Introduction: Percutaneous stenoscopy lumbar decompression (PLSD) is a minimally invasive procedure to treat herniated nucleus pulposus (HNP). The most common and dangerous complication of this procedure is cerebrospinal (CSF) leakage. If there is an undetectable small tear in the dura during surgery or known as an occult dural tear (ODT), it can lead to a delayed CSF leakage.
Case report: A 48-year-old woman complained of lower back pain since 2 months ago. The patient had a history of PSLD 3 months ago due to HNP, 6 days after surgery, the patient felt headache, nausea, vomiting, and fainting. Lumbosacral MRI results revealed a posterior sacral pseudomeningocele and CSF herniation from the defect. The patient underwent open repair surgery, she was hospitalized for 5 days and was discharged without neurological deficits, complaints of headache and lower back pain disappeared.
Discussion: Delayed cerebrospinal fluid leakage can cause complications in the form of intracranial hypotension which can be dangerous and must be diagnosed and treated immediately. MRI is the gold standard examination in this case. The neurosurgeon decided to perform open repair surgery to identify the defect and close it using the overheating technique. Consideration of open repair surgery in this patient is done in order to get a wider field of view to close the defect.
Conclusion: Although the incidence of ODT after PSLD is very rare, further investigation needs to be carried out in patients who experience headaches, vomiting and fainting after PSLD procedures. Operator experience in performing minimally invasive procedures also plays a role. Multilevel suture during open repair surgery prevents recurrence of CSF leakage.
Cerebrospinal leakage, Occult dural tear, Spine surgery, PSLD, Complication
Lower back pain is a very common complaint worldwide, at least 80% of the population has experienced it [1]. One of the most common causes of low back pain is HNP. HNP is a condition where there is a protrusion of the nucleus pulposus through the annulus fibrosus of the intervertebral disc causing compression of the nerve roots, 95% of HNP is located in the L4-L5 or L5-S1 lumbar region and is one of the most common indications for spinal surgery worldwide [1-3].
The prevalence of lumbar disc herniation is quite high, namely 5 out of 20 cases per 1000 adult cases per year, and is most often found in the third to fifth decades of life [4]. Epidemiological data regarding HNP in Indonesia do not yet exist, but the incidence of HNP based on patient visits to several hospitals in Indonesia ranges from 3-17% [2].
Treatment of HNP consists of conservative and surgery. Conventional surgery for HNP is open laminectomy discectomy, while the latest minimally invasive surgery is Percutaneous stenoscopy lumbar decompression (PLSD). PLSD optimizes the endoscopic system to perform laminectomy, discectomy, foraminotomy, and flavectomy in cases of lumbar stenosis [5]. Minimally invasive surgery has been widely performed in the last 20 years. When compared to conventional surgery, minimally invasive surgery has a shorter operating time, less blood loss, and lower infection rates [6,7]. However, minimally invasive surgery is associated with a high complication rate and a lot of experience is required before the surgeon becomes familiar with this technique [8]. The most common complication of this procedure is CSF leakage, there are several case reports of delayed CSF leakage due to undetected small dura tears at the time of surgery, or what is called an occult dural tear further can lead to intracranial hypotension and infections such as meningitis [9].
Minimally invasive or endoscopic lumbar surgery has a higher risk of tearing the dura when compared to open surgery, which is about 1-6%. This may be because all structures are not visualized when performing this procedure. In addition, tearing is more common in elderly patients and operators have less experience [10].
Here we present an interesting case of complication of PLSD that we found in our institution and the treatment of that complication.
A 48-year-old woman came to the hospital with complaints of lower back pain since 2 months ago. The pain was felt radiates to the lower limbs accompanied by a stabbing feeling, the pain was felt intermittently, the pain worsens at night especially when sitting and sleeping in a soft place, and the pain was reduced when the patient stands up. The patient had a previous history of PSLD surgery at another hospital 3 months ago due to HNP (Figure 1). 6 days after surgery, the patient felt headache, nausea, vomiting, and fainting. Normal bowel and bladder, no history of trauma. On physical examination, there were no lumps in the lumbar spine, motoric and sensory was normal.
