The principle of the middle cranial fossa MCF approach is to expose the entire length of the internal auditory canal via an extradural approach while preserving the auditory and facial function.
It was described by Perry in 1904 [1] to perform a neurotomy in a patient suffering from a Menière's disease. It was subscribed because of the very serious postoperative morbidity. William House in 1961 [2] using microsurgical techniques was able to describe the details of this approach which he used to operate on small vestibular schwannomas and disabling vertigo by performing vestibular neurotomy.
The MCF approach was indicated in:
- Patient under 65 years of age,
- Vestibular schwannoma < 20 mm in cases when hearing preservation is being con- sidered (Functional or useful hearing: > 50% speech discrimination score),
- Vestibular neurotomy for Ménière's disease.
The MCF approach was contraindicated in:
- Patient over 65 years of age due to fragility of the dura mater,
- Vestibular schwannoma larger than 1.5 cm in the pontocerebellar angle.
Long-term muscle relaxants should be avoided during the induction of anesthesia and intubation, as these may interfere with facial nerve electromyography.
The patient is placed in the supine position with the head turned to the side opposite the lesion (Figure 1). The head is turned such that the index ear is facing up and the side of the skull is as parallel to the floor as possible [3]. Care should be taken to avoid forcing the neck to turn to prevent injury to the cervical spine and to prevent occlusion of the contralateral internal jugular vein that can impede cranial venous return.
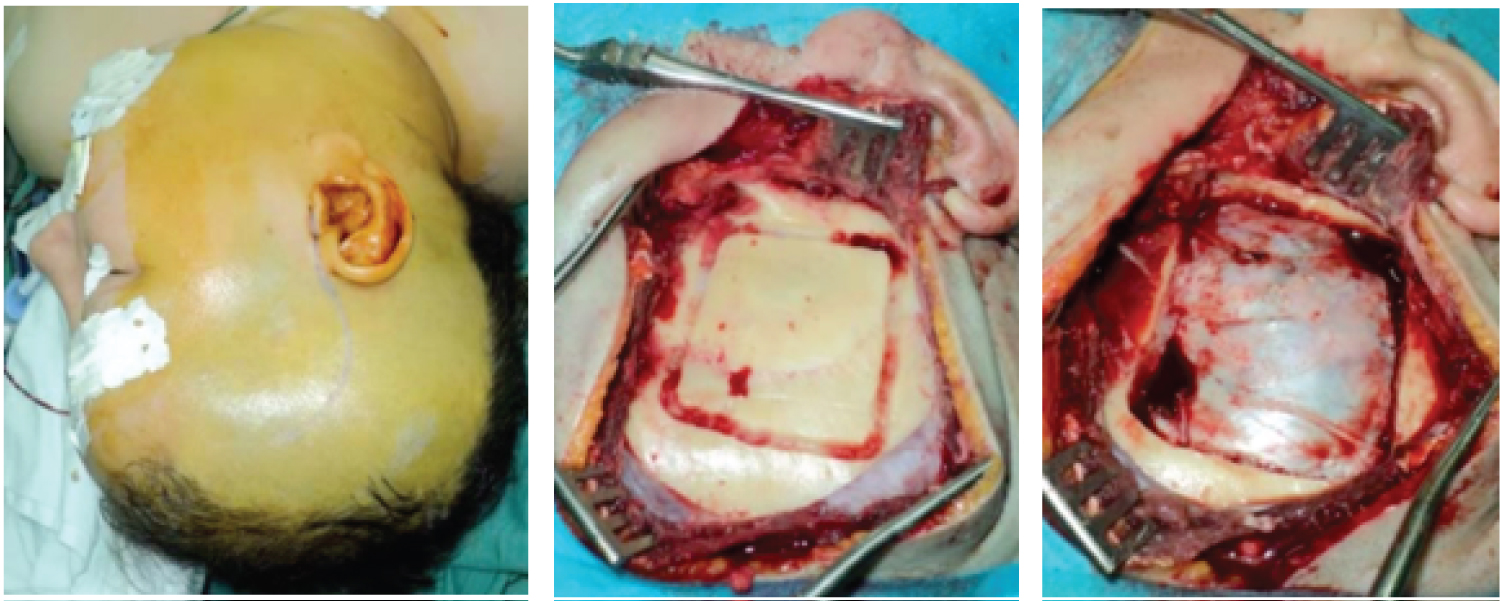 Figure 1: (a) The patient is placed in the supine position with the head turned to the side opposite the lesion and a temporofrontal skin incision in the form of a question mark was made; (b) Temporal craniotomy was performed. The root of the zygoma (RZ) was a landmark to identified the floor of MCR; (c) The inferior limit of the flap should be at the level of the floor of middle cranial fossa (white arrow).
