Fractures of the femur in children are not as common as those of adults but presents significant morbidity when they do occur. Such fractures present in diverse pattern in terms of age, causes, season, treatment and outcome. Presentation and treatment is influenced by age of the patients, locality of practice, available resources and experience of treating surgeons.
To evaluate the pattern of presentation, treatment and outcome of fractures of the femur in children seen in a regional trauma centre in Nigeria with the aim of proffering recommendations.
Data of all cases of femoral fractures in children treated at the trauma centre from 1st January 2007 to 31st December 2011 was evaluated retrospectively from the trauma database which had been developed prospectively. Demographic information of the patients, cause of injury, treatment offered and outcome were extracted and analyzed. Descriptive statistics were generated and presented. Inferences were drawn from the observed results as deemed necessary.
During the period under study, 314 cases of femoral fractures were seen in children constituting (23.5%) of the 1334 fractures of the femur treated in the centre. Males predominated overall but below the age of 5 years the male to female ratio was approximately 1:1. Road traffic crashes (209, 66.6%) and falls from heights (70, 22.3%) including those from fruit trees (32, 10.2%) were the major causes of the fractures especially in children older than 10 years with Mean age (SD) been 11.5 (6.3) years. Below 10 years ground level falls and assaults were the main causes; Mean age (SD) = 5.2 (3.6) years. Most of the fractures were of the closed type (286, 91.1%) whereas open fractures were only 28 (8.9%). Two hundred and two of the cases (64.3%) were treated by non-operative methods while surgery including internal fixation was done for 91 cases (29%), external fixation for 13 cases (4.1%) and amputation in one case. Two hundred and eighty-one of the cases (89.5%) of the fractures had attained significant radiological union at 12 weeks after injury while 282 patients had been discharged from hospitalization as at 6 weeks from admission. Infection was recorded in 8 cases (2.5%), while malunion was recorded in 5 cases (1.6%) and non-union was recorded in one patient.
Femoral fractures in children are not as common as those of adults in the centre. Road traffic crashes and falls from heights including falls from seasonal fruit trees were major causes of femoral fractures in children seen at the centre. Preventive measure should include children road safety advocacy and implementation of policies to reduce the population of out-of-school children so as to reduce risk exposure to causative factors.
Femoral fractures, Children, Presentation, Treatment, Outcome, Nigeria
Fractures of the femur in children are not as common as those in adults but are the most common musculoskeletal injury in children requiring hospitalization [1]. Fractures of the femoral shaft in children often follow fractures of the forearm regarding frequency of occurrence [2]. The cause of femoral fractures in children varies with age; whilst falls from a height of less than 1 meter is the most common mechanism in preschool children, in children aged 4-12 years, accidental injury during sports [3], and falls from trees particularly in parts of Africa and Asia [4-7] are the predominant causes. In adolescent and older children, road traffic crashes remain the predominant cause [8].
The method of management of these injuries varies with age and weight of the child, however available resources, local cultural and socioeconomic factors also influence the choice of treatment [8,9]. Most fractures of the femur in children are managed by non-operative methods but in recent time, there has been a growing trend towards operative fixation with development and improvement in implants designs and methods of fracture fixation. Whatever the choice of treatment, adherence to sound principles as outlined by Dameron, et al. produces acceptable outcome [10]. The principles stipulate that the simplest but effective treatment should be the best treatment, the initial treatment should whenever possible be definitive and the injured limb should be immobilized in a splint until definitive treatment had been instituted. The principles further stipulate that anatomic reduction may not be required for perfect function but alignment must be restored, especially rotational alignment, and shortening may not be a problem since remodeling especially in younger children can correct such deficit.
Splinting by harness, spica, casting and traction (skin or skeletal), are all options of treatment in younger children particularly for those younger than 4 years. However, such options have been considered inappropriate in patients over 4 years [11] for reasons of associated complications. Because of the prolonged period of immobilization required for non-operative management in older children, management now trends towards surgery which allows for shorter hospital stay, earlier return of function and reduced impact on modern family life. Other complications of non-operative treatment include the risk of pressure sores with skin traction, whereas skeletal traction may carry the risk of damaging the proximal tibial [12] or distal femoral physes [13] and pin track infection which may progress to pin track osteomyelitis. Limb shortening remains an issue with spica casting [14]. However, some shortening may be desirable to accommodate for the overgrowth often seen in the injured limb [15].