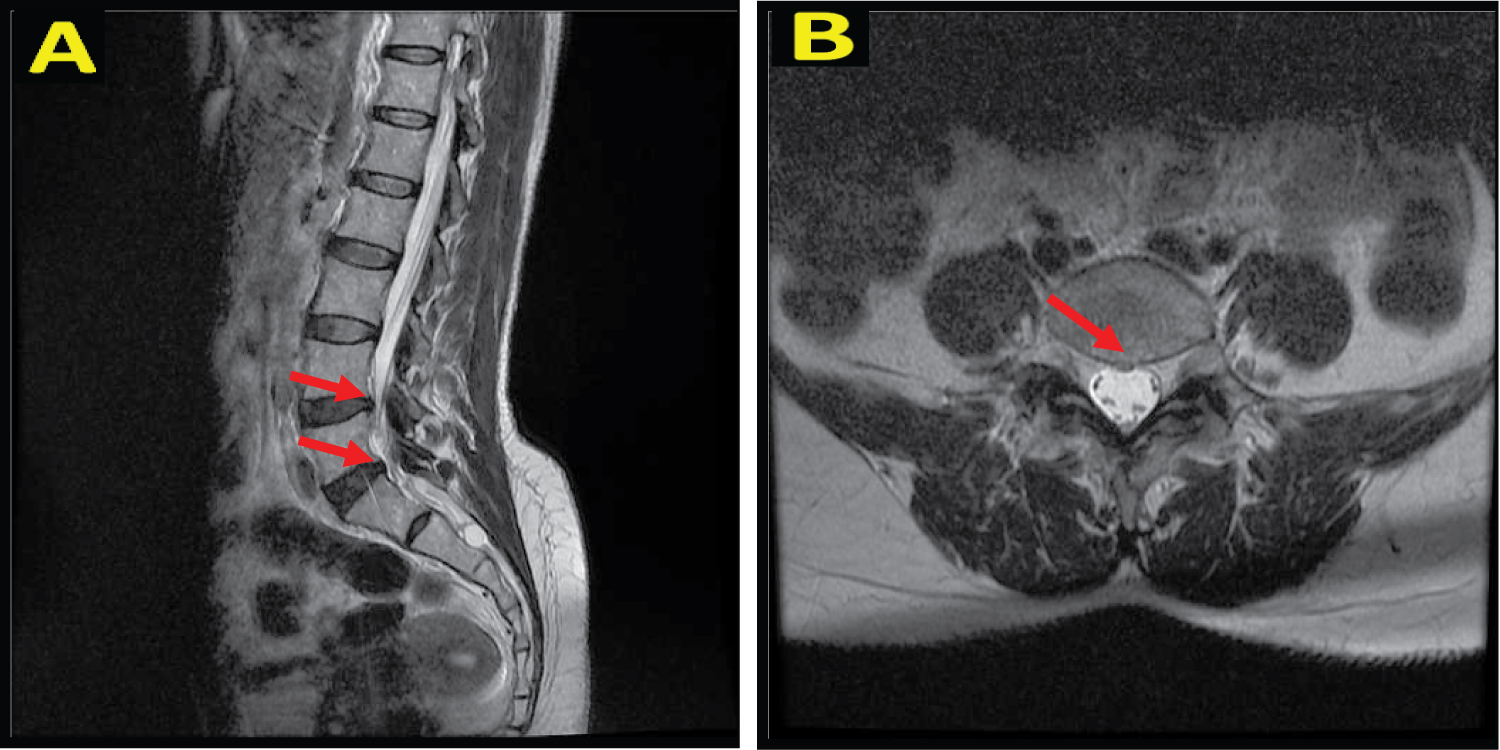 Figure 1: A) Sagittal T2 MRI image shows protrusion of the intervertebral disc at L4-L5 and L5-S1 levels; B) Axial T2 MRI image shows protrusion of the intervertebral disc at L5-S1 level towards the posterior central.
View Figure 1
Figure 1: A) Sagittal T2 MRI image shows protrusion of the intervertebral disc at L4-L5 and L5-S1 levels; B) Axial T2 MRI image shows protrusion of the intervertebral disc at L5-S1 level towards the posterior central.
View Figure 1
The patient underwent a MRI lumbosacral without contrast and a pseudomeningocele appeared in the posterior sacral region. The MR myelography showed no stenosis, and CSF herniation from a defect at the level of CV S1 was seen (Figure 2). The patient then underwent open repair surgery. During the operation, the patient was in a prone position under general anesthesia, a linear incision in the lumbosacral region was made 12 cm long, and a cystic mass appeared in the subcutis area. Then, we freed the cyst wall from the surrounding tissue, cut the cyst wall, and clear CSF fluid came out of the 1 cm defect. The defect was closed by overhecting the dura mater and fascia, then a fibrin glue was applied (Figure 3). Next, the neurosurgeon performed sutures to the muscle, fascia, subcutis, and skin.