View Figure 1
Figure 1: (a) The patient is placed in the supine position with the head turned to the side opposite the lesion and a temporofrontal skin incision in the form of a question mark was made; (b) Temporal craniotomy was performed. The root of the zygoma (RZ) was a landmark to identified the floor of MCR; (c) The inferior limit of the flap should be at the level of the floor of middle cranial fossa (white arrow).
View Figure 1
An incision is made in the preauricular area and extended superiorly in a gently curving fashion (Figure 1A). Care must be taken near the anterior extension of the incision to avoid injury to the frontal branch of the facial nerve.
Once the skin flap is elevated, the temporalis muscle is incised, beginning at the zygomatic root, along the linea temporalis, and the muscle is elevated from the temporal fossa and reflected anteroinferiorly. This exposes the temporal squama (Figure 1B).
Temporal craniotomy is performed. The root of the zygoma is identified and this landmark is used to approximate the location of the middle fossa floor [4]. The craniotomy measures approximately 5 × 5 cm and is two-thirds anterior and one-third posterior to the zygomatic root (Figure 1C). The inferior limit of the flap should be at the level of the zygoma, approximating the floor of the middle cranial fossa.
The bone flap is set aside for later replacement. Bleeding from the diploic can be controlled with bone wax. The air cells along the craniotomy edges that were opened must be obliterated with bone wax to prevent CSF leakage.
The dura is elevated from the floor of the middle fossa under the surgical microscope. The initial landmark is the foramen spinosum (Figure 2A) which is the entrance of the middle meningeal artery into the middle cranial fossa, which marks the anterior extent of the dissection. Frequently, venous bleeding is encountered from this area and can be controlled with oxidized cellulose (Surgicel). Dissection will progresse medially along the anterosuperior surface of the petrous bone until the superior border of the petrous bone is found and the superior petrous sinus (SPS) is elevated from the petrous ridge (Figure 2C). The elevation of the dura is then continued anteriorly exposing the eminence arcuate (Figure 2B) (usually indicates the position of the SSCC) and the bone surface lying in front of it for about 10 to 15 millimeters. During this elevation, the greater superficial petrosal nerve (GSPN) may come into view laterally at its exit from the bone at the facial hiatus (Figure 2C). To avoid avulsion of the GSPN from the geniculate ganglion, it is necessary to dissect it from the dura mater of the temporal lobe.
