The yellow ligament, or Ligamentum flavum, is the ligament that connects the lamina arches of two adjacent vertebrae in the spine [1,2]. This ligament is yellow and has elasticity [3,4]. Ligamentum flavum ossification is an uncommon cause of pressure on the cervical cord [3] [5-7]. Ligamentum flavum ossification commonly occurs in the thoracic cord which can cause myelopathic symptoms in the patient [8,9]. The main cause of this problem is unknown, but it occurs when the soft tissue of the spine is calcified and causes narrowing of the spinal canal [10,11].
The patient is an 80-year-old man who presented with pain and paresis in all four limbs about a year ago. The patient's symptoms have worsened over the past month. The force of the patient's upper limbs was about three-fifths and the lower limbs were about four-fifths. The patient complained of numbness and tingling in all four limbs, especially the upper limbs. Sphincter disorder has been characterized by urinary incontinence, which began a year ago and has now worsened over the past few months. Hoffman's sign was positive on both sides.
Magnetic Resonance Imaging (MRI) of the cervical spine showed stenosis with cord compression from C3 to C7 levels (Figure 1). Sagittal computed tomography image of the cervical spine showing ossified yellow ligament from c4 to c7 (Figure 2 and Figure 3).
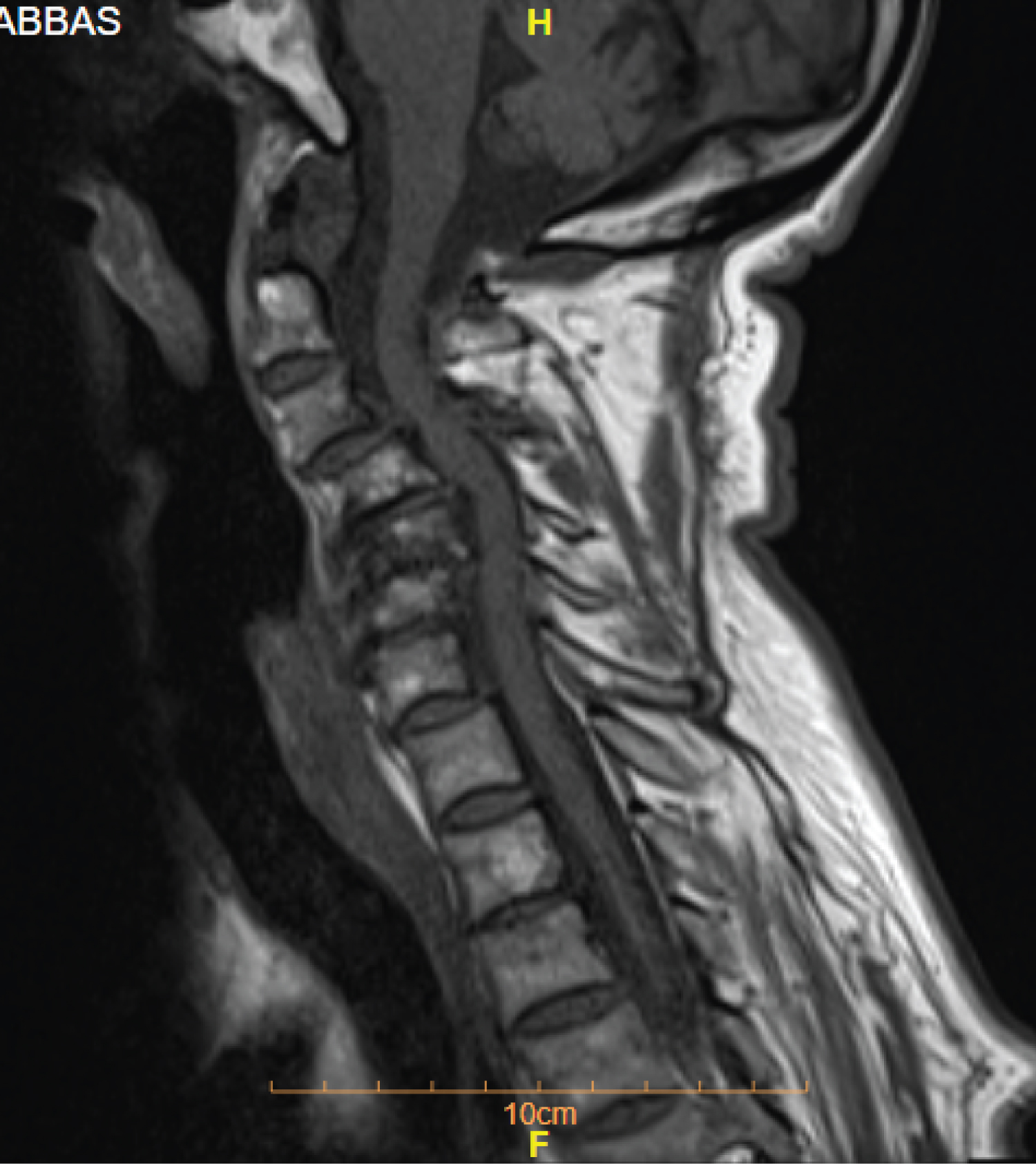 Figure 1: Sagittal T1 weighted MR image of the cervical spine showing a narrowed spinal canal due to a low signal intensity mass anterior to the posterior elements with cord oedema at C4 - C7 levels.