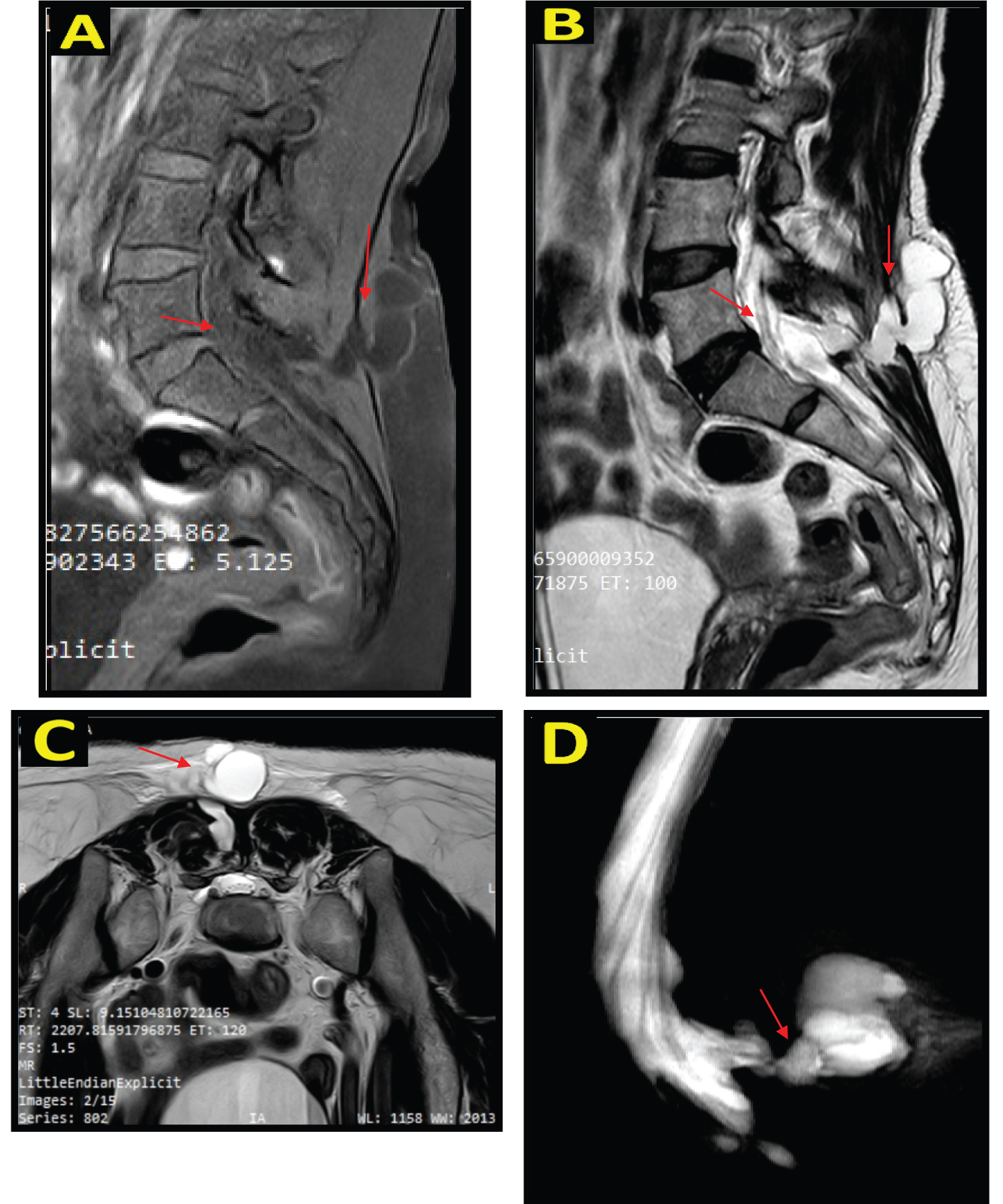 Figure 2: Non-contrast lumbosacral MRI image on sagittal section, hypointense lesion on T1WI (A), and hyperintense on T2WI (B). On T2W1 axial view, posterior to CV L5, relatively firm borders, regular margins, with a diameter of +/- 4.4 cm, The impression comes from a defect in the spinal cord at the level of CV S1 (C). On MR Myelography, no stenosis was seen and CSF herniation is seen from a defect at the level of CV S1 (D).
View Figure 2
Figure 2: Non-contrast lumbosacral MRI image on sagittal section, hypointense lesion on T1WI (A), and hyperintense on T2WI (B). On T2W1 axial view, posterior to CV L5, relatively firm borders, regular margins, with a diameter of +/- 4.4 cm, The impression comes from a defect in the spinal cord at the level of CV S1 (C). On MR Myelography, no stenosis was seen and CSF herniation is seen from a defect at the level of CV S1 (D).
