The purpose of this review article is to showcase the importance of neurosurgical care in third world countries, including the lack of support and awareness among developed countries on this issue.
A summary of available data on neurosurgical mission trips has been collected from PubMed and Google Scholar on the following mesh keywords: Neurosurgery trips, mission neurosurgery, and neurosurgery in third world countries. We gathered our information that was closely related to neurosurgical education such as proficiency, equipment, ethics and outcomes (Figure 1).
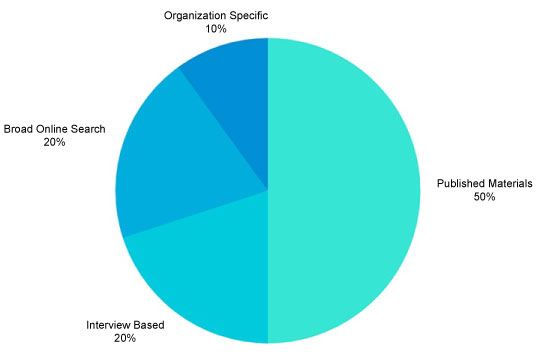 Figure 1: Visual representation of acquired data on neurosurgical capacity in low and middle-income countries. View Figure 1
Figure 1: Visual representation of acquired data on neurosurgical capacity in low and middle-income countries. View Figure 1
The neurosurgical workforce in third world countries is still scarce as awareness on the lack of specialized surgical care is still underdeveloped worldwide. In addition to the lack of neurosurgeons, the unavailability of specialized equipment is still one of the main concerns of visiting neurosurgeons.
The analyzed summary on the role of neurosurgeons in third world countries showcased improved surgical skills for neurosurgeons themselves, and proved to be a positive indicator on the improvement of healthcare worldwide.
Neurosurgery mission trip, Global neurosurgery
Neurosurgery is a very complex, yet expensive surgical specialty that treats millions of patients who suffer from illness of the nervous system worldwide. To become a board-certified neurosurgeon in the United States and North America, it takes 7 years of rigorous residency and craftsmanship of this specialty. Only the brightest and top performing students are matched into this competitive specialty every year, in order to become leaders of tomorrow's neurological surgery field. However, regardless of the output of neurosurgical education, to this day - a demand for treatment for neurosurgical patients in the world still remains high; and unfortunately the proportion of available neurosurgeons to patients almost always supersedes the demand. This trend is especially prevalent in the third world and low-income countries, where access to these specialists requires a substantial amount of money or sometimes-even a long distance relocation to a major city [1].
The lack of basic surgical care in low-income countries causes mortality of the population up to three times more than AIDS, malaria, and tuberculosis combined together. Unfortunately, surgical needs in those countries haven't been properly addressed in the decision maker's meetings, nor has it been brought to light in the media - as much as malaria, Ebola, and HIV did in the past. This issue raises a huge concern for population desperately seeking surgical care in the hands of those who can volunteer and sacrifice their precious time to help them [2,3]. Currently, there are several issues with global neurosurgery access:
It hasn't been addressed widely in the research publications of epidemiologists, who are conducting health research in third world countries rampant with low income.
Certain countries don't have adequate neurosurgery programs, which can do a lot to prepare a future generation of neurosurgeons.
Neurosurgery as a specialty requires a special operating room, instruments and technology to conduct safe and proper neurosurgical procedures.
All the mentioned above points paint a great picture of why low-income countries still struggle with high rates of neurosurgical mortality.
As mentioned earlier, the demand for neurosurgery in the developed countries is very high and it estimates roughly 1:61,000 (neurosurgeon per population ratio), however neurosurgical workforce in the underdeveloped countries at large estimates 1:10,000,000 [4,5]. This sad statistic showcases an urgent intervention and the support of the numerous hard-working surgeons in low-income countries. Even with the presence of some neurosurgical capability in the country, the rate of inadequately treated traumatic brain injuries and neurological malformations still remains high.
What concerns of neurosurgical sub-specialty in particular, it's practically non-existent, as the majority of general neurosurgeons are left to treat the neurological disease with the little knowledge they received either in the educational institution or from the available publications in that particular region. It's also very interesting to note that due to the shortage of even general neurosurgeons in low-income countries, general surgeons on call do most of the non-complicated neuro-trauma procedures. While many underserved general surgeons can provide simple procedures such as trauma epidural or subdural hematoma evacuation, their knowledge and skills simply can't be compared to that of a well-trained neurosurgeon.
