Background: A very uncommon subtype of chronic cholecystitis is follicular cholecystitis (FC). Hyperplastic lymphoid follicles and noticeable germinal centers are its defining features. About 2% of standard cholecystectomies involve it. A very uncommon form of chronic cholecystitis is follicular cholecystitis. At least three lymphoid follicles per cent of the gall bladder tissue and an inflammatory infiltrate that is almost entirely made up of dispersed, well-formed lymphoid follicles define it. To prevent misinterpretation of lymphoma, the pathologist needs to be knowledgeable with this condition.
Objective: To educate pathologists about this entity, this case is being presented.
Case description: We describe a case of FC in a 42-year-old woman in this article. Her abdominal pain was clinically determined to be calculus cholecystitis, and laparoscopic cholecystectomy was used to treat it. It was grossly observed that the gall bladder wall had thickened. A histopathological study showed that the gall bladder wall was heavily infiltrated with lymphocytes, which produced lymphoid follicles with distinct germinal centers. We therefore determined that FC was the cause. This growth should not be confused with lymphoma. A thorough histological analysis is diagnostic, and immunohistochemistry may be used in some cases.Objective: To educate pathologists about this entity, this case is being presented.
Conclusion: This case was used to highlight the rarity of follicular cholecystitis. It is a benign and extremely uncommon entity that frequently looks like lymphoma. FC does not seem to be associated with autoimmunity, lymphoma, or obstructive pathologies.
