Sickle cell anemia is the most common abnormality of the red cell. The clinical manifestations of SCD are mostly related to hemolytic anemia, hypersplenism, and Vaso-occlusion, which can lead to acute and chronic pain and tissue ischemia or infarction. Disseminative or primary invasive infections such as histoplasmosis can masquerade in splenomegaly resulting in multiple hospital visits for acute splenic crises, causing increased morbidity and mortality. This case would increase our index of suspicion for invasive Splenic fungal infection in a sickle cell patient, especially with recurrent abdominal pain and hepatosplenomegaly as well as its management. Such patients have been erroneously labeled as narcotic seeking, owing to multiple Emergency Department (ED) visits for recurrent symptoms.
A 40-year-old African American female with a history of sickle cell disease with frequent emergency room visits for abdominal pain, hepatosplenomegaly with calcification per CT, type 2 DM, hypertension, and obesity, presented to the ED with abdominal pain following a physical assault. She was found to have hemoperitoneum, from a splenic laceration on abdominopelvic CT imaging. She had emergent exploratory laparotomy and splenectomy. While being managed in the intensive care unit (ICU) for Acute hypoxic respiratory failure from acute chest syndrome and Hyperosmolar Hyperglycemic State, developed persistent fever with leukocytosis, and was started on empirical broad-spectrum antibiotics while awaiting blood cultures. The patient's post-Op repeat CT showed nothing concerning the source of sepsis. Post-op splenic tissues pathology report revealed necrotizing granuloma with fungal yeast suggestive of Histoplasma. Blood bacteria, fungal culture and HIV tests were negative. CT chest with contrast was negative for granulomatous disease. The patient was subsequently started on oral itraconazole for diagnosis of invasive histoplasmosis infection by the Infectious disease (ID) specialist. The patient had significant clinical improvement after 4 days of antifungal therapy. She was discharged to complete antifungal therapy, with outpatient infectious disease and hematology follow-up.
The Sickle cell crises account for most of the ED visits in SCD patients and could cause anchoring bias, clouding suspicion for some rare indolent or chronic splenic infections. Infection is the major cause of morbidity and mortality in patients with SCD. Histoplasmosis, as in this patient, may cause chronic invasive splenic infection and may be difficult to differentiate from acute splenic crisis, in view of the low clinical suspicion for histoplasmoma infection involving the spleen. This case is unique as no case of invasive histoplasmosis of the spleen in a sickle cell anemia patient has even been reported. Also, histoplasmosis of the spleen with no lung involvement is very rare. Splenic histoplasmosis (non-pulmonary) should be considered in sickle cell disease patients with recurrent abdominal pain and hepatosplenomegaly evidence on CT, especially those immunosuppressed with other chronic illnesses such as uncontrolled diabetes (Figure 1 and Figure 2). Early diagnosis and treatment of histoplasmosis in sickle cell anemia patients can decrease the risk of Overwhelming Post Splenectomy Infection (OPSI) and mortality. Preventing OPSI with early and timed immunization should be emphasized. This case opens a question as to if sickle cell disease should be considered a risk factor for disseminated histoplasmosis [1-3].
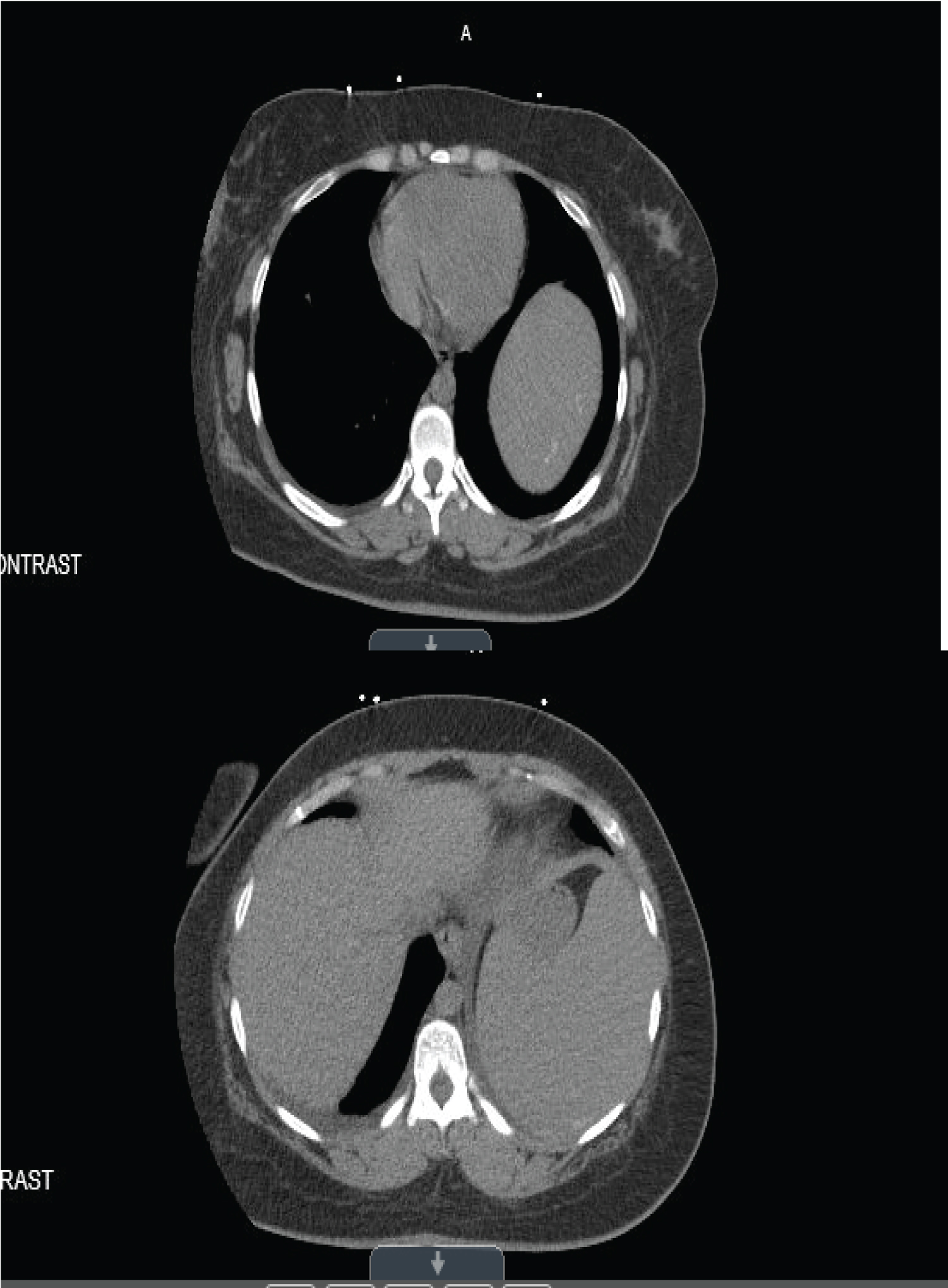 Figure 1: Hepatosplenomegaly.
