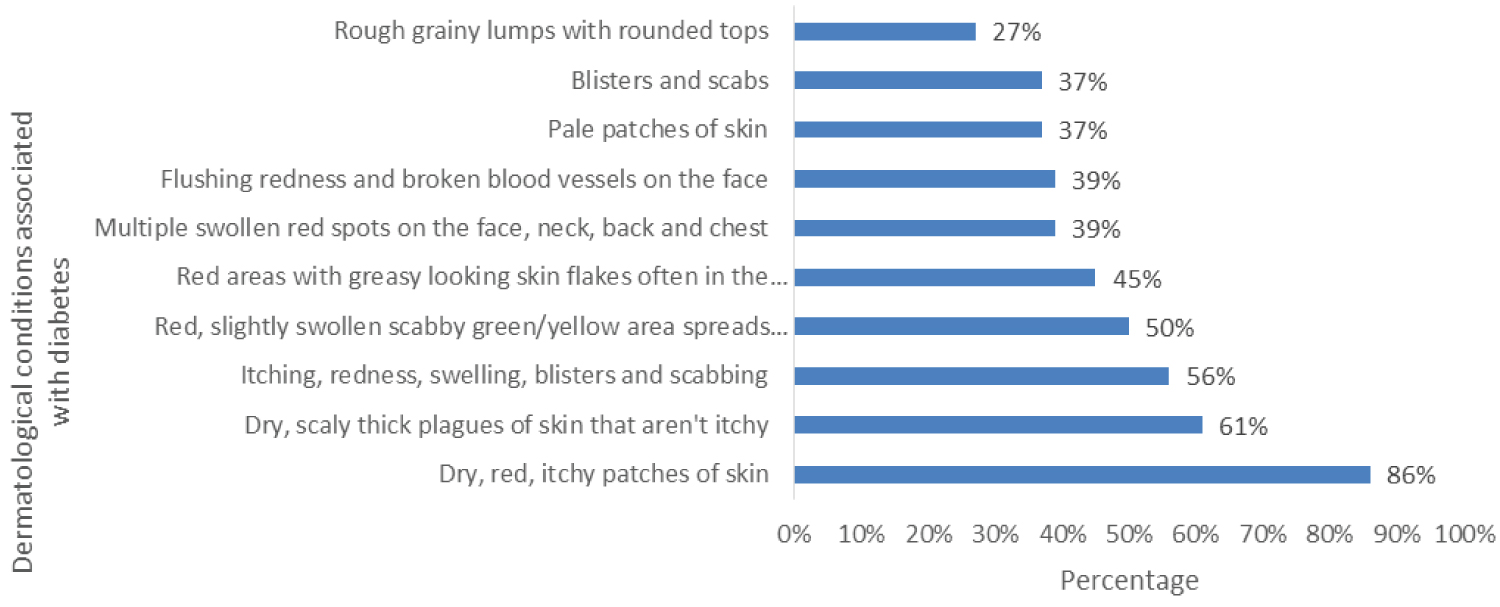 Figure 1: Symptoms and frequency of symptoms in diabetes patients with pruritus. The primary representation was the redness and itchy patches of skin reported by maximum patients.
View Figure 1
Figure 1: Symptoms and frequency of symptoms in diabetes patients with pruritus. The primary representation was the redness and itchy patches of skin reported by maximum patients.
View Figure 1
Classification of diabetes patients with pruritus: Based on the classification of the pruritus, acute 46% (n = 112) and chronic 54% (n = 131) pruritus are the two main types pruritus observed in persons living with diabetes. Local or systemic pruritus and pruritus because of infections was observed in 66% (n = 198) and 65% (n = 195) persons living with diabetes in physicians' clinical practice.