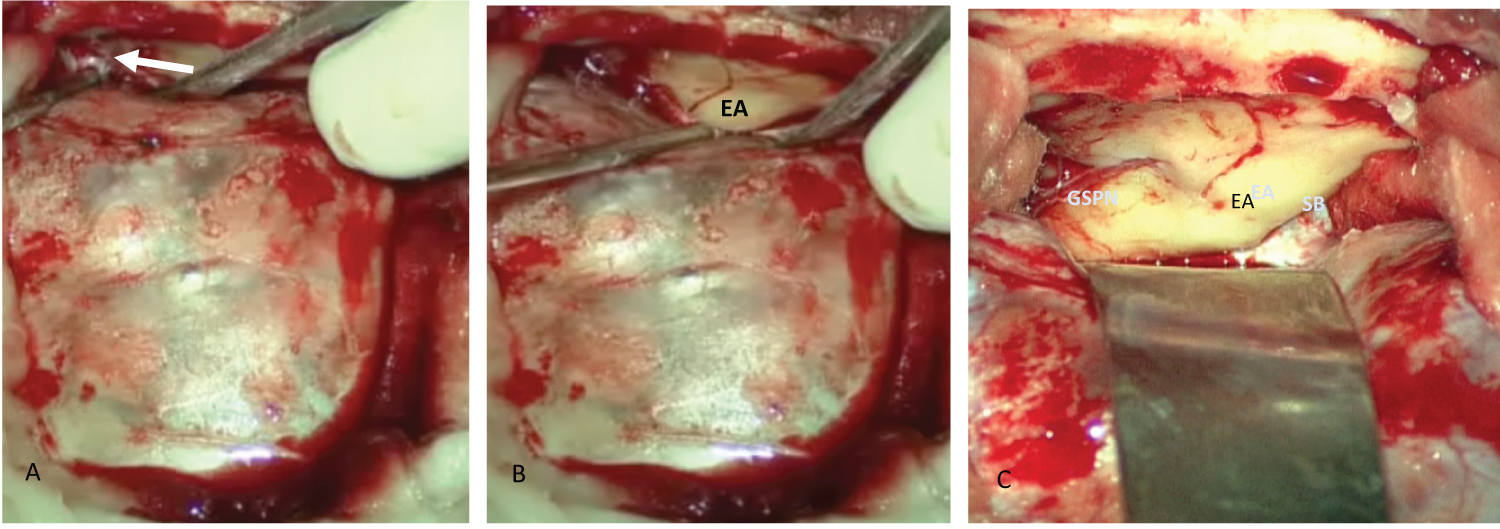 Figure 2: The different surface landmarks of the middle fossa floor. (a) The middle meningeal artery: Anterior landmark; (b) Eminence arcuate (EA); (c) Greater superficial petrous nerve (GSPN) and superior border of the petrous bone (SB).
View Figure 2
Figure 2: The different surface landmarks of the middle fossa floor. (a) The middle meningeal artery: Anterior landmark; (b) Eminence arcuate (EA); (c) Greater superficial petrous nerve (GSPN) and superior border of the petrous bone (SB).
View Figure 2
At this point, temporal lobe retractors are placed, ideally with the tips of the retractor blades resting on the petrous ridge between the arcuate eminence and the GSPN (Figure 2C).
One of the major challenges of using the MCF approach to expose IAC is that the surface anatomy of the middle fossa floor has few consistent landmarks. In this situation the use of neuronavigation finds its full indication to identify the internal auditory canal.
