This is a case of a 35-year-old male who presented with signs and symptoms of direct tenderness on left and right lower quadrants of abdomen and was later diagnosed to be having ruptured intra-abdominal testicular seminoma with 2 liters of hemoperitoneum. Exploratory laparotomy and excision of intra-abdominal mass was done. Rupture of intra-abdominal testicular seminoma is a rare cause of abdominal pain with associated hemoperitoneum. Patient claimed both testes to be retractile and palpable occasionally on the upper scrotal and inguinal area. Although physical exam revealed negative bilateral testes, immediate imaging was not able to provide the definite pre-operative diagnosis. Patient was sent home and was advised for follow up after 3 months under active surveillance.
Abdominal pain may be due to a variety of diseases that may involve gastrointestinal system, biliary tract, solid viscera or genitourinary system. Identification of patients who require surgery is important for timely management. Undescended testis [1] has an incidence of 1 in 500 men (0.2%), and can be associated with complications like malignancy, infertility, torsion and hemorrhage. It has a 40 times higher risk of malignant transformation, most commonly seminoma, as compared with scrotal testis. Rupture of intra-abdominal seminoma [2] is very rare. Only five (5) cases with same presentations have been reported worldwide, till date [3-7].
A 35-year-old male, presented with abdominal pain after allegedly lifting heavy boxes during work. Patient has no comorbidities except for bilateral undescended testes [8]. Patient claims to palpate both testes occasionally above the scrotal pouch and inguinal canal. Patient last palpated his left and right testis on the scrotal area 3 years and 1 year ago respectively.
4 days prior to admission, patient noted vague abdominal pain while lifting heavy boxes during work which prompted immediate consult at a private institution, where workup was done and was subsequently admitted. Initial hemoglobin was 40 g/L. Patient was transfused with 3 units of packed red blood cell. Whole abdominal ultrasound was done which revealed an isodense structure seen in the right lower abdomen measuring 12.1 × 9.1 cm and large amount of free fluid in the peritoneal cavity. Patient was advised surgery, however due to financial constraints, opted to transfer to our institution.
On admission, his blood pressure was 110/70 mmHg, pulse rate was 95 beats/min, respiratory rate of 16 breaths/min, temperature of 36 °C, O2 sat of 99%. On physical examination, abdomen was soft, with direct tenderness on the left and right lower quadrant. No visible or palpable hypogastric nor inguinoscrotal bulging mass was noted. Both scrotal pouch are negative for presence of testis. Digital rectal examination was unremarkable. Chest and abdominal X-ray revealed unremarkable result, no pneumoperitoneum was noted. Initial complete blood count, revealed hemoglobin concentration of 85 g/L and white blood cell count of 7,800/mm3. Plan was to optimize patient's condition by hydration and transfusion of 2 unit packed red blood cells prior to surgery. Whole abdominal computed tomography scan with triple contrast was requested and revealed a heterogenous intraperitoneal mass in the mid lower abdomen, superior to the urinary bladder measuring 12.5 × 9.6 cm, displacing the bowel loops superiorly and laterally, with impression of To consider Blood clot formation, mid lower abdomen and a large amount of fluid accumulation in the peritoneal cavity. Both testes were not seen within the inguinoscrotal sac and the rest of the scan was unremarkable. With the patient's condition optimized, patient was brought to the operating room. Preoperative diagnosis was Anemia, probably secondary to bleeding intra-abdominal mass.
Exploratory laparotomy was done, Initial finding was approximately 2000 mL of hemoperitoneum, with an actively bleeding mass on the hypogastric area which has connections to the right inguinal canal. The mass, with size of 12 × 10 × 8 cm, covered with tortuous blood vessels and with continuous bleeding at its 1 cm point of rupture on its anterolateral aspect. Excision of the intra-abdominal mass was done. No other mass was found and the solid viscera, mesentery and intestines were found to be normal. Patient tolerated the procedure.
After revealing an intra-abdominal testicular mass, additional workup and further imaging was requested including serum LDH, AFP and b-HCG. Tumor markers revealed 3x elevated LDH and within normal AFP and b-HCG (Table 1).