Diagnostic test for pruritus: Overall, 71% (n = 213) physicians recommended diagnostic tests for diagnosing pruritus'. Similar trend was observed in CP and endocrinologist where 70% (n = 126) and 74% (n = 88) respectively, preferred diagnostic test over clinical examination. Complete blood count emerged out to be the most common test and was recommended by 92% (n = 196) of the physicians followed by serum creatinine 65% (n = 138) and liver 63% (n = 134) and renal function test 63% (n = 134) (Figure 2).
 Figure 2: Diagnostic tests recommended by physicians in clinical practice for diagnosing pruritis. These tests were preferred over clinical examination with complete blood count being the most common test.
View Figure 2
Figure 2: Diagnostic tests recommended by physicians in clinical practice for diagnosing pruritis. These tests were preferred over clinical examination with complete blood count being the most common test.
View Figure 2
Etiology of pruritus in diabetes patients: Concerning the causation of pruritus in persons living with diabetes, overall, 83% (n = 249) physicians stated diabetes to be the major reason for pruritus followed by infections related to diabetes 51% (n = 153) and environmental factors 38% (n = 114). Approximately 90% physicians agree that stress, diabetes, and environmental factors act as major etiological factors for pruritus.
Ninety-one % (n = 109) endocrinologists stated diabetes was the cause for pruritus followed by infections related to diabetes 89% (n = 107) and stress 88% (n = 106). The CP considered environmental factors (83%), stress (79%) and diabetes (78%) to be the primary etiological factors.
Extent of association of diabetes with pruritus among patients: Eighty-eight % (n = 261) physicians perceived that bringing the patient's glycemic levels under control would resolve pruritus and 87% (n = 258) physicians perceived reduction in pruritus symptoms as a sign of controlled diabetes. A few physicians stated that there are certain other conditions for patient developing acute and chronic pruritus apart from diabetes such as renal disorders (67% [n = 201] and drug allergies (56% [n = 168]).
Comorbidities in diabetes patients with pruritus: Majority of the physicians stated that patient having pruritus also have other comorbidities such as metabolic syndrome 75% (n = 225), hypertension 59% (n = 177), and renal disorders like chronic kidney disease 52% (n = 156) (Figure 3).
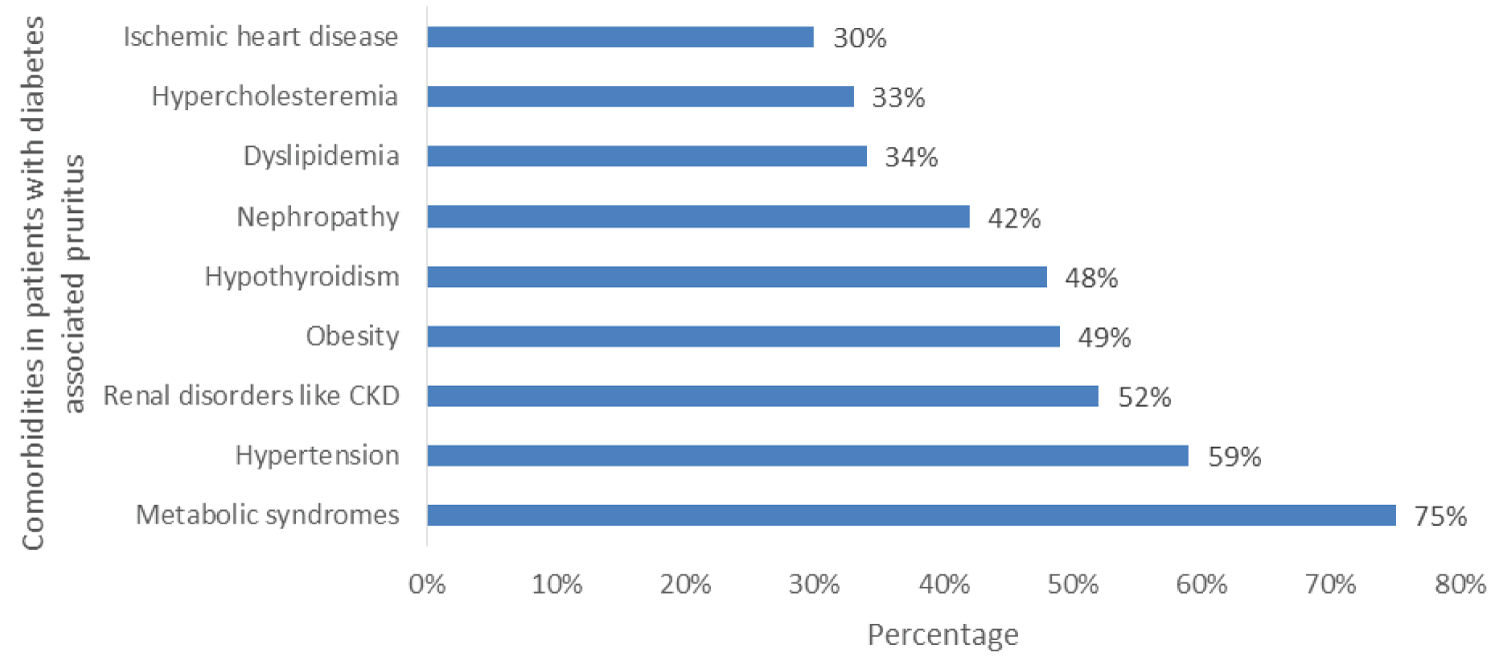 Figure 3: The diabetes patients with prurities have different comorbidities with metabolic syndrome being the most common comorbidity.