Follicular cholecystitis, Gallbladder, Lymphoid follicles
Diseases of the gallbladder are a major cause of morbidity and mortality. Inflammatory conditions, acute and chronic cholecystitis, granulomatous cholecystitis, follicular cholecystitis, gallbladder polyps, and carcinoma pseudolymphoma are just a few of the disorders that can affect the gall bladder.
The disorder known as follicular cholecystitis causes the creation of several conspicuous lymphoid follicles in the lamina propria of the gallbladder, which results in a pseudo lymphoma pattern [1].
Folicullar cholecystitis is a rather uncommon illness, and little is known about its etiopathology. Gram bacteria infection has been the key factor in causal associations that have been infrequently documented in the literature [2].
A 36-year-old female patient was admitted to the surgical department with right-sided abdominal pain. She was handled carefully. She once again objected to a similar complaint after 3 months. Following that, she underwent cholecystectomy surgery to address her cholecystitis. The pathology division received the specimen for histological examination.
Gross feature: The size of the cholecystectomy specimen was 7 × 2 × 2 cm. The exterior is sleek and smooth the inner surface of the sliced piece displays bile-stained velvety mucosa, and the wall thickness was 0.5 cm. No stones found (Figure 1).
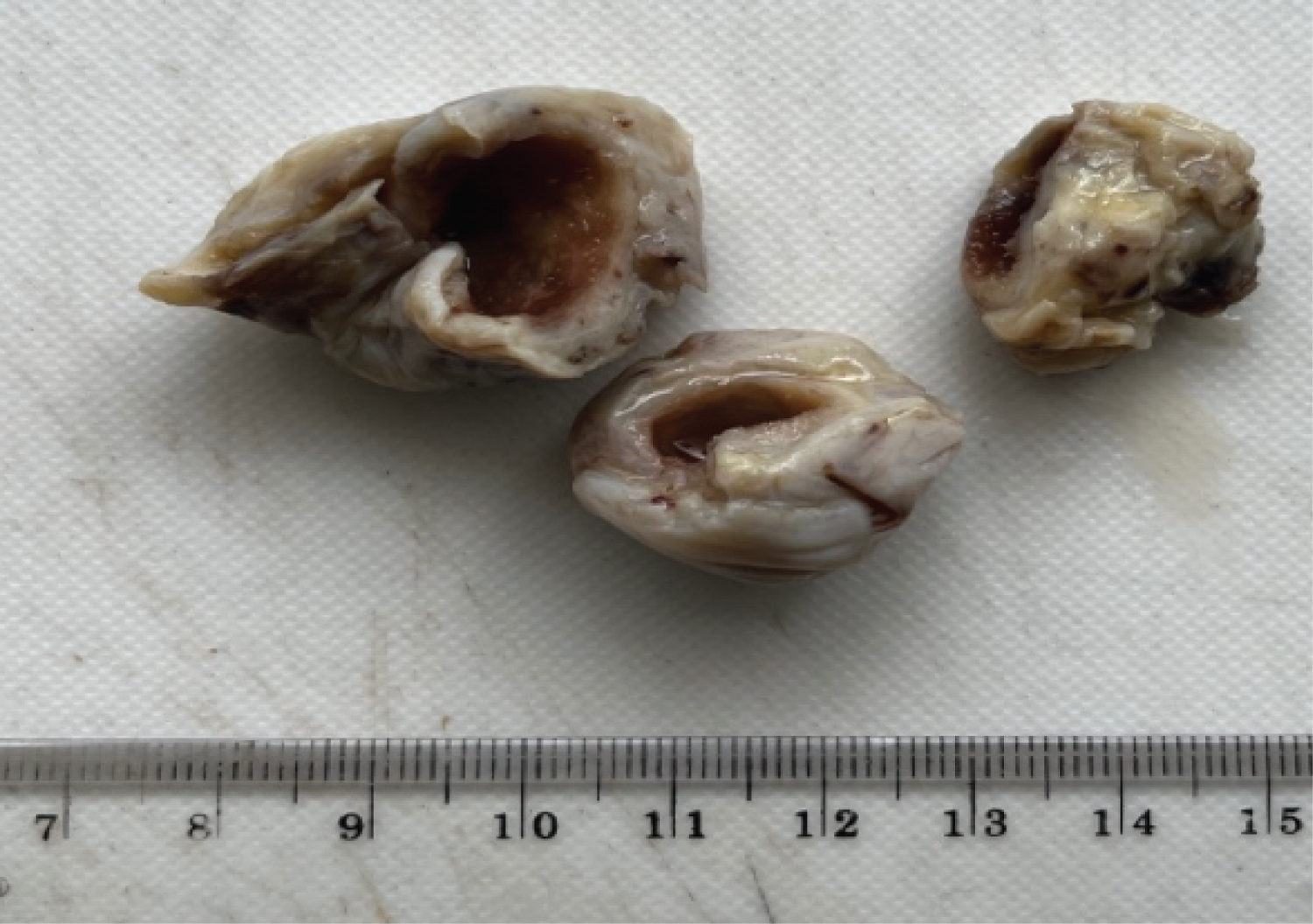 Figure 1: Gross appearance of cholecystectomy specimen.