Table 1: Serum Tumor markers Post orchiectomy Day 1. View Table 1
Specimen was sent for histopathology. Result is conclusive of seminoma, classical type, tumor size 13 cm greatest dimension. Negative for lymphovascular space invasion. Negative for tumor involvement: 1) Epididymis 2) Spermatic cord. Patient is classified as Stage IS (pT1b N0 M0 S2). Patient was discharged after three days and was advised for follow up after three months with repeat serum tumor markers and Chest X-ray and abdominal CT scan (Figure 1, Figure 2, Figure 3 and Figure 4).
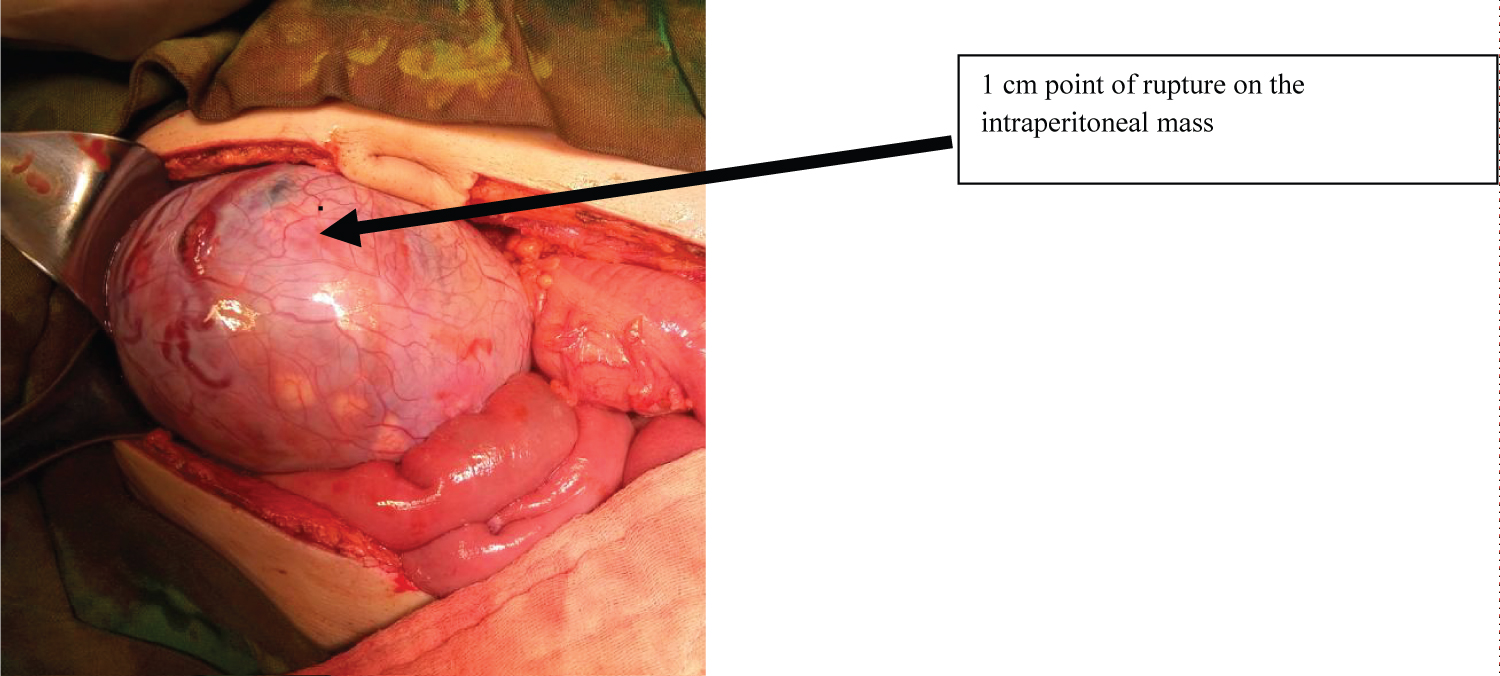 Figure 1: Intraperitoneal mass 12 × 10 × 8 cm covered with tortuous blood vessels and 1 cm point of rupture at its anterolateral aspect.