View Figure 3
Figure 3: The diabetes patients with prurities have different comorbidities with metabolic syndrome being the most common comorbidity.
View Figure 3
Perception of severity regarding pruritus: Overall, 69% (n = 207) stated pruritus to be slightly more severe than common alignments or conditions such as acute fever 37% (n = 111), weakness (n = 174), cough and cold 33% (n = 99). The physicians also reported that pruritus causes a higher amount of physical discomfort and hinders patient from carrying on their day to day activities. Additionally, common aliments like cough cold or fever may be seasonal or acute in nature while pruritus may be acute or chronic in nature.
Treatment approach toward diabetes patients with pruritus: Overall, 62% (n = 186) physicians reported that they preferred to focus on treating the underlying condition as well as pruritus (slightly higher in among endocrinologists 67% [n = 80]). Overall, 46% (n = 138) and 45% (n = 135) physicians preferred proactive and reactive treatment approach for pruritus management.
Impact on Quality of life and counseling: Overall, 83% (n = 249) physicians and 90% (n = 108) endocrinologists stated that pruritus affects the quality of life of the patients. The need to counsel the patient about pruritus was emphasized by 91% (n = 273) physicians, 88% (n = 158) CP and 96% (n = 115) endocrinologists. Overall, 85% (n = 255) physicians reported counseling to be important and very important, 80% (n = 144) CP and 94% (n = 112) endocrinologists considered counseling to be important and very important. Overall majority 64% (n = 192) of the physicians believed that counseling should be recommended once the patient is diagnosed with diabetes. Mostly, the treating physician was considered most suitable as the counselor 48% (n = 144) followed by diabetes educator 29% (n = 87) and patient support programs 9% (n = 27). Relatively higher preference toward counseling by the treating physician was given by the CP 52% (n = 94) compared to endocrinologist 42% (n = 50). While more endocrinologists preferred diabetes educators as the counselor 37% (n = 44) as compared to CP 24% (n = 43).
Factors considered while choosing treatment regime: The initiation of treatment is based on various factors including age 83% (n = 249), severity of pruritus 61% (n = 183), comorbidities 59% (n = 177). Other vital parameters include HbA1C level, creatinine, complete blood count, duration, and site of pruritus (Figure 4).