View Figure 2
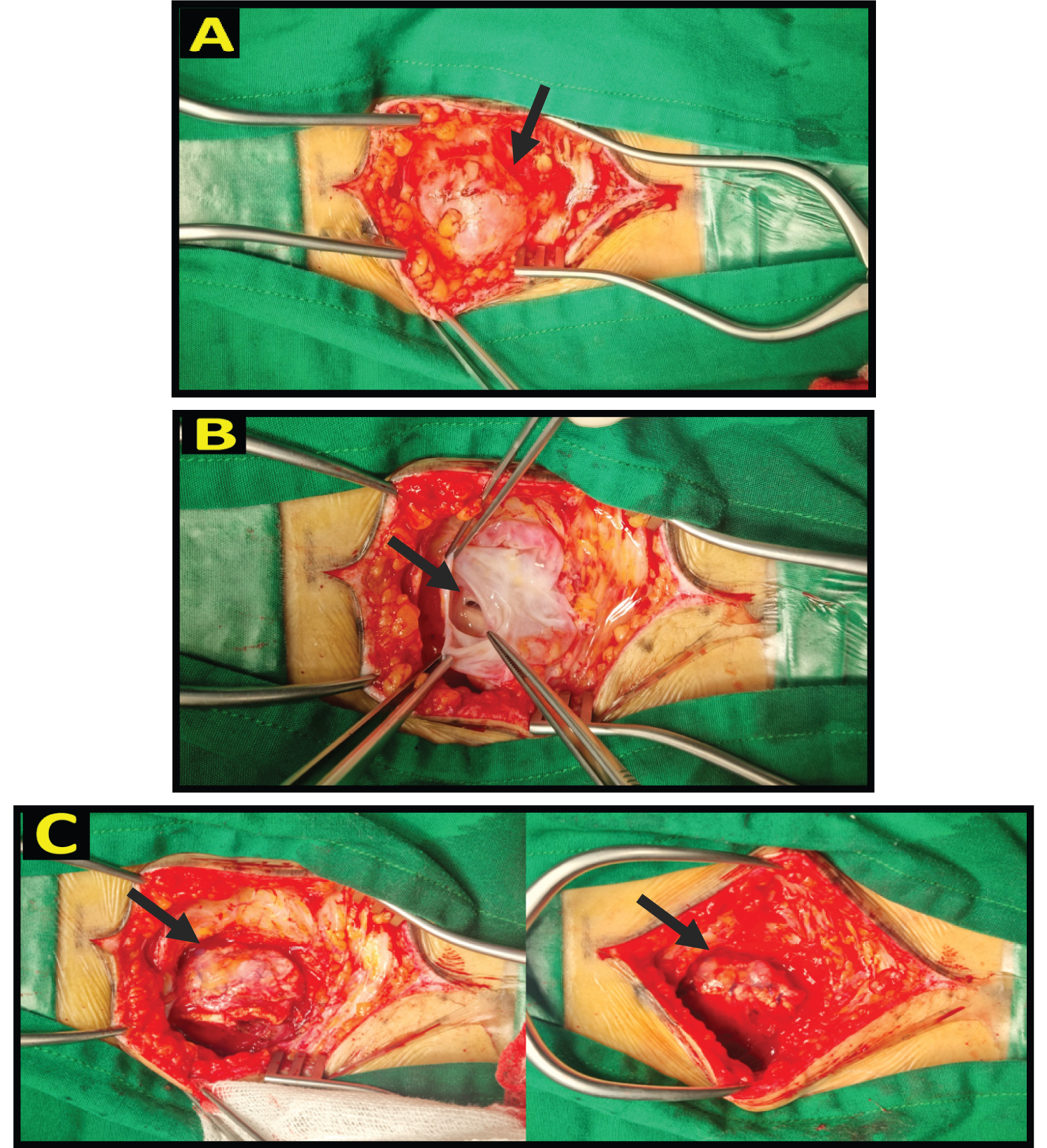 Figure 3: There was a mass measuring ± 4.5 cm with positive fluctuations in the impression of a cyst (A), the cyst wall was freed from the surrounding tissue and then excised, clear CSF came out, and the defect was detected with ± 1 cm in size (B). The defect was closed by overhecting the dura mater then the fascia and fibrin glue was applied (C).
View Figure 3
Figure 3: There was a mass measuring ± 4.5 cm with positive fluctuations in the impression of a cyst (A), the cyst wall was freed from the surrounding tissue and then excised, clear CSF came out, and the defect was detected with ± 1 cm in size (B). The defect was closed by overhecting the dura mater then the fascia and fibrin glue was applied (C).