Operative treatments of fractures of the femur in children include intramedullary nailing, use of flexible (Elastic) nails, plate and screws, and external fixators. The use of anterograde intramedullary nailing and elastic nails for unstable diaphyseal fractures remain controversial because of issues of safety of the growing bone and availability of these fixation implants in resource-scarce regions which often reduces the use of these implants in the region [11]. The choice of plates and screws (platting) for femoral fractures in children which was traditionally reserved for polytrauma patients especially in older children, or for stabilizing fractures too proximal to manage with intramedullary nails [11] has been growing due to reports of complications with the use of other treatment modalities.
Open femoral fractures are usually uncommon in children, but when it occurs, it often results from high-energy trauma and is often associated with various degrees of soft tissue injury [16]. Management of open fractures of the femur in children requires early collaboration between orthopedics and plastic surgeons [17]. In fractures with extensive soft-tissue injury, external fixation remains the standard in the management irrespective of the age of the patient [18]. External fixation, can lead to longer union times when compared to elastic nailing or plating. Union of femoral fractures treated with external fixation takes a minimum of 8 weeks [18,19] which may be related to the nature of the associated soft tissue injury. Because of the risks of re-fracture or loss of alignment following earlier removal of the external fixator, leaving the external fixator for up to 12 weeks has been recommended [20].
Fractures of the femur in children, unlike those in the adult femur, has a high healing and remodeling capacity as such angulations up to 25 degrees in any plane can be tolerated [21], but rotational deformity however, is less well tolerated [22]. There is often overgrowth in the injured limb due to a stimulated response from the vessel-rich periosteum. As such. shortening of up to 2-3 cm of the injured limb, especially in those under the age of 10 years, can be accepted [1].
This study aims to evaluate the cases of fractures of the femur in children treated at the regional trauma centre as to determine the pattern of presentation, treatment given and outcome with the view of making recommendations where necessary.
Following Ethical Committee approval according to Helsinki Declaration 1975 and revised in 2000 from the authorities of International Centre for Advanced Medical Care and Development (ICAMCAD), the developers of the Registry, data of subsets of patients younger than 18 years that presented with fractures of the femur at a regional trauma centre in Port Harcourt Nigeria from 1st January 2007 to 31st December 2011 was retrospectively analyzed. Data of patients older than 18 years, patients that were transferred to other centers for reasons of advanced medical care which was not available at the center, and patients that died before resuscitation and treatment was commenced were excluded. Since there was no direct interaction with the patients, informed consent from the patients was waived. However, confidentiality of the patients' information was maintained throughout the study.
Information relating to age, gender, the cause of injury, location, type of fracture, fracture pattern, type of treatment received and outcome of treatment were analyzed. Other variables assessed included postoperative complications; the lengths of hospitalization and the duration to return to full function characterized by fracture union evidenced clinically by the absence of pain at fracture site, good radiological union and return to pre-injury activities. Since the trauma centre was jointly run with an international non-for profit, non-governmental organization, treatment of all patients at the centre was free-of-charge to the patient. Therefore, the cost of care did not influence the choice of treatment for the fracture but was influenced by the hospital policy at any particular time based on the available resources (material and skill) for the specific type of definitive treatment at any material time. Children younger than two years were treated by immediate splinting with harness, spica casting, long leg cast and Gallow's traction as considered necessary while children older than two years with displaced fractures were treated by skin traction and skeletal traction which was later converted to casting. Internal fixation with intramedullary nailing, plating were utilized for older children particularly those older than 12 years. External fixation was reserved for open fractures with extensive soft tissue injuries. Such open fractures were classified using Gustilo and Anderson classification [23] while the degree of contamination was classified using Altemeier wound contamination classification [24].
The outcome of treatment was assessed by the duration of hospital stay, duration to fracture union, complications of treatment such as post-treatment infection, inappropriate fracture union which included malunion and non-union, implant failure, and functional status at 24 weeks post definitive treatment.
Obtained data were analyzed using statistical package for Windows version 20 (IBM SPSS Statistics for Windows, Version 20.0. IBM Corp. Amok, NY). Descriptive statistics were generated and presented as considered appropriate and inferential statistics provided when necessary. Categorical variables were presented as proportions and percentages and numerical variables were presented as means and standard deviation (SD) and median with inter-quartile ranges (IQR) as considered appropriate. Chi-Square χ2 was used to test for observed differences among categorical variables whereas student's t-test was used to compare means between two groups, while one way analysis of variance (ANOVA) was used to compare means in multiple groups as considered necessary. P values less than 0.05 were accepted as statistical significant.