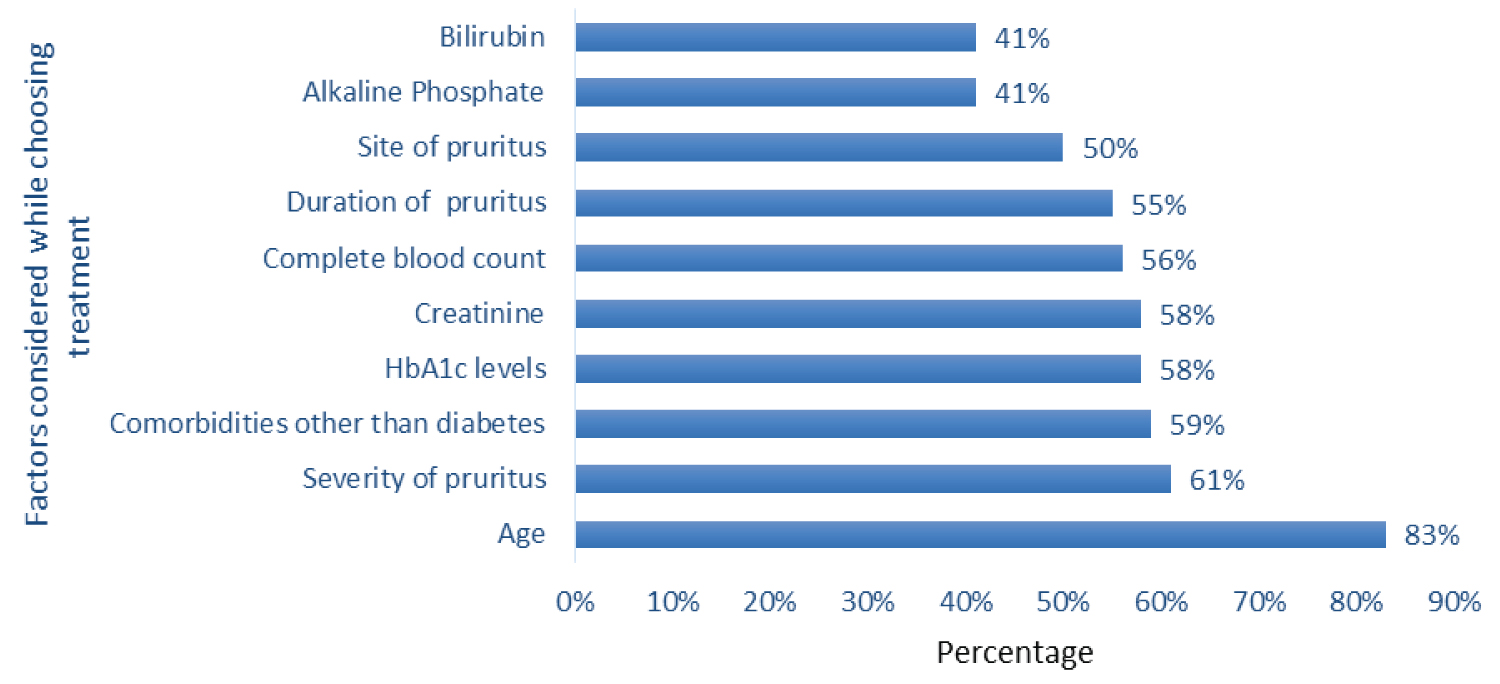 Figure 4: The different factors are considered while choosing treatment regime or for the initiation of treatment where age is the primary factor.
View Figure 4
Figure 4: The different factors are considered while choosing treatment regime or for the initiation of treatment where age is the primary factor.
View Figure 4
Treatment and duration of treatment: Physicians preferred a combination of topical and oral medication for the treatment of diabetes patients with pruritus, as the first line 25% (n = 75) and second line 29% (n = 87) treatment respectively.
CPs preferred a combination of topical and oral medication (first line 28% [n = 50] and second line 32% [n = 58]) while the endocrinologists preferred topical treatment alone (first line 27% [n = 32] and second line 20% [n = 24]) for diabetes patients with pruritus. Physicians usually prescribed emollients and antihistamines as first line therapy for four weeks and two weeks for their patient respectively, 4.5 weeks of emollient and 3.5 weeks of antihistamines as second line therapy and emollients for more than one and half month and around one month of antihistamines as third line therapy. Majority the patient continued the usage of topical emollients beyond prescribed duration 84% (n = 245) (Table 2).
