Facial Nerve Palsy is mostly idiopathic in nature. Every patient with a facial nerve Paralysis needs to go under through investigation, most importantly imaging to exclude other causes such as neoplasms. In very rare cases, the normal imaging results may be misleading and occult tumor or perineural spread along the nerve may not be detectable. Luckily these cases may present with alarming signs such as progressiveness nature associated with pain, complete Paralysis with no recovery and most importantly a history of regional skin cancer. These signs, when correctly interpreted, warrant for surgical exploration and biopsy avoiding misdiagnosis in patients with occult malignancy. We present a case report of a patient who initially diagnosed as idiopathic facial nerve Palsy which later turned to have a perineural invasion with occult metastasis of squamous cell carcinoma of the skin in the parotid gland as well as a review of the literature reporting similar cases.
Bell's Palsy remains the most common cause of facial nerve paralysis [1]. Nonetheless, any patient with a history of malignancy must be extensively and thoroughly investigated before concluding the diagnosis of Bell's palsy. A normal MRI does not exclude the malignancy, cases with occult malignancy demonstrate initially normal radiological finding [2-8]. Thus, a delay in diagnosis [9]. Awareness of this rare possibility lead to careful acquisition interpretation of patient history and high suspicion index in risk patient will help to shorten diagnostic delay and to implement further diagnostic workup like biopsy rather than simply categorizing these cases falsely under Bell's Palsy [8]. In this case, we report about a patient who had a facial nerve for nine months initially diagnosed as Bell's Palsy, which turned out to be an extensive Perineural invasion of the facial nerve despite normal MRI.
A 70-years-old male with a known case of chronic renal impairment on dialysis, renal hypertension, secondary hyperparathyroidism and hyperuricemia, status post hemithyroidectomy for papillary thyroid cancer before 20 years presented to the Neurology clinic in our University hospital of Augsburg with a complete Facial Nerve Paralysis of the right side. The facial weakness began about nine months before his presentation; the weakness was progredient and had a partial response to Steroid Therapy. The first symptom was right side earache without discharge, 14 days later, he started to notice a progressive weakness around the eye with increased eye tearing on the same side. Later he started to develop progressive weakness around the mouth. Lately, he has been experiencing pain around the Mandible and right side of the neck followed by Hypoesthesia on the tip of the tongue. His first medical contact was with his Family doctor who referred him to MRI examination, after one and half months he had the referred to a neurologist who prescribed him Prednisolone 75 mg for 14 Days which improved temporarily the clinical picture. The patient later experienced a worsening to his symptoms, so his Neurologist referred him to the Neurology Clinic in the University Hospital for diagnostic. The patient denied any had no taste impairment, but he reported Hyperacusis.
Eight months after the beginning of facial paralysis, the patient received surgical excision by Dermatology clinic of Keratoacanthoma on left Eyebrow area, whereby three suspicious skin lesions on the right side of the face were biopsied, two of them on the cheek area and the third one on Nasal dorsum. Histology was positive for Squamous cell carcinoma (SCC) in all three lesions of the right side of the face. Surgical excision performed with R0 margins achieved. All the three tumors were well-differentiated SCC. The tumors ranged from T1-T3 (0.9 mm to 4.0 mm). The patient had a cN0 neck on Sonography exam.
A month after the first diagnosis of skin SCC, the patient was admitted under Neurology care for Facial Paralysis diagnostic. A second MRI without contrast because of the renal impairment was done. The diagnostic test included EMG, Somatosensory Evoked Potential of the Trigeminal nerve, Lumbar Puncture, and ENT consultation, which included Audiogram and head and neck ultrasound examination.
The Neurological Diagnostic Tests were without abnormality. There was no mention of the SCC in the neurologist Discharge Summary. Both MRI failed to show any abnormality of the Facial nerve (Figure 1). EMG showed no Reinnervation potential. Lumber Puncture showed light elevation of protein but was otherwise, including cell count and Lyme serology, were normal. ENT consultation includes Audiogram and Parotid/Neck Sonography failed to reveal any cause of facial palsy. A follow up after EMG to plan Facial Reanimation was arranged. The patient received a short course of cortisone without any improvement. The patient was discharged from the Neurology clinic with Idiopathic Facial Paralysis as a diagnosis.