The result shows that during the period under study, 314 cases of femoral fractures in children (23.5%) were amongst the 1334 cases of fractures involving the femur treated in the facility. The age distribution shows that nine fractures (2.9%) were in children less than six months. The highest incidence, 103 cases (32.8%) occurred in children between the ages of 1 and five years while children between 11 years and 15 years and those between 15 and 18 years contributed equally 59 cases (18.8%). The mean age of the patients ± standard deviation (SD) was 8.9 ± 5.5 years, while the male to female ratio (M:F) was 1.8:1.
The cause of injury showed that Road traffic crash (RTC) was the highest contributor of the cases (209, 66.6%) particularly motor vehicle crashes (125, 39.8%) and motorcycle crashes (81, 25.8%) especially in the older children (mean age ± SD = 11.4 ± 6.5 years). Ten fractures (3.2%) resulted from gunshot injuries (GSI) while 90 fractures (28.7%) resulted from falls, mainly falls from height (70, 22.7%) in older children (mean age ± SD = 11.7 ± 6.1 years), whereas 20 fractures (6.4%) resulted in ground level falls in younger children with the mean age ± SD 4.8 ± 3.3 years. There was a statistically significant difference in the cause of fracture between persons older than ten years and those younger than ten years (P < 0.0001). The mean age ± SD of patients with fractures that resulted from RTC, GSI and falls from heights was (11.5 ± 6.3 years) as compared to the mean age ± SD of patients with fractures that resulted from ground level falls, assaults and birth trauma (5.2 ± 3.2 years), t-test = 4.9261; P < 0.0001. Thirty-two patients (10.2%) amongst those that fell from heights fell from fruit trees.
Most of the fractures were closed fractures 286 (91.1%), while the combined open fractures were 28 (8.9%). Amongst the open fractures type I open fractures were 10 (3.2%) while there was one (0.3%) type IIIC, Figure 1.
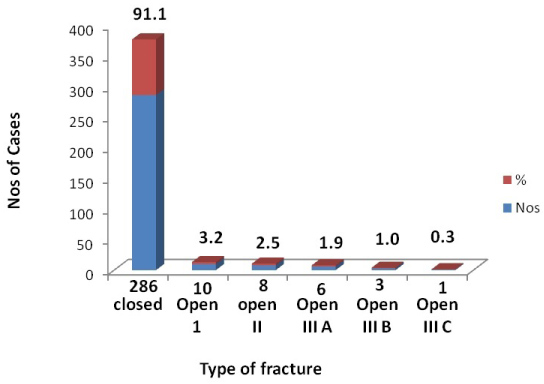 Figure 1: Types of fracture.
Figure 1: Types of fracture.
χ2 = 987.048; P-value < 0.00001.
View Figure 1
Classification of the associated soft tissue wounds of the open fractures using Altemeier wound contamination classification, showed that 10 cases (3.2%) were contaminated, 16 cases (5.1%) were dirty, and 2 (0.6%) cases were outrightly infected on arrival. Figure 2.
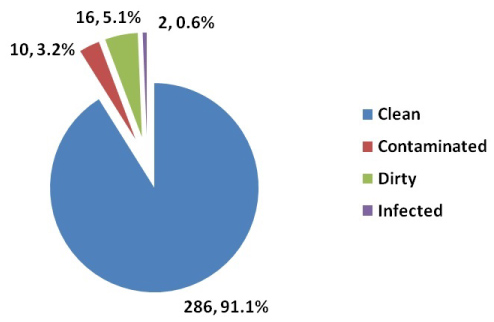 Figure 2: Classification of soft tissue wounds (Altemeier wound contamination classification).
View Figure 2
Figure 2: Classification of soft tissue wounds (Altemeier wound contamination classification).
View Figure 2
Assessment of the fractures geometry showed that most of the fractures (266, 84.7%) were transverse and short oblique fractures, whereas 21 fractures (6.7%) were comminuted. The right side (178, 56.7%) was significantly more involved than the left side (136, 43.3%), P = 0.018.
One hundred and fourteen cases (36.3%) were treated by casting with POP, whereas 91 cases (29%) were treated by open reduction and internal fixation. Thirteen cases (4.1%) were treated by external fixation while one case was treated by amputation. Some of the fractures of the neck of femur and those involving the distal femur particularly epiphyeal fractures Salter-Harris types 2 and type 3 and condylar fractures in older children were treated with screws only while other fractures of the distal femur including condylar, supra-condylar and epiphyseal fractures of the distal femur were treated with percutaneous pins (K-wires). Some undisplaced fractures such as Torus, greenstick and unicorticular fractures were treated by bed rest, braces and splints (Table 1).