View Figure 1
Figure 1: Intraperitoneal mass 12 × 10 × 8 cm covered with tortuous blood vessels and 1 cm point of rupture at its anterolateral aspect.
View Figure 1
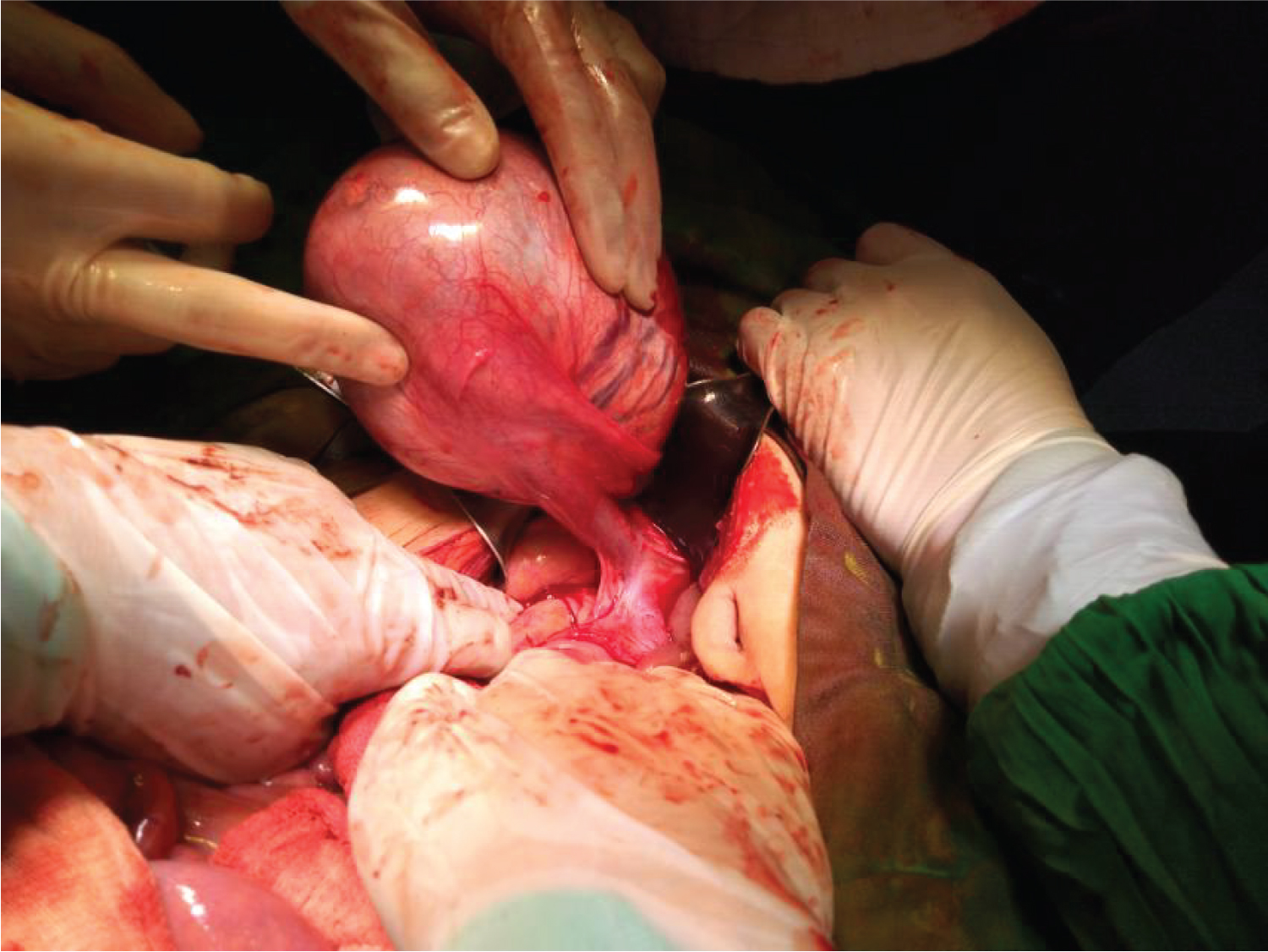 Figure 2: Intraperitoneal mass retracted anteriorly revealing connection to the right inguinal canal, probably spermatic cord and its vessels.