View Figure 1
Figure 1: Sagittal T1 weighted MR image of the cervical spine showing a narrowed spinal canal due to a low signal intensity mass anterior to the posterior elements with cord oedema at C4 - C7 levels.
View Figure 1
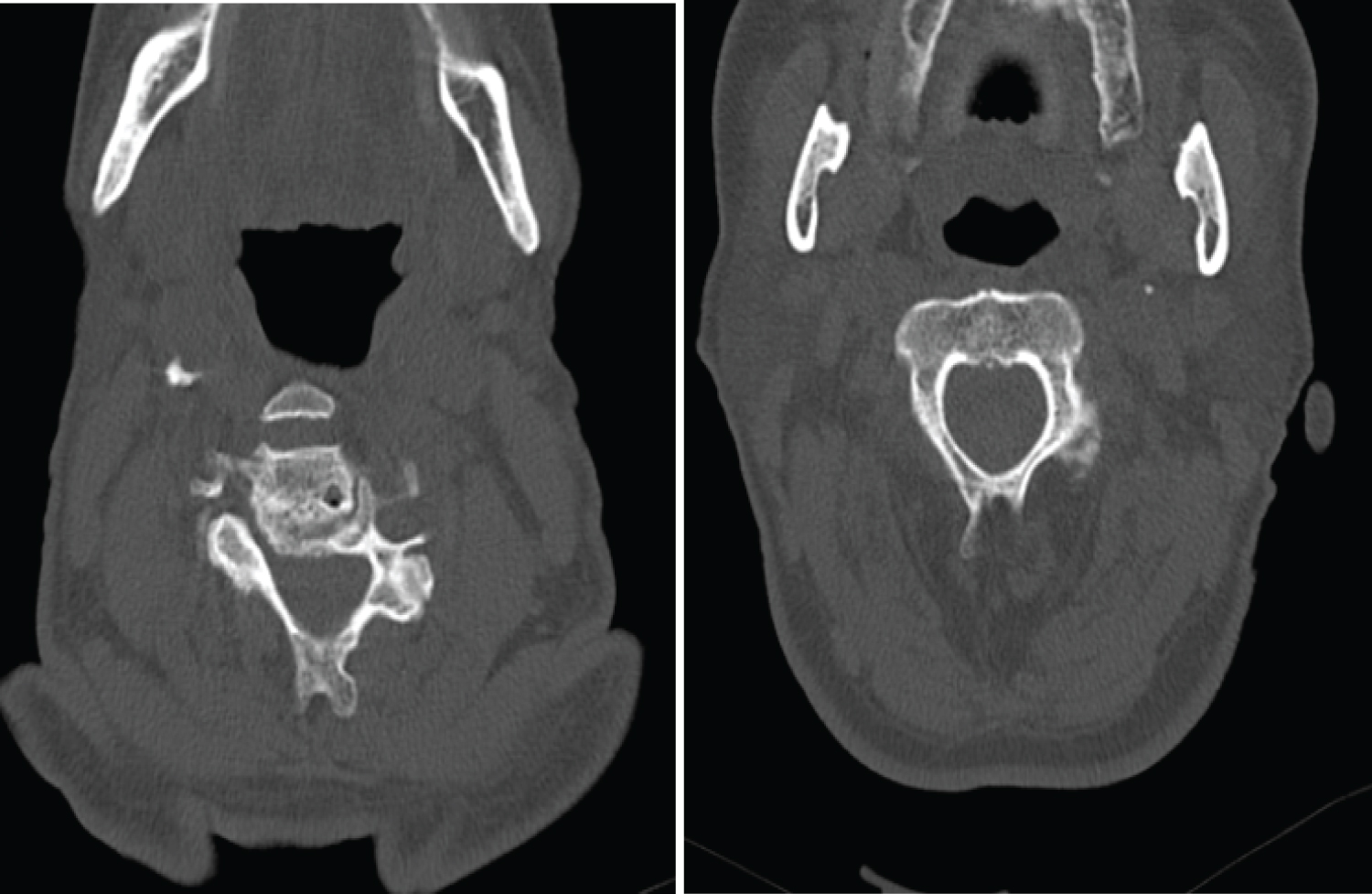 Figure 2: Axial computed tomography image showing thickened nodular ossified yellow ligament.
View Figure 2
Figure 2: Axial computed tomography image showing thickened nodular ossified yellow ligament.
View Figure 2
 Figure 3: Sagittal computed tomography image of the cervical spine showing an ossified yellow ligament.
View Figure 3
Figure 3: Sagittal computed tomography image of the cervical spine showing an ossified yellow ligament.