View Figure 1
Figure 1: Gross appearance of cholecystectomy specimen.
View Figure 1
Microscopy: The gall bladder's Hematoxylin and Eosin-stained slice revealed signs of chronic cholecystitis with the establishment of Rokitansky Aschoff Sinuses in some areas. Proliferating or reactive lymphoid follicles can be seen beneath the lamina propria. There was no necrosis or giant cell. On the basis of the aforementioned findings, follicular cholecystitis of the gall bladder was pathologically diagnosed (Figure 2).
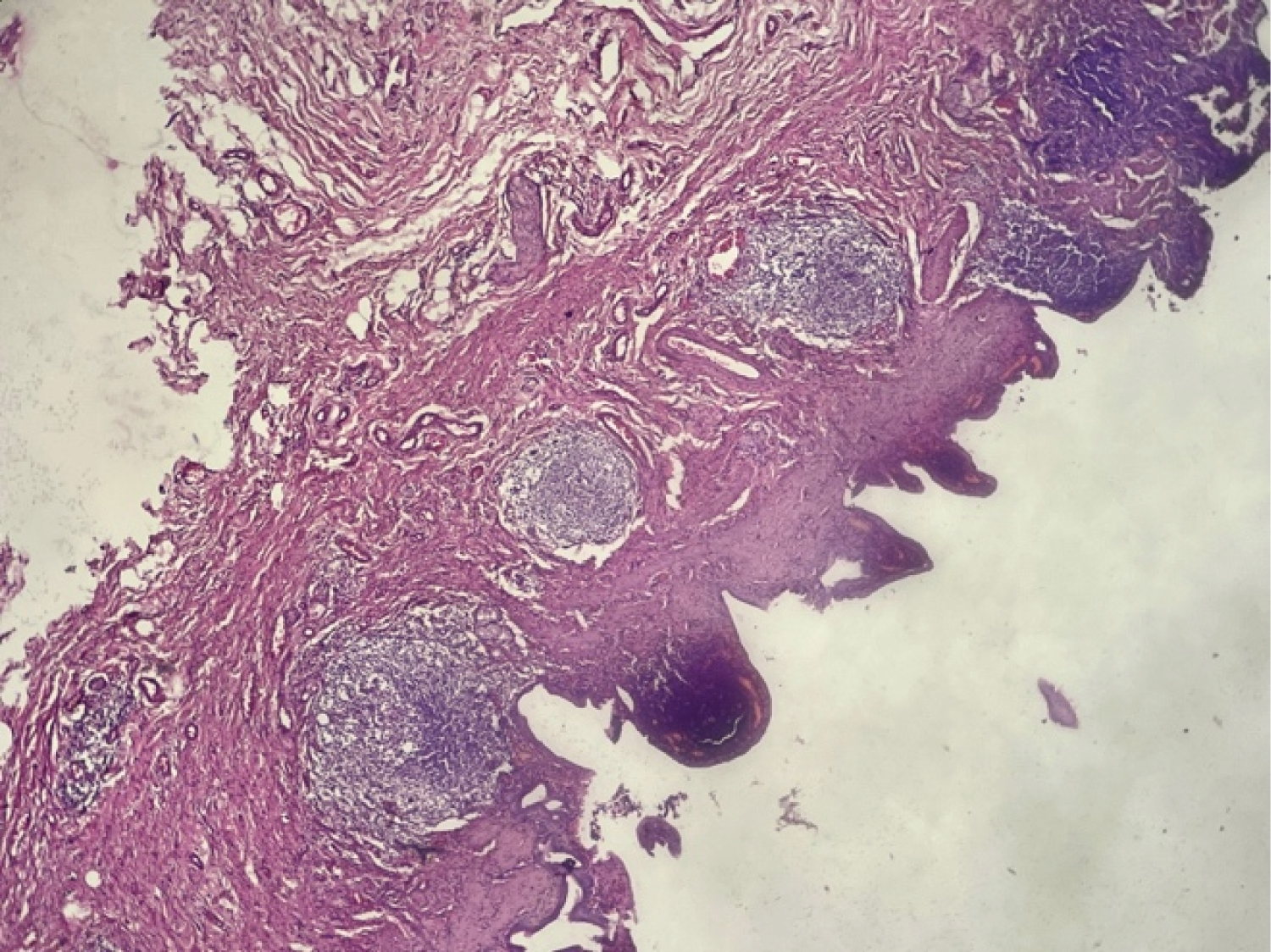 Figure 2: Reactive/proliferation lymphoid follicle in lamina propria (H&E 100x).
View Figure 2
Figure 2: Reactive/proliferation lymphoid follicle in lamina propria (H&E 100x).
View Figure 2
Gallbladder pathology called follicular cholecystitis is quite uncommon. A few cases with an occurrence frequency of under 2% have been published [3]. It consists of polymorphic lymphoid populations dispersed along the entire gallbladder wall in the form of hyperplastic lymphoid follicles with germinal centers [4].
The condition can also affect the skin, GIT, orbit, and lungs [4]. The phrases lymphoid hyperplasia, pseudolymphoma, and follicular cholecystitis are a few that have been used to describe the same gall bladder lesion in the literature [1].
The presence of many germinal-center-containing reactive lymphoid follicles. The potential of a lymphoproliferative lesion was dismissed by the circular cellular lymphoid infiltrate and numerous lymphoid follicles seen (Figure 3 and Figure 4).