View Figure 2
Figure 2: Intraperitoneal mass retracted anteriorly revealing connection to the right inguinal canal, probably spermatic cord and its vessels.
View Figure 2
 Figure 3: Gross specimen of testicular tumor.
View Figure 3
Figure 3: Gross specimen of testicular tumor.
View Figure 3
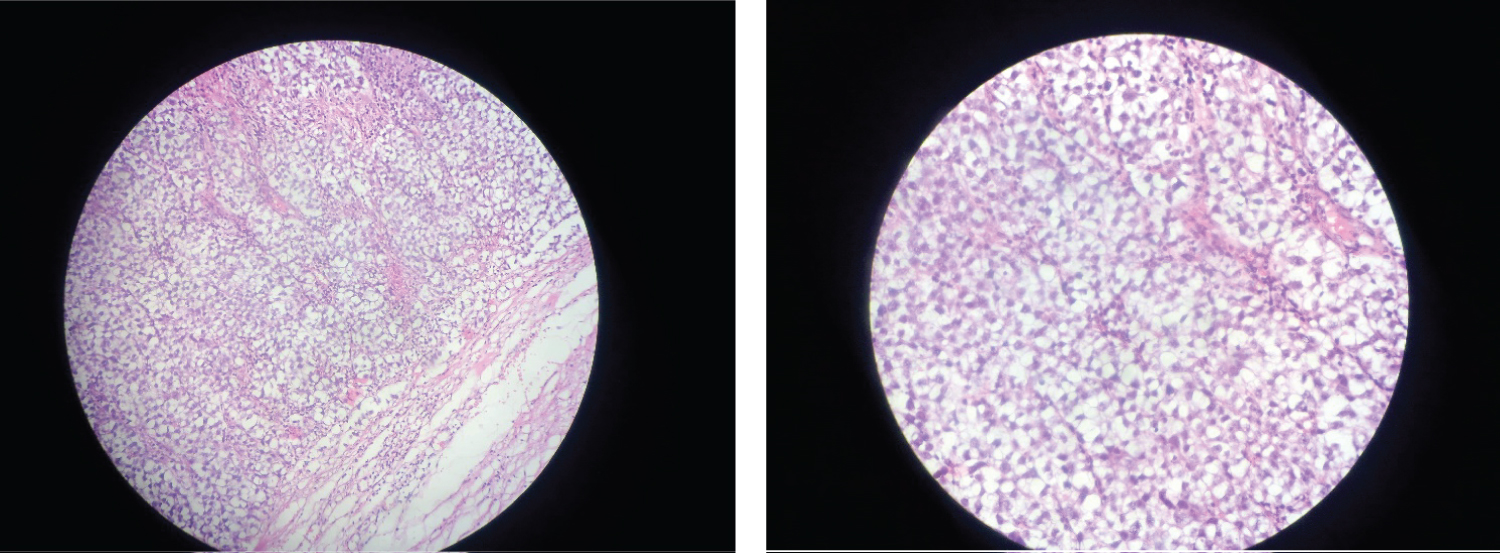 Figure 4: Actual slides of tumor showing seminoma cells within fibrous septae.
View Figure 4
Figure 4: Actual slides of tumor showing seminoma cells within fibrous septae.