Table 2: Physician reported various treatment options for management of diabetes associated pruritus. View Table 2
Physician's satisfaction with current treatment: Overall, majority of the physician 76% (n = 228) with relatively higher proportion of endocrinologist 87% (n = 104) were satisfied with the currently available treatment option. Majority of the physicians (79% [n = 237]) were satisfied with the knowledge imparted during continuous medical education while 74% (n = 222) suggested lack of focus on pruritus associated to diabetes.
Challenges faced while managing diabetes patients with pruritus: The major challenges encountered by the physicians while managing the patient with pruritus included lack of clear diagnostic test for pruritus 72% (n = 216), high cost of treatment 60% (n = 180) and lack of patient compliance to treatment 56% (n = 168) (Table 3).
Table 3: Challenges faced by physician and patient while managing/treating diabetes associated pruritus. View Table 3
Focus on diabetes associated pruritus and future scope: There are few reasons attributable to the lack of focus in diabetes associated pruritus including physicians belief that pruritus can be managed easily without specific treatment by just controlling glycemic levels 65% (n = 144), pruritus being managed by specialties including dermatologists 62% (n = 138) and the perception that pruritus is not a major clinical problem for the persons living with diabetes 59% (n = 131). The physicians stated that according to them increasing awareness for early diagnosis 73% (n = 219), prioritizing counseling 66% (n = 198) and educating the primary physicians treating persons living with diabetes 51% (n = 153) can help with better management of diabetes associated pruritus in future.
Majority of the persons living with diabetes (n = 300) were suffering from pruritus as a concomitant condition from past three years. A total of 61% (n = 184) of the persons living with diabetes upon experiencing pruritus or itching reached out to allopathic doctor (General/Family physician 57% (n = 105), CP 24% (n = 44) and diabetologist/endocrinologist 16% [n = 29]). Sixteen% (n = 48) of the persons living with diabetes tried home remedies while 6% (n = 18) persons living with diabetes self-medicated. The average duration suffered by the persons living with diabetes were three weeks with around 42% (n = 126) persons living with diabetes experiencing it for 1-2 weeks and 34% (n = 102) experiencing for 3-4 weeks. The average time gap in reaching the current treating specialty was five weeks.
Currently 64% (n = 130) of the persons living with diabetes are being treated by the same doctor. The trigger to change to the treating physician included increase in symptoms 69% (n = 127), non-responsiveness from past treatment on Ayurveda/homeopathy 52% (n = 96) and no reduction in symptoms on self-medication or home remedies 48% (n = 88). General/Family physician 33% (n = 99) formed the majority proportion of the current treating doctor specialty followed by CP 29% (n = 87) and endocrinologist/diabetologist 29% (n = 87) (Figure 5).