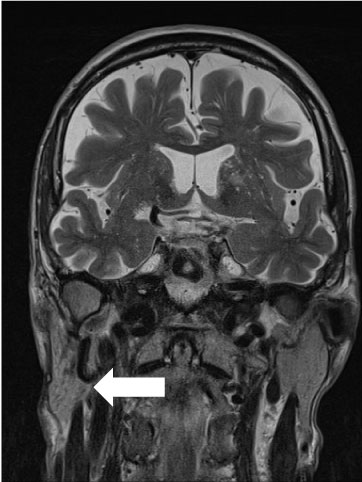 Figure 1: Turbo spin echo MRI Coronal Image shows Normal Parotid Tissue on the right side (marked with an Arrow).
View Figure 1
Figure 1: Turbo spin echo MRI Coronal Image shows Normal Parotid Tissue on the right side (marked with an Arrow).
View Figure 1
The Patient presented to the ENT clinic a month after discharge for the Follow-up appointment. Sonography this time revealed a normal Parotid gland but a thickening of the Greater Auricular Nerve with inhomogeneous hypoechoic texture (Figure 2). A Biopsy of this lesion revealed a good differentiated SCC with Perineural invasion. A staging including CT Thorax without contrast and Ultrasound examination of Neck and Abdomen was performed and revealed no distant metastasis.
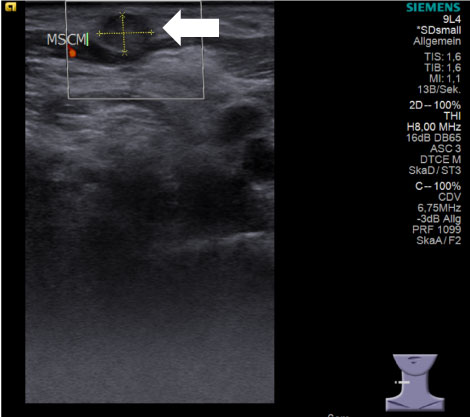 Figure 2: Ultrasound of the neck revealing thickening of the Great Auricular Nerve (marked with an Arrow).
View Figure 2
Figure 2: Ultrasound of the neck revealing thickening of the Great Auricular Nerve (marked with an Arrow).
View Figure 2
Based on the result, a radical parotidectomy with neck dissection was recommended by our Tumor Board.
The Operation included Unilateral Neck dissection, where Intraoperatively there was no detectable gross lymph node metastasis, the complete resection of the Greater Auricular Nerve was done; the facial nerve main trunk was dissected, and it was surrounded by a tumor. Here a radical parotidectomy with facial reanimation was done, the frozen section of facial never at stylomastoid foramen was free of tumor.
The final Pathology report showed two areas of diffuse carcinoma infiltration growing in small tumor cells nests and showing typical squamous features with poor differentiation. The neck tissue had 18 Lymph nodes, one of them showing a papillary thyroid tumor metastasis. The definitive report of the facial nerve showed small carcinoma infiltrate.
Based on the pathology report, a mastoidectomy with resection of the mastoid segment of the facial nerve was performed. The nerve intraoperatively was grossly normal (Figure 3 and Figure 4).
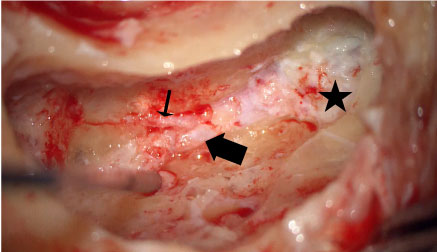 Figure 3: Intraoperative microscopic picture showing the mastoid segment of the facial nerve (large arrow). Chorda Tympani nerve (small arrow) and Stylomastoid fat (star) can be recognized.
View Figure 3
Figure 3: Intraoperative microscopic picture showing the mastoid segment of the facial nerve (large arrow). Chorda Tympani nerve (small arrow) and Stylomastoid fat (star) can be recognized.
View Figure 3
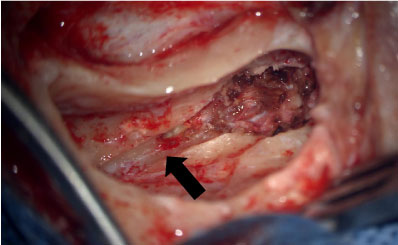 Figure 4: Intraoperative picture after resection of the mastoid segment of the facial nerve showing facial canal (marked with an arrow).
View Figure 4
Figure 4: Intraoperative picture after resection of the mastoid segment of the facial nerve showing facial canal (marked with an arrow).
View Figure 4
Later the final pathology report revealed carcinoma infiltrate. So that a revision with resection of the extracranial segment of the facial nerve was performed that included the ossicular disarticulation and rest of mastoid Segment as well as tympanic segment, the nerve was resected at the level of Geniculate ganglion (Figure 5 and Figure 6). There was no sign of CSF leak the stump of the nerve was covered with fat graft. The ossicular reconstruction was performed using Incus interpostioning.