Table 1: Definitive treatment given. View Table 1
Following treatment, 70 patients (22.3%) were discharged from the hospital within one week of admission while 162 patients (51.6%) were hospitalized between 2 weeks and six weeks. Seven patients (2.2%) of the patients were hospitalized for a period longer than 12 weeks, and 282 patients (89.8%) of the patients had been discharged from admission as at 6 weeks following admission. This proportion was statistically significant, P < 0.00001. On the duration to radiological union, 281 of the fractures (89.5%) had shown radiological evidence of fracture union while four (1.3%) of the fractures were yet to show evidence of union on radiography. Six cases were lost to follow-up following treatment; Table 2. Infections following treatment were observed in 8 cases (2.5%), Non-union and malunion were recorded in 1 (0.3%) and 5 (1.6%) cases respectively, Table 3. When the recorded infections were related to the type of fracture, it was observed that 2 cases amongst the closed fractures became infected giving an infection rate of 0.7% whereas types III-A and IIIB open fractures had infection rates of 50% and 33% respectively. The observed infection rates for the various types of fractures were statistically significant, P < 0.00005 (Table 4).
Table 2: Time from definitive treatment to radiological union. View Table 2
Table 3: Complications recorded. View Table 3
Table 4: The relationship between type of fracture and infection. View Table 4
The result of this study confirms that children are not exempt from fractures of the femur. Both genders were affected. Whereas in patients younger than one year there was a slight predominance towards the female gender with the male:female ratio approximately 1:1, this ratio was reversed as the patients get older with the ratio approximating 2:1. (Table 5) This pattern had been reported by earlier studies [2] and may not be unconnected to the increased activity level and tendency to risk exposure of the male child compared to the female child as they grow older [2].
Table 5: Age distribution. View Table 5
As had been previously reported, whilst road traffic crashes remain the highest contributor of fractures in children [4], fall was a frequent contributor in children under the age of 10 years [4,5] with the mean age of patients with fractures from ground level falls in this study been (3.3) years while those from falls from height being 11.7 (6.1) years [4,8], Table 6. The use of children who should be in school as child hawkers on the streets and highways may explain the high number of femoral fractures resulting from RTC because of higher risk exposure [25]. The UNICEF Report 2013, shows that 20% of the worlds out-of-school children are in Nigeria [26]. A recent survey by the UNICEF in 2015 reported that about 13.2 million children in Nigeria are out of school [27]. These are the children who often will become child hawkers and beggars on the streets with associated exposure to traffic hazards. This pattern had existed even during the period of this study. One important observation is the contribution of falls from trees to femoral fractures seen in 32 patients (10.2%). These falls are often seasonal and coincide with the seasons of various economic fruits especially mango tree and other seasonal economic fruit trees in the region. This pattern had been observed by Nwadinigwe, et al. in 2006 and Onyemaechi, et al. in 2016 both in Enugu Nigeria [3,4] in Papua, New Guinea [5], and India [7] where falls from heights particularly seasonal fruit trees was a common cause of fractures. Ensuring that most children attend schools may reduce the exposure to such hazards which is highest amongst out-of-school children [25]. Only one patient was observed with fracture resulting from birth trauma. This pattern is not surprising as fractures of the femur during birth are rare and often discovered latently. Risk factors for these injuries include breech deliveries; twin pregnancies and osteoporosis of birth related to prematurity [28].
Table 6: Cause of injury. View Table 6
A significant proportion of the fractures were closed fractures (286, 91.1%) Figure 1. However, some of the fractures were open. In children, open fractures are not as common as in adults, but when they do occur, they carry significant mortality and morbidity because of the severity of the injury and the reduced ability of children to withstand the associated haemodynamic derangement associated with such injury [16]. Also, open fractures in the femur are usually not as common as those of the tibia - the reason been partly due to the rich soft tissue envelope of the femur [29].
Most of the fractures were transverse and short oblique (266, 84.7%) as compared to the spiral fractures (27, 8.6%), Figure 3. This pattern is not surprising as a significant proportion of the fractures resulted from high energy injuries from road traffic crashes. Injuries from ground level falls often result in spiral fractures. Both sides were equally affected in the distribution of injury with a statistically significant preponderance to injury with a statistically significant preponderance
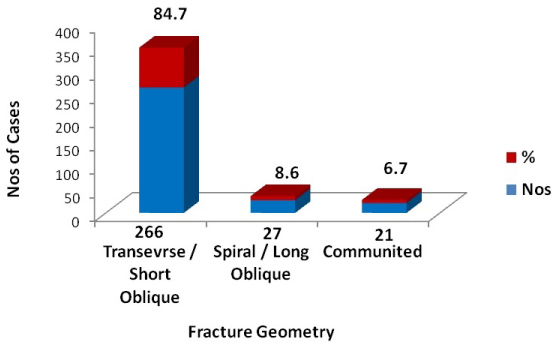 Figure 3: Fracture geometry.