The non-availability of neuronavigation requires knowledge of the different techniques to identify the IAC. The eminence arcuata and GSPN are the major landmarks for identification the meatal plane (Figure 2C). Three basic methods of exposing the IAC may be used separately or in combination:
- House method (Figure 3): The great superficial petrosal nerve (GSPN) was the essential landmark. This technique consists in the identification of the geniculate ganglion and then labyrinthine segment of the facial nerve,
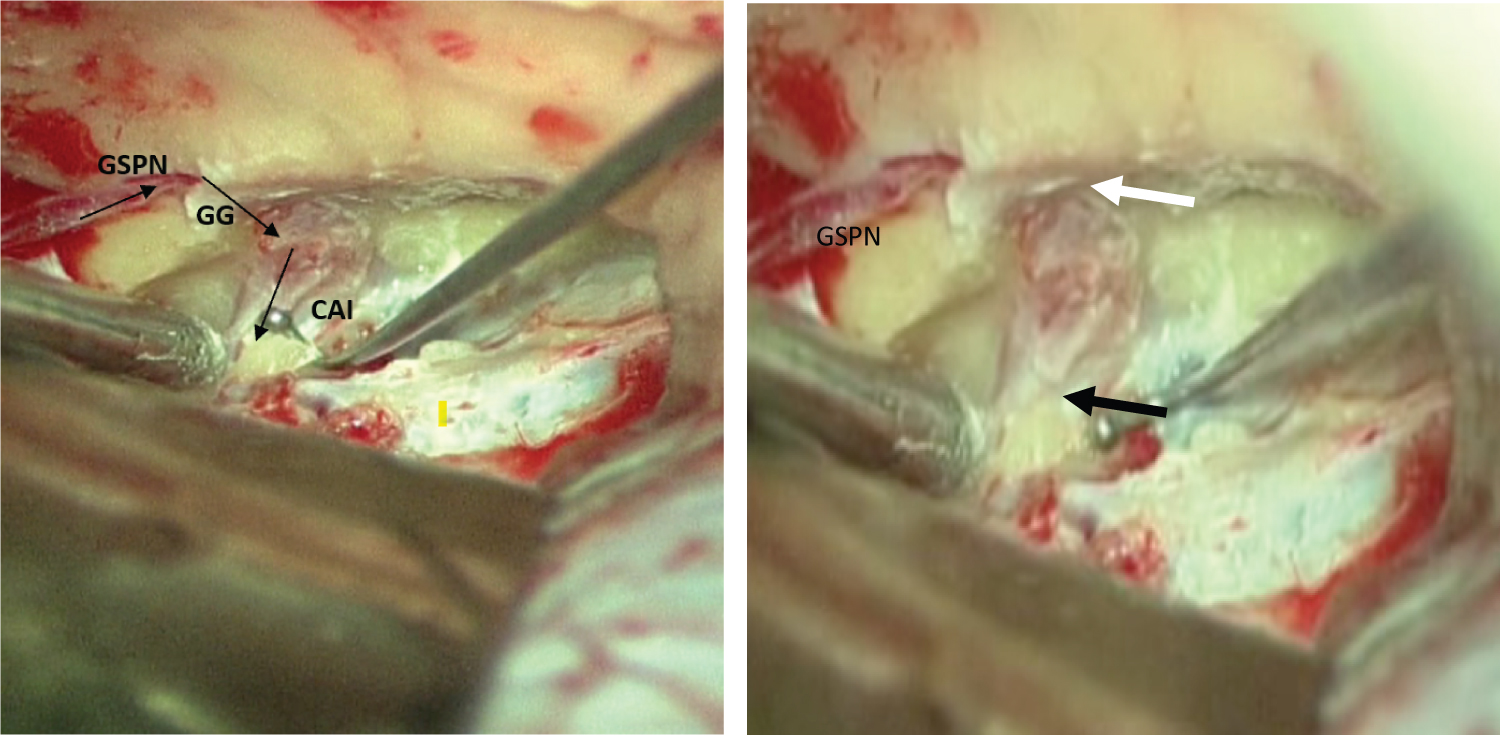 Figure 3: Identification of internal auditory canal IAC (Meatal plane) according to the William House technique. GSPN: Greater superficial petrous nerve, Black arrow: Porus, White arrow: Fundus.
View Figure 3
Figure 3: Identification of internal auditory canal IAC (Meatal plane) according to the William House technique. GSPN: Greater superficial petrous nerve, Black arrow: Porus, White arrow: Fundus.
View Figure 3
- Fisch method: In this technique the major landmark was the eminence arcuate. The meatal plane is located 60° in front of the CSCS plane.
- Garcia-Ibanez method (Figure 4): It is a rapid technique whose meatal plane is search in the bisection of the angle formed by the GSPN and the eminence arcuata.