View Figure 3
Based on the above findings, cervical myelopathy due to pressure on the cord was diagnosed as a result of OYL. Posterior laminectomy and removal of the yellow ligament was performed for the patient. Due to the stability of the cervical vertebrae and the fusion of adjacent vertebrae, no device was performed for the patient (Figure 4). The sample sent to the lab showed endochondral ossification, which was consistent with our diagnosis. Three months after surgery, the patient's symptoms, including paresthesia and loss of limb strength, improved relatively.
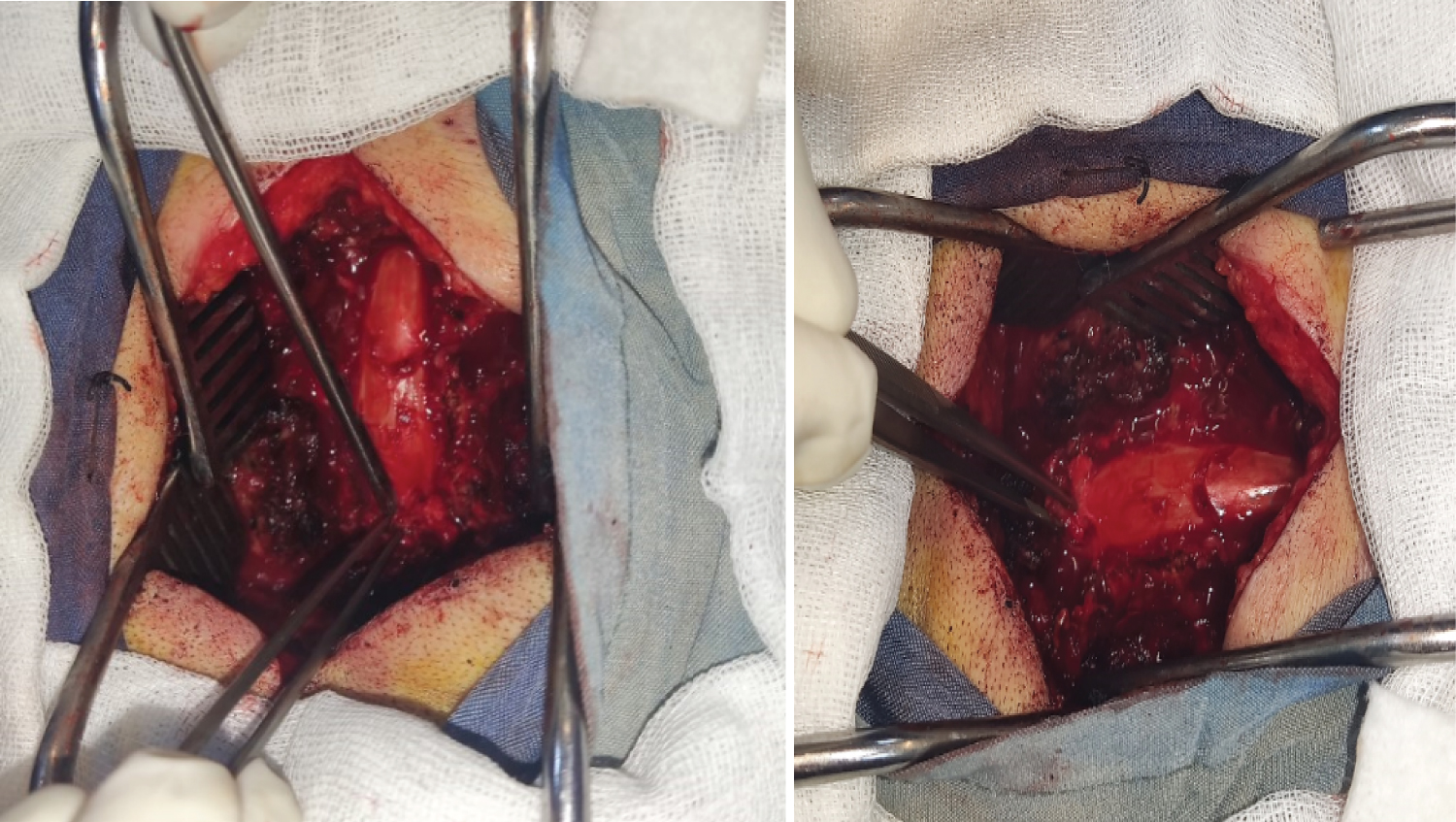 Figure 4: Intraoperative photograph of the surgical field, after posterior instrumentation and laminectomy, showing the ossified segment of the yellow ligament pointed with the curette.
View Figure 4
Figure 4: Intraoperative photograph of the surgical field, after posterior instrumentation and laminectomy, showing the ossified segment of the yellow ligament pointed with the curette.
View Figure 4
Increasing the thickness of the yellow ligaments leads to a decrease in the diameter of the spinal canal, which is one of the causes of spinal stenosis [9,12]. Cervical myelopathy following yellow ligament ossification is very uncommon and has been reported in most cases from Asia [13]. The follow-up of this patient showed that if the cervical vertebrae are stable, device placement is not required in all cases [11].
This case report was one of the rare cases of yellow ligament ossification that occurred in the cervical spine. And showed no need for device placement in all patients.