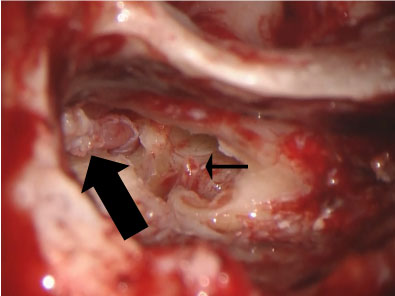 Figure 5: Intraoperative view of tympanic segment of the facial nerve (large arrow) after ossicular disarticulation, here Stapes can be recognized (small arrow).
View Figure 5
Figure 5: Intraoperative view of tympanic segment of the facial nerve (large arrow) after ossicular disarticulation, here Stapes can be recognized (small arrow).
View Figure 5
Figure 6: Intraoperative view after resection of the tympanic segment of the facial nerve showing the empty tympanic facial canal (large arrow) and Stapes (small arrow).
View Figure 6
The pathology report showed carcinoma infiltration with massive Perineural invasion (Figure 6 and Figure 7). With R1 resection margin the patient was referred to the Radiotherapy clinic based on Tumor Board decision.
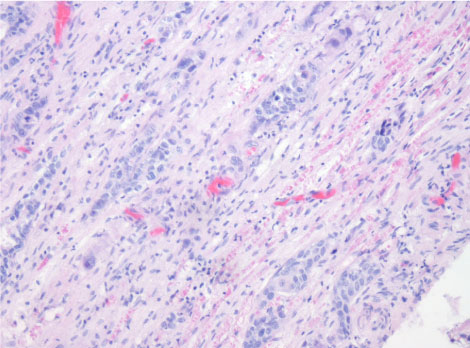 Figure 7: Histology slide showing squamous cell infiltration of the facial nerve.
View Figure 7
Figure 7: Histology slide showing squamous cell infiltration of the facial nerve.
View Figure 7
Cutaneous SCC with Perineural Invasion (PNI) accounts for 14% of all Cutaneous SCC. PNI is more seen in face region where it usually involves Trigeminal and facial nerve. It may manifest silently, but it has a significant impact on the survival rate of these patients [10]. When PNI involve the facial nerve, it presents with facial paralysis which not uncommonly misdiagnosed as Bell's Palsy. Neoplasia is a relatively rare cause of facial Paralysis, and sometimes, it is overlooked [9]. Misdiagnosis can be attributed to under investigated cases or inappropriate diagnostic imaging [3]. In rare cases even reassuring imaging results turns to be deceiving an Parotid malignancy or Perineural Invasion of skin carcinoma maybe overlooked [2,4,6,7,11-13]. Our patient had a progressive facial weakness with pain and newly diagnosed skin cancer. Boehner, et al. reviewed 15 patients who had facial nerve paralysis secondary to occult malignancy and normal imaging and diagnosis delay of about two years. In his series the paralysis progressed over mean time of 8.7 months, facial pain or paresthesia was associated with half of the cases. In his series, he concluded a progressive pattern associated pain, other nerve involvement, or history of skin cancer as an indication for surgical exploration [7]. Broderick, et al. report of 6 cases of Facial Paralysis due to occult Malignancy, and he concluded that progressive ear pain with facial paralysis with trigeminal involvement is suggestive of malignancy. Morris, et al. reported 5 patients with perineural spread to the trigeminal or facial nerve, in his series 4 out of five patients had normal imaging, he reported progressive involvement from terminal to proximal fashion [13]. Quensel, et al. reported 4 cases with a sudden rather than progressive facial nerve but showed no improvement after six months [3]. Jungehuelsing, et al. reported eight patients with normal MRI and occult Malignancy involving the facial nerve and suggested a paralysis over 6-12 weeks as alerting sign, but he states that persistent of the paralysis to be more alerting [12]. In our case, there were no signs of reinnervation on facial EMG. In cases with no apparent cause, Facial nerve Paralysis care must be taken before diagnosing it as Bell's Palsy. A detailed History of Progression, as well as associated pain with clinical skin inspection, is mandatory. In cases with a history of parotid or skin malignancy as well as cases that show no improvement after six months, surgical exploration and biopsy of the paralyzed branch are warranted regardless of normal imaging result. In conclusion, facial nerve Palsy should be closely followed up especially in high risk patient or atypical signs or symptom regardless of normal MRI imaging.