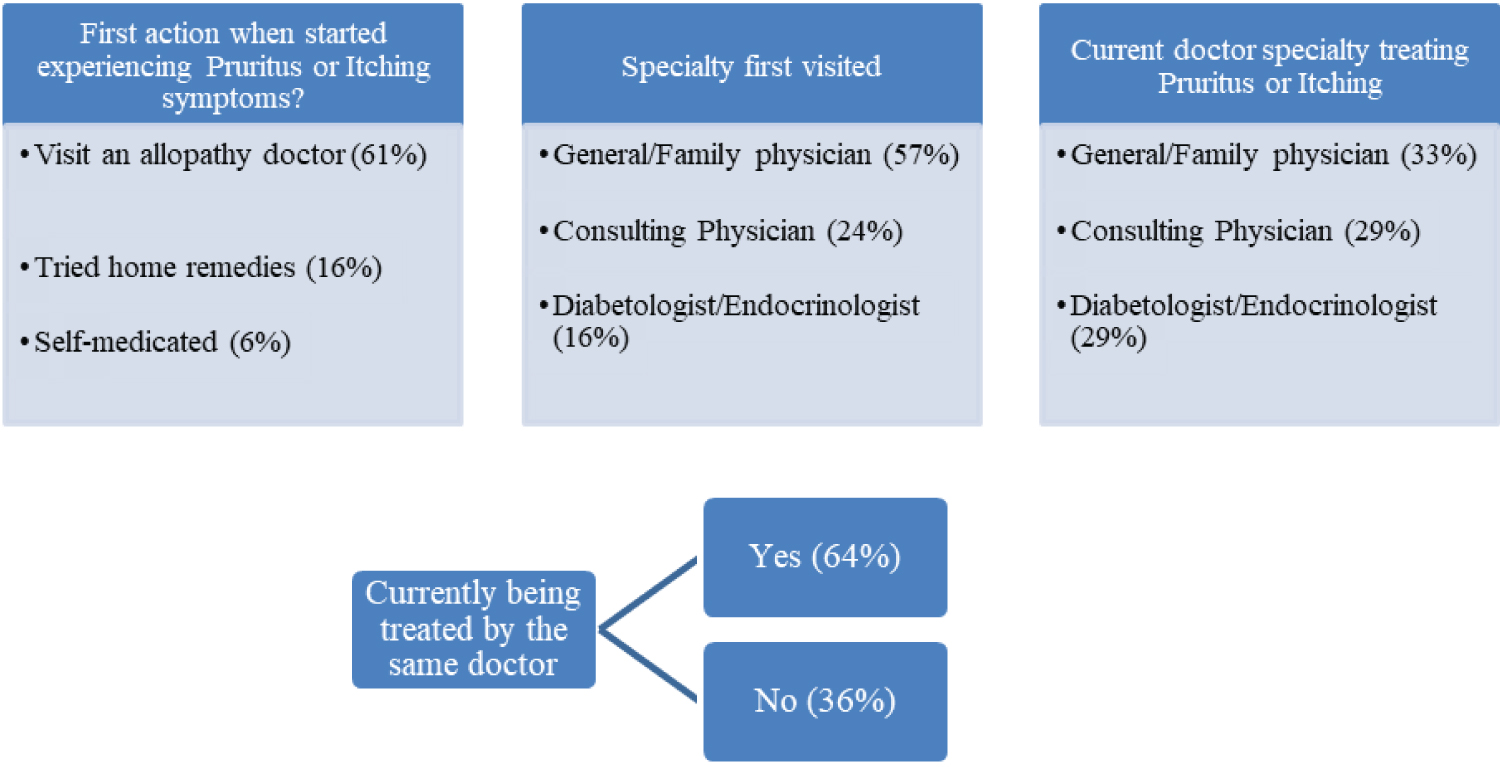 Figure 5: The entire patient journey is represented here emphasizing on the first action taken and first specialty visited.
View Figure 5
Figure 5: The entire patient journey is represented here emphasizing on the first action taken and first specialty visited.
View Figure 5
As reported by the patients the skin conditions that are commonly seen among persons living with diabetes associated pruritus (n = 184) were redness 84% (n = 155), dry cracked skin 64% (n = 118), and bumps, spots, or blisters 49% (n = 90). Overall, 53% (n = 159) of the persons living with diabetes were aware of reasons for itch prior to visiting physicians.
Patients mentioned that physicians said that diabetes was the major reason for itch and other symptoms for pruritus. 80% of the patients mentioned that their physicians discussed the correlation between diabetes and itching as diabetes associated pruritus after they went through clinical examinations and/or diagnostic tests.
A total of 78% (n = 234) persons living with diabetes believed that there is a strong association between diabetes and pruritus. Eighty-five % (n = 254) of the persons living with diabetes opined that bringing the sugar levels under control would resolve the itching symptoms while 84% (n = 251) considered reduction in itch to be an indication of controlled diabetes.