View Figure 3
After surgery, the patient was admitted to the ward, and given acetazolamide, an antibiotic, and analgesic. The patient was hospitalized for 5 days and then discharged without a neurological deficit. The complaints of headache, back pain, and stabbing legs disappeared. Patients are educated not to take actions that can increase intracranial pressure such as straining, lifting heavy weights, coughing, and sneezing.
Treatment of HNP cases continues to develop, the latest minimally invasive surgery is percutaneous stenoscopic lumbar decompression (PLSD). PLSD optimizes the endoscopic system to perform laminectomy, discectomy, foraminotomy, and flavectomy in cases of lumbar stenosis [5].
The most common complication of lumbar spine surgery is CSF leakage. Although neurosurgeons have given special attention to this complication, it is still unavoidable [9]. According to the data, the incidence of CSF leakage after spine surgery is 2-20% [11]. Minimally invasive or endoscopic lumbar surgery has a higher risk of dural tears when compared to open surgery, which is about 1-6%. This may be because all structures are not visualized when performing this procedure. In addition, dural tears are more common in elderly patients and operators have less experience [10].
The delayed or not treated properly of CSF leak will lead to pseudocyst formation, intracranial hypotension, infection, and even death. The most serious complication of CSF leak is meningitis, which is about 19% and patients will still be at risk until successful closure of the defect [11,12].
Delayed CSF leakage is a condition in which the patient does not feel any complaints of intracranial hypotension after surgery and does not find any dural tears at the time of surgery. The etiology is still unclear, but there are 3 allegations, (1) There is weakness in the dura or an incomplete dura tear which then becomes a complete tear when the complaint of severe headache appears, (2) The dura tear is present at the time of surgery but the CSF leak has not occurred because it is still in the subfacial layer, and (3) The increase of CSF pressure due to physical activity causes erosion of the dura due to the dura being exposed to sharp angles from the decompression site [13].
In this case, the patient suddenly complained of headache, nausea, vomiting, and fainting on the 6 th day after PSLD surgery, this may be due to intracranial hypotension. Undetected small dural tears can cause symptoms in less than 6 days, but there are cases where symptoms appear late, starting to appear above 5 days after surgery. These complaints generally occur suddenly [13].
According to the Monro-Kellie doctrine, CSF leakage will reduce the pressure so that it can cause venous dilatation, which causes meningeal traction and subdural effusion, as well as hematoma through rupture of bridging veins causing headaches. Type of headaches can vary, sometimes in severe cases, there can be orthostatic unconsciousness due to diencephalic herniation. Symptoms of nausea and vomiting occur in 50% of cases of intracranial hypotension. Neck stiffness, diplopia, photophobia, facial pain or numbness, paresthesia of limbs, dementia, and behavioral disturbances have been reported. Less common complaints of radiculopathy and myelopathy may also occur, this is due to compression of the extradural fluid or dilation of the venous plexus [14,15].
MRI is a sensitive and noninvasive modality for detecting CSF leakage. On MRI, extradural CSF is seen in several vertebral segments. On MR angiography, the location of the CSF leak is seen clearly. Therefore, non-contrast MRI of the vertebrae is the first diagnostic imaging in patients with suspected CSF leak and orthostatic headache [16].
In this case, Consideration of open repair surgery in this patient is done to get a wider field of view to close the defect. Failure to close the dura with primary hecting ranges from 5-9%. It is recommended to perform a primary suture on a small dura tear or small defect using a continuous suture or 8 figure suture technique. The thread should be 4.0-6.0 in size with a distance of < 3 mm between the 2 sutures and 1 mm from the margin. However, for minimally invasive spine surgery, traditional threads are not used. In large dural tears or large defects, patches should be applied using fat, muscle, or fascia. Fat patches have a good water sealant if muscle patches cannot be used. This can provide the advantage of revascularization, preventing scarring and not sticking to nerve tissue. It is essential to perform sutures by layers of the paraspinal muscles necessary to remove dead space to effectively prevent minor dural tears [17]. The sharp bones should be removed adequately by laminotomy. The use of a dural sealant and bed rest for 24-48 hours after surgery is also recommended [13].
Although the incidence of ODT after PSLD is very rare, further investigation needs to be carried out in patients who experience headaches, vomiting and fainting after PSLD procedures. Operator experience in performing minimally invasive procedures also plays a role. Multilevel suture during open repair surgery prevents recurrence of CSF leakage.