To date, The Lancet Commission on Global Surgery that was established in 2013, provided excellent, but at the same time unnerving statistics. The commission stated that more than 5 billion people worldwide still don't have access to safe and affordable surgical care. As a result, roughly 18.6 million people die due to lack of basic surgical care, which is alarmingly triple the number of deaths caused by AIDS [3].
Within a vocal and evidence based need of immanent neurosurgical care worldwide, North America and the majority of the developed countries started carrying out missionary trips with academic neurosurgeons of major hospitals on board. The average length of the trip typically lasts between a 2 weeks to a month and consists of neurosurgeons with a broad variety of specialties to address diseases such as hydrocephalus, spine deformities, cerebrovascular malformations, tumors and trauma [6]. Upon arrival to the given destination, neurosurgeons not only adapt to the local environment, but also hold grand rounds and educational seminars, in order to educate local neurosurgeons on the latest techniques and guidelines that can heavily improve patient outcomes in the future. To date, there are more than 50 non-profit organizations in the United States, which focus solely on the improvement of neurosurgical diseases in low-income and third world countries. Most of those organizations were founded and funded by active neurosurgeons who participate in the missionary trips mentioned above.
A missionary trip on average holds 10 to 32 surgeries per week, depending on the volume of admitted patients and complexity of procedures needed in the given hospital. Besides the smooth operating procedures, many visiting neurosurgeons should also adapt to minimalism of surgical instruments and medico-cultural competency of the receiving country's staff.
Every neurosurgical mission trip regardless of country of origin holds 5 main components:
Every attending or resident who participates in the missionary trip, presents an incredible value of teaching to the local neurosurgical community, which creates a great bond for further partnership with the local surgical staff.
Mentorship in neurosurgery worldwide has a tremendous value not only for young neurosurgeons, but also for academic professionals. Consulting on neurosurgical cases and direct observation of the procedures, allows visiting surgeons to guide the steps of the operation from the beginning to the end. Additionally, international mentorship helps local physicians develop a diverse set of skills, which they may have never been exposed to before; and it further opens the gates for the next level of neurosurgical development.
Any neurosurgical missionary trip requires a set of specialized instruments that might not be available at the receiving country. Therefore, teams of local neurosurgeons almost always provide a capacity based checklist on what they have and what they are missing. This checklist allows traveling neurosurgical teams to thoroughly prepare their traveling luggage and sometimes even obtain a clearance for the security purposes. The most needed neurosurgical instruments in low and middle-income countries are:
• Electric craniotomes
• Horse shoe head rest
• Mayfield clamps
• Perforators & Drills
• Titanium plates
• Micro instruments
• Ventricular shunt hardware
• Spinal implants
• CT and MRI scanners [7].
Partnership is what makes all mission trips unique. This special partnership that is formed during a given trip, allows adoption and further development of academic grounds between two healthcare systems and long term post-follow up care [8,9]. While there is still a stigma in regards to the lack of post-follow up care of visiting surgeons, modern physicians widely adapt mobile technology for videoconferences to address any post-operating questions or complications remotely [10].
A thorough preparation and execution of a successful missionary trip requires substantial funding. All the funds for living and airfare expenses must be included ahead of a time. As mentioned earlier in the article, most of the neurosurgical volunteer organizations hold 501-C status as a non-profit medical organization. This status allows surgical trip organizations secure donations from private or public donors and become tax exempt from any mission related business spending.
Additionally, besides of those top five major points, local medical and non-medical volunteers and location guides should be involved as well, as multicultural competency and language barriers can create an unprecedented obstacle.
According to numerous articles, neurosurgeons who engaged in the missionary work showcased a great satisfaction about the trip not only professionally but also personally. Most of the neurosurgical teams described their creativity and teamwork in the situations they had never come across before. These kinds of scenarios not only provide a competency for modern physicians, but also a critical thinking and academic advocacy for the underserved areas. The more neurosurgical professionals that are involved in the mission of improving unprivileged healthcare worldwide, the better advocacy and outcome we can expect in the near future. Further investigation on efficacy and improvement of neurosurgical trips to the third world countries is strongly indicated.
The consent for publication is not applicable for this review article.
Authors declared no competing interests to declare.
Data sharing is not applicable for this review article.
Funding is not applicable to this study.
Author would like to acknowledge the contributing neurosurgeons who are actively involved in improving neurosurgical care worldwide.
The approval and consent is not applicable to this study.