Overall, of the persons (n=300) living with diabetes associated pruritus, 79% (n = 237), 58% (n = 174), 37% (n = 111) stated the severity of itch, weakness, fever compared to pruritus as severe and extremely severe. Eight-five % (n = 255) of persons living with diabetes emphasized on the importance of counseling. A total of 80% (n = 240) persons living with diabetes reported being counseled for pruritus. There was equal proportion 50% (n = 120) of persons living with diabetes receiving counseling at stage of reporting their symptoms of itching and while being diagnosed with diabetes. The treating physician (45% [n = 70], 48% [n = 143]) and the diabetic educator/counselors at the doctor's clinic (44% [n = 68], 41% [n = 122]) were the preferred and suitable type of counselor respectively.
Medicated creams or ointments prescribed by the physician (61% [n = 183] for 16 weeks), and tablets or capsules (39% [n = 117], antihistamines for 13 weeks) was reported to be the favored current treatment. However, the persons living with diabetes often tend to continue using these medications beyond the duration of prescription (medicated creams or ointments for 17 weeks, antihistamines for 15 weeks). Fifty‑one % (n = 153) of the patients mentioned that they apply creams, moisturizing lotions on their own as self-medication without recommendation or prescription from doctor. Patients tend to use them because of their past experience 45% (n = 68) and because of suggestions from friends/families 47% (n = 71) and the chemist 42% (n = 64). Majority of the persons living with diabetes 85% (n = 255) were satisfied with their current treatment regimen.
Majority the persons living with diabetes faced challenges in managing pruritus including fear of increased symptoms 61% (n = 183), recurrence of symptom 60% (n = 180), negative impact on family life 58% (n = 174) and societal embarrassment 57% (n = 171).
Diabetes is a chronic disease that affects individuals irrespective of their age and socioeconomic status. The rapid socioeconomic development and demographical change in association with an increase in susceptibility has led to increased prevalence of diabetes in India, ultimately causing a rise in its associated clinical manifestations [22]. It has been observed that around thirty to seventy percent of the persons living with diabetes present with cutaneous manifestation, primarily pruritus at least once in their lifetime [7]. It is mainly attributable to the acute metabolic derangements along with chronic degenerative complications of diabetes [23].
Pruritus can be considered as a surrogate marker for uncontrolled and complicated diabetes, associated metabolic conditions [6,8]. In the present survey, the physicians (CP and endocrinologists) reported the 14% (n = 46) patients with diabetes had pruritus. The results were in accordance with previous published literature, both at the global and regional level where the prevalence of cutaneous manifestations and pruritus in persons living with diabetes have been established [10,23-26].
In the current survey, the physicians reported that majority of the persons (63%) living with diabetes tend to approach physicians directly on their own for dermatological issues mostly due to the regular follow ups for diabetes. Based on their condition and dermatological issues, the persons living with diabetes either visit an endocrinologist by themselves or are referred to other specialists by their CPs (54% to dermatologists and 17% to endocrinologists). Most of the physicians (~90%) were aware and stated that poor diabetes control predisposed the persons living with diabetes toward developing pruritus. These findings were in line with prior studies where association between the augmented glucose level in diabetes and development of pruritus has been established [8,11,27].
Research has also demonstrated pruritus or other dermatological manifestations increases as the duration of diabetes increases and is more prevalent in type II diabetes [28]. Thus, controlling diabetes plausibly lead to improvement in pruritus management [29]. Stress (88%) and infections related to diabetes (89%) were also stated as important causes by the surveyed physicians. A previously published study has demonstrated that maintaining personal hygiene is pertinent in improving pruritic condition [17,30,31]. Additionally, stress is linked to pruritus since it affects the immune response of the persons living with diabetes reflecting as a common clinical manifestation in persons living with diabetes with pruritus [31].