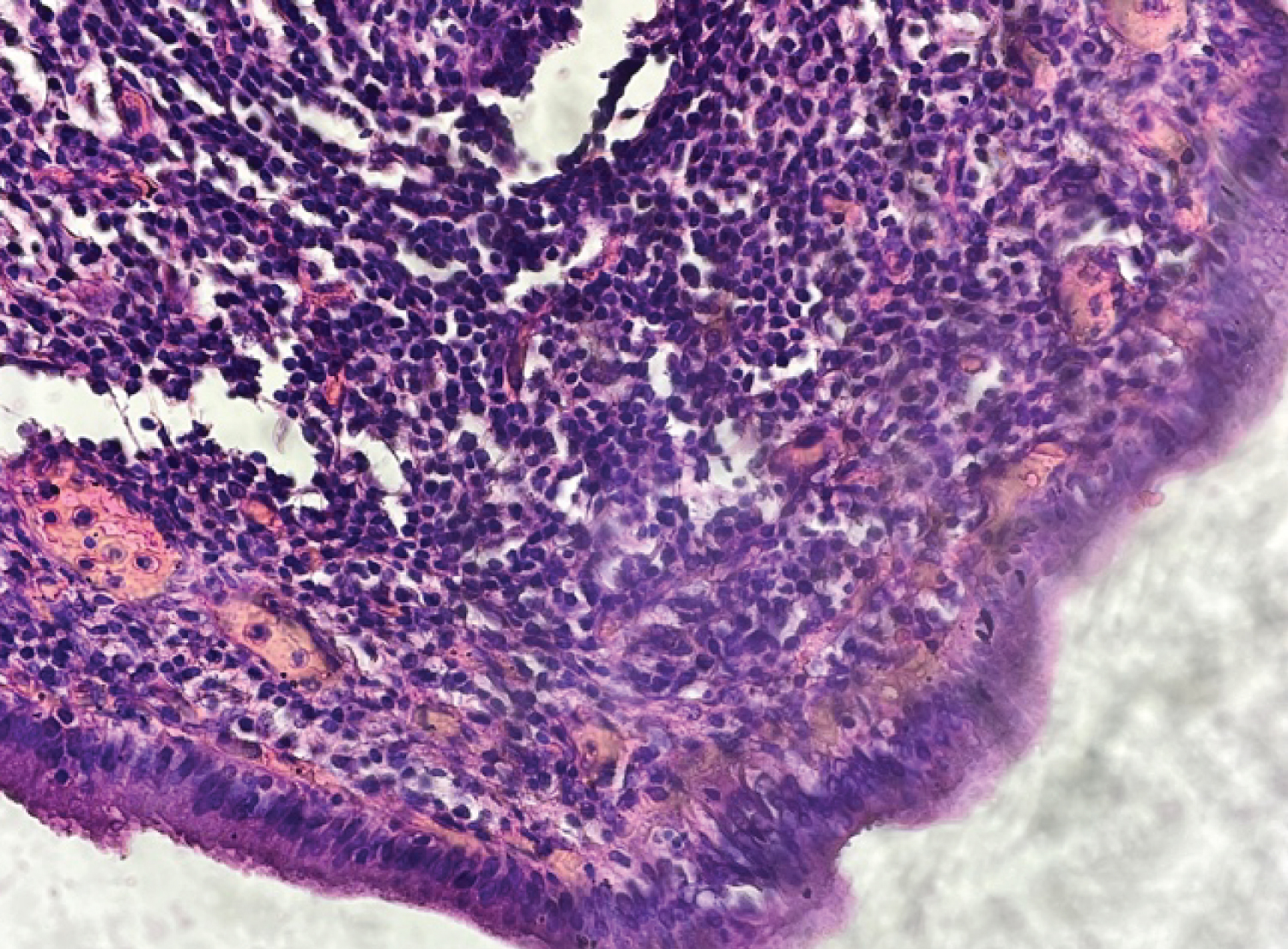 Figure 3: Monomorphic mucosal epithelium with lymphocytes (H&E 400x).
View Figure 3
Figure 3: Monomorphic mucosal epithelium with lymphocytes (H&E 400x).