View Figure 1
Figure 1: Hepatosplenomegaly.
View Figure 1
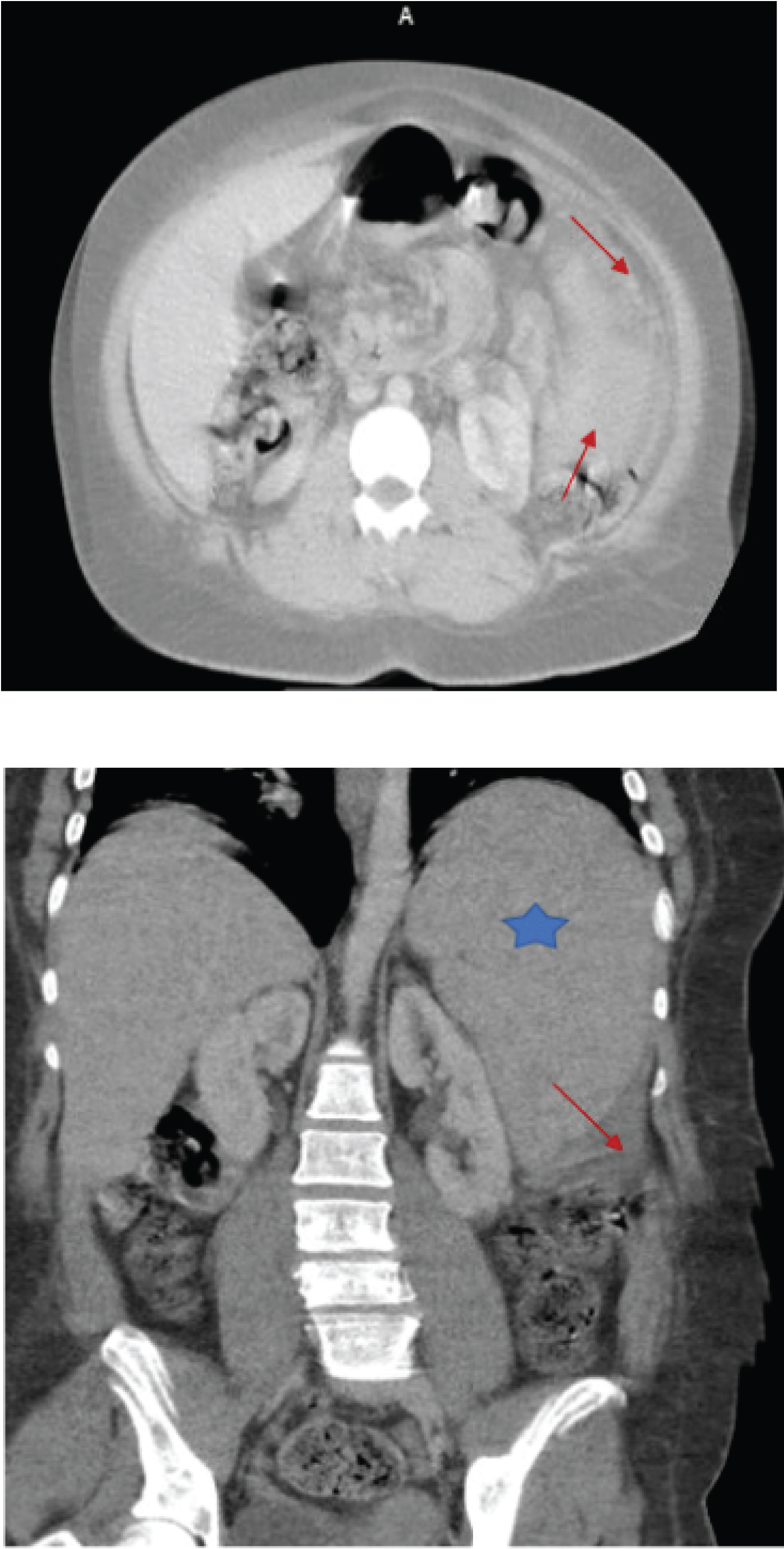 Figure 2: Traumatic splenic rupture.
View Figure 2
Figure 2: Traumatic splenic rupture.
View Figure 2