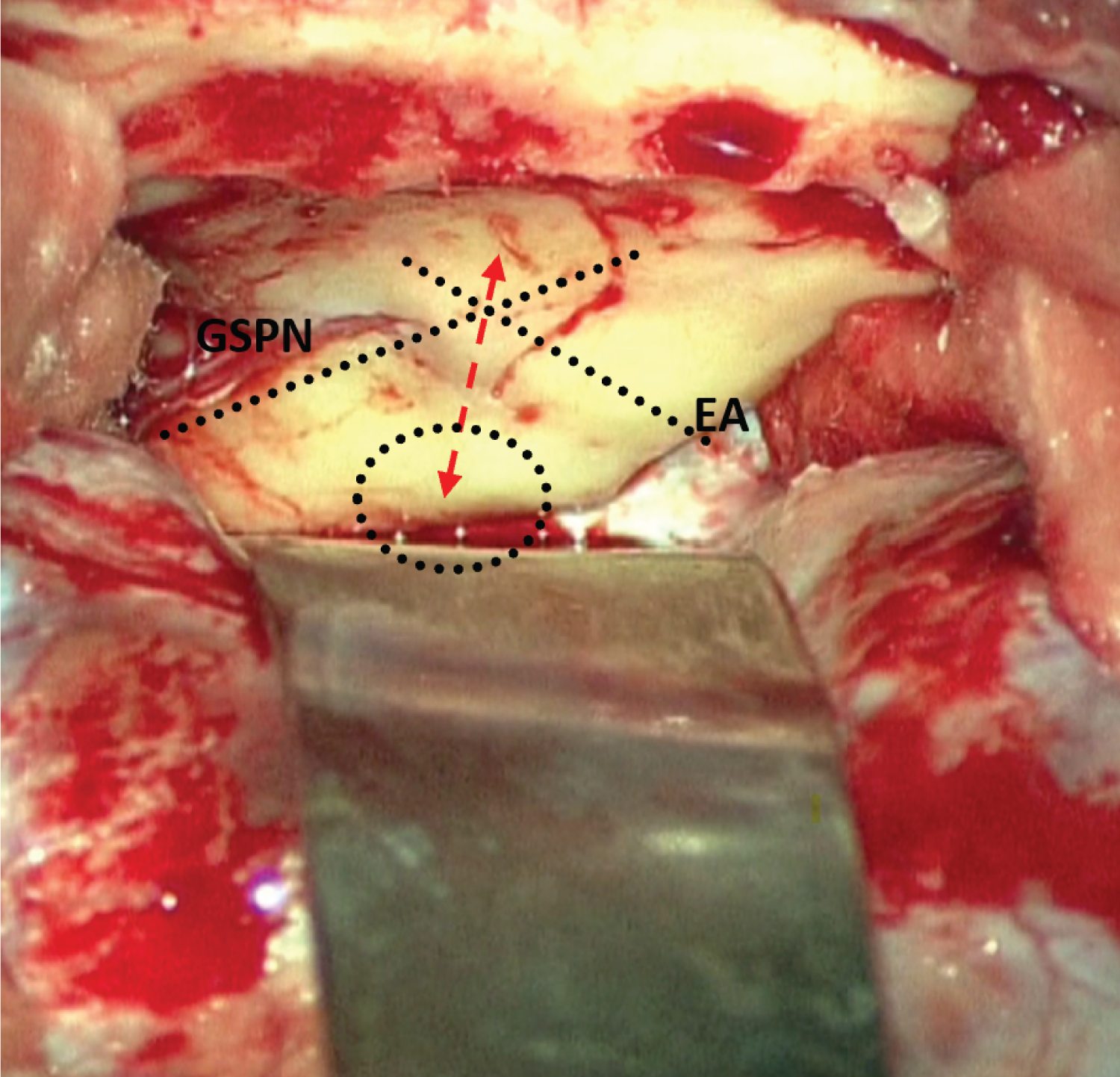 Figure 4: Identification of internal auditory canal according to the Garcia-Ibanez technique. It consists in drilling directly over the bisection of the angle formed by the Greater superficial (GSPN) and the eminence arcuata (EA).
View Figure 4
Figure 4: Identification of internal auditory canal according to the Garcia-Ibanez technique. It consists in drilling directly over the bisection of the angle formed by the Greater superficial (GSPN) and the