View Figure 3
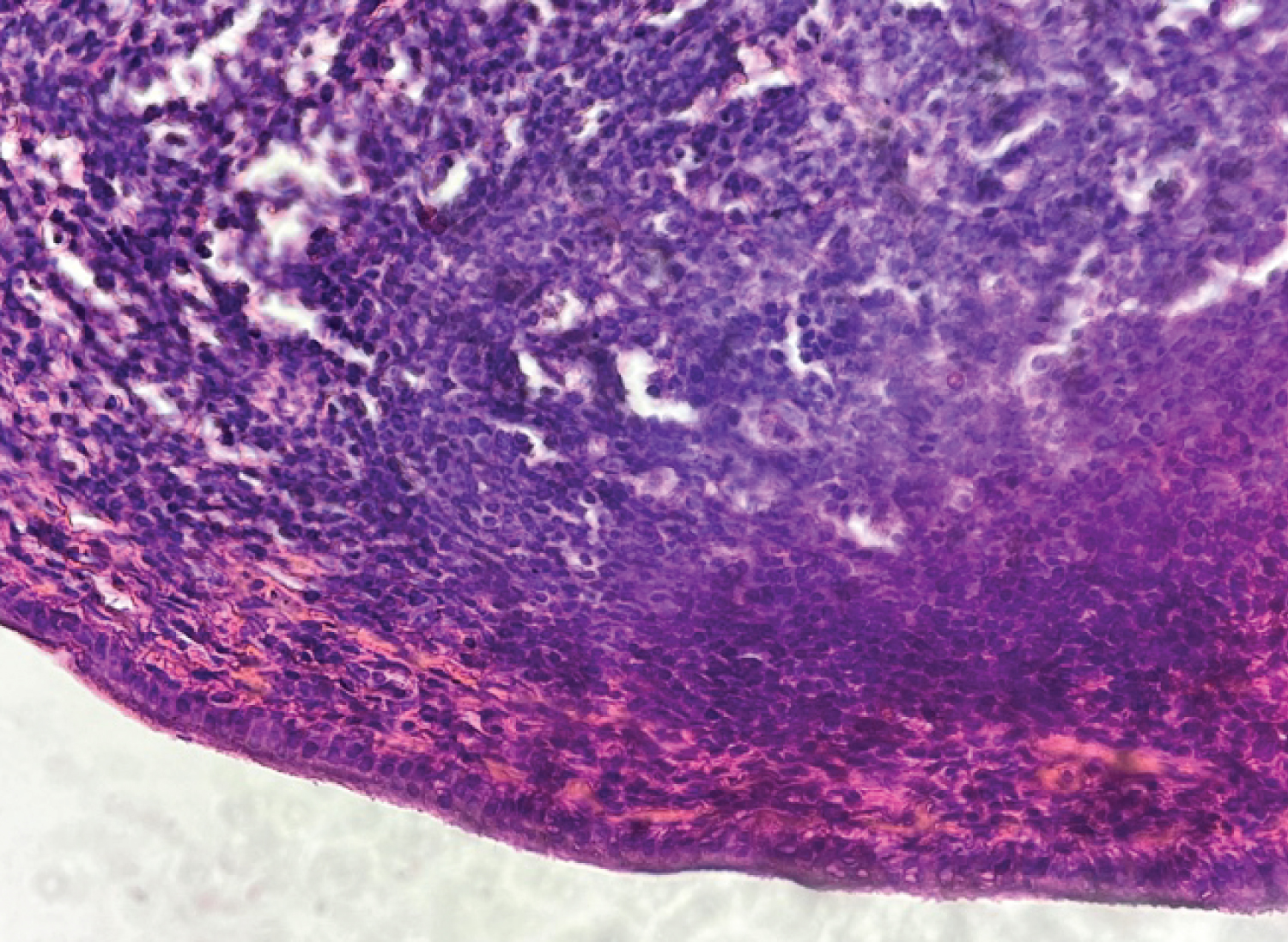 Figure 4: Cellular lymphoid infiltrate (H&E 400x).
View Figure 4
Figure 4: Cellular lymphoid infiltrate (H&E 400x).
View Figure 4
Historically, Escherichia coli , Klebsiella pneumoniae , and Salmonella typhi infections caused by gram-negative bacteria have been linked to follicular cholecystitis [5,6]. In addition, many chronic cholecystitis patients exhibit pyloric metaplasia and detectable Helicobacter pylori infection of the gallbladder mucosa, albeit this does not seem to predict the particular histologic subtype [7,8].
It is crucial to distinguish between reactive lymphoid hyperplasia and malignant lymphoma. They frequently pass for cholecystitis. The most prevalent ones are CLL/SLL, follicular lymphoma, mantle cell lymphoma, and mucosa associated lymphoid tissue (MALT) lymphoma [9]. Gallbladder MALT lymphoma is described as having diffuse infiltration of cells that resemble tiny follicular cells, a significant number of plasmocytes, and lymphoid cell invasion of epithelium. It differs from the reactive changes [10]. The limitations of this study were the lack of bacterial culture data and no immunohistochemical examination to rule out malignancy.
This case was used to highlight the rarity of follicular cholecystitis. It is a benign and extremely uncommon entity that frequently looks like lymphoma. FC does not seem to be associated with autoimmunity, lymphoma, or obstructive pathologies.
This case report was prepared with the support of all Bethesda Hospital Anatomic Pathology laboratory staff.
There is no conflict of interest in preparing this case report.