Figure 3: Fracture geometry.
χ2 = 370.419; P-value < 0.00001.
View Figure 3
Table 7: Localization of fracture and laterality of injury. View Table 7
Whereas non-operative treatment by casting with POP (114, 36.5%) and traction (88, 28.0%) was used in most of the cases, operative treatment was utilized in about a third of the patients with Internal fixation (90, 29%) particularly intramedullary nailing (32, 10.2%), and plates and screws (35, 11.1%) especially in the older children whose fractures were treated just like adult fractures. This is a common practice in most series [11]. One patient with type IIIC fracture had amputation. It is worth noting that no patient had fixation with Titanium elastic nails which were rarely available in the region as at the time of this study. Patients that that open fractures with extensive soft tissue wounds were treated with external fixators [11].
A significant proportion of the fractures (281, 85.5%) had achieved radiological union by 12 weeks after definitive treatment, whereas only 4 (1.2%) of the cases had not achieved radiological union as at 24 weeks after definitive treatment Table 2. The reason for this pattern is not surprising; as fractures in children tend to heal faster and better than those of adults. This pattern may be related to the high periosteal activity of the growing bones in children [30]. In keeping with the healing rate of the fractures, a significant proportion of the patients were hospitalized for periods of 6 weeks and below (282, 89.8%), Figure 4. The reason for this high union rates may be related to the fact that majority of the fractures were closed and managed by non-operative methods which did not compromise the fracture hematoma as such increased the chances of rapid healing of the fractures [30].
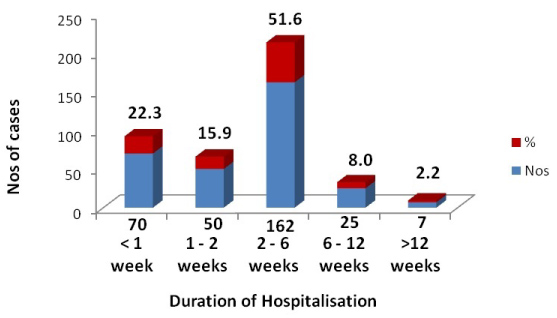 Figure 4: Duration of hospitalization.
Figure 4: Duration of hospitalization.
χ2 = 231.333; P -value < 0.00001.
View Figure 4
Observation of the complication rates (Table 3) indicated that adverse events from the treatment of such fractures such as infection, malunion, non-union and implant failure were lower than those for adult fractures [30]. Again, this may be attributed to the fact that a good proportion of the fractures were treated by non-operative methods as mentioned above, and the healing and remodeling potential in children may have been the reason that the observed malunion and non-union rates were low. That no implant failure was recorded could be explained that majority of the fractures had reached an advanced stage of healing early enough to reduce the stress and fatigue on the implants from delayed on non-united fractures. A closer look at the infection rates for various types of fractures showed that Gustilo/Anderson types III A and B open fractures had significantly higher infection rates with Adverse ration (0.50, 0.33) respectively than closed and Gustilo/Anderson types I fractures and type II (0.007,0.1) respectively (Table 4). Again, this may be related to the fact that open fractures in children although not common are often severe and often associated with significant morbidity when they do occur [31].
Fractures of the femur in children constituted about 25% of the fracture involving the femur seen at the trauma centre. Road traffic crashes and falls from heights were the leading causes of such injuries with falls from trees contributed about 10% of such fractures. Ensuring that children are in school may reduce the risk exposure of children to fractures of the femur. Non-operative treatments with properly applied casts and traction for suitably selected fractures of the femur in children produce acceptable results.
The study was approved by the Research and Ethical Review Committee of International Centre for Advanced Medical Care and Development (ICAMCAD) who are the developers of the registry.
Not applicable.
The data that support the findings of this study are available from the authority of International Centre for Advanced Medical Care and Development (ICAMCAD), but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the authority of International Centre for Advanced Medical Care and Development.
We acknowledge the Board and Management of International Centre for Advanced Medical Care and Development for allowing access to the data from their trauma registry.
Authors have declared that no competing interests exist.