Most of the physicians have classified pruritus as acute and chronic in nature which forms the basis of the treatment regimen. The treatment modality primarily relied on symptomatic relief and treating the underlying cause of pruritus, taking on a multifaceted approach. Previously published study also suggested pruritus of the scalp being treated for symptomatic relief in persons living with diabetes [32]. However, the physicians emphasized on the lack of focus on pruritus treatment among persons living with diabetes due to lack of awareness and preference toward lifestyle modifications. The surveyed physicians in the present study took proactive approach 46% (n = 138) in managing pruritus.
The current survey also highlighted the need to strengthen the counseling about pruritus in persons living with diabetes. Since pruritus affects the quality of life of the persons living with diabetes by causing different dermatological conditions that might hinder in day to day activity, hence creating awareness and spreading adequate information is the need of the hour. Although many physicians did not prioritize counseling until the symptoms of pruritus appeared.
Physicians from the current survey reported the unmet need of lack of clear diagnostic test for pruritus, high cost of treatment and lack of patient compliance to treatment. The other key challenge put forth by the physicians is the addition to the existing pill burden causing considerable out of pocket expense, often leading to non-adherence to the stipulated regimen [33,34]. The access to healthcare for persons living with diabetes and economic burden along with social barriers are major challenges for the Indian scenario [35]. The physicians also reflected on the need of unified guidelines for management of diabetes associated pruritus which would help in standardized treatment approach.
One of the major attributes highlighted in the survey was the under treatment of pruritus since only 60% of the persons living with diabetes prefer visiting physicians while rest of them either use home remedies or self-medicate.
This further leads to the aggravation of pruritus. This reflects on the patient's perspective who do not consider pruritus as a serious issue, majorly due to lack of awareness. The persons living with diabetes also confirmed on the adverse impact of pruritus on the quality of life and expressed need for optimal therapeutic approach. The survey findings suggest concordance between knowledge and practice and concordance between what physician said and what persons living with diabetes heard.
Thus, the need for patient centered approach to plan and prescribe treatment in persons living with diabetes associated pruritus is inevitable. Additionally, the physician should be made aware regarding the importance of patient history during the diagnostic process and in the treatment phase. Moreover, the treatment should be for symptomatic relief and also based on etiology of pruritus and adequate attention to the underlying causes will aid in providing a holistic treatment approach. The importance of counseling could not be ruled out since it is vital in creating awareness among the persons living with diabetes.
The current survey was associated with the limitation of not classifying pruritus into infective and non‑infective (fungal and non-fungal). However, this parameter was assessed while assessing the practice parameters. Despite the limitation, this survey was first of its kind where sub-group data for physicians (CP and endocrinologist) was analyzed. Large sample size spread over all four zones of India formed the base for a large-scale analysis. Additionally, comparison between physicians and persons living with diabetes helped identify the need gaps to deduce valuable insights on treating persons living with diabetes having associated pruritus in India.
The survey concluded that Indian physicians considered infections and vascular complications of diabetes along with environmental factors and stress as the major causes of diabetes associated pruritus. Therefore, it is essential to understand the etiology of pruritus and underlying pathomechanism for developing suitable treatment regimen for the persons living with diabetes. Additionally, there is considerable proportion of persons living with diabetes opting for self- medication, thereby highlighting the need of adequate counseling and awareness. The way forward includes patient centered treatment and awareness of treatment options for the physicians to provide effective treatment regimen. Moreover, the awareness is an important requisite in improving the quality of life of the persons living with diabetes having pruritus.
Dr. Amey Mane, Ms. Colette Pinto, Dr. Rahul Rathod, Dr. Roheet Rathod are full‑time employees of Dr. Reddy's Laboratories Pvt Ltd. Dr. Sanjay Kalra has received honoraria for lectures, however not directly related to the current manuscript. Dr. Asit Mittal has no conflict of interest.
The study was funded by Dr. Reddy's Laboratories Pvt Ltd.
The authors acknowledge Yukti Singh, and Mrigna Malhotra from IQVIA, India for their medical writing and editing support.