View Figure 4
Cryptorchidism is a developmental defect in which the testes fail to descend completely in the scrotum and has an incidence of 1 in 500 men (0.2%). True undescended testis is unilateral in 75% of cases. Our patient presented with bilateral undescended testis which composes 25% of cryptorchidism cases [4]. Testicular germ cells tumors affect 1% of young men. They have a prevalence of 1% of all neoplasms in men, with the peak incidence between 20 to 40-years-old. Approximately 10% of testicular tumors arise from undescended testis. Rupture of intra-abdominal seminoma is very rare. As of October 2019, listed below are the published case reports with same case of ruptured intra-abdominal seminoma.
• Locally published case reports (Philippines): 0
• Internationally published case report: 5
• Massive bleeding caused by rupture of intra-abdominal testicular seminoma: Case report [3].
• Spontaneous rupture of an Intraabdominal testicular tumor: A case report [9].
• Ruptured seminoma of undescended testis presenting as acute abdomen: Case Report with Literature review [5].
• A torted ruptured intraabdominal testicular seminoma presenting as an acute abdomen [6].
• Spontaneous rupture of seminoma in undescended testis with hemoperitoneum: A rare presentation [7].
The most common location of undescended testis is within the inguinal canal. Approximately 90% of tumors in undescended testis are seminomas, particulary those that occurs in abdominally located testis [10]. A patient with an undescended testicle has at least four times the risk for carcinoma compared to a normal testicle. In the Philippines, cryptorchidism in the adult population has lessen due to the practice of elective orchidopexy in children aged under 2-years-old and orchiectomy in post puberal patients. According to the patient, both testes are occasionally palpable up to the upper scrotal area, but does not descend fully on the scrotal pouch. No consult was done. Patient had two children, one 14-year-old and one 12-year-old, which made him not to worry about his condition.
The peak incidence of malignancy in undescended testis is in the third or fourth decade of life. Clinically, patients with malignant intra-abdominal testis can be asymptomatic or may present with symptoms mimicking appendicitis, incarcerated hernia, urinary frequency or dysuria from mass effect on bladder or as acute abdomen due to torsion and rupture with hemorrhage. Our patient only presented with direct tenderness on both lower quadrants of abdomen. Radiological and preoperative diagnosis of complications such as torsion or rupture is often difficult because, generally, imaging findings can be non-specific.
In a male patient with undescended testis, and an intraperitoneal mass on imaging, testicular malignancy should be suspected. A definite diagnosis and treatment usually involves operative exploration and resection of mass. If there is a probability of a testicular tumor, the tumoral markers might bring further evidence and also will be of use for post operative management and follow up. LDH is three times elevated than normal in our patient, hence classified into Stage IS Seminoma. Staging includes pT1b (Tumor 3 cm or larger in size) N0 (No regional lymph node metastasis) M0 (No distant metastasis) S2 (LDH 1.5 - 10x normal).
According to the latest NCCN Guidelines for testicular cancer [11], standard management options after initial orchiectomy include active surveillance for pT1-pT3 tumors (preferred), chemotherapy with 1 or 2 cycles of single-agent carboplatin, or RT at 20 Gy (preferred) or 25.5 Gy. Disease-specific survival for stage I disease is 99% irrespective of the management strategy used.
On our case, tumor marker levels are elevated even after surgery, and the tumor has not spread within the epididymis or spermatic cord. In this stage, one or tumor marker levels is still high after the testicle containing the seminoma has been removed. This is very rare, and it can be treated with chemotherapy. However, physicians are cautioned against treating a patient based on minimally elevated LDH or beta-hCG alone, as other causes may be responsible for elevation of these markers. Persistent elevation of serum markers is usually evidence of metastatic disease, which will show up radiographically if doubt exists in the diagnosis.
Active surveillance was advised to our patient which includes history and physical examination, abdominal CT scan, with optional measurement of postorchiectomy serum tumor markers (AFP, beta-hCG, and LDH), performed every 3 to 6 months for the first year, every 6 to 12 months for years 2 to 3, and annually for years 4 and 5. No initial isolated relapses in the lung have been reported in studies of patients with stage I seminoma managed by active surveillance; therefore, routine chest imaging, including chest X-ray and chest CT with contrast, is only indicated for patients with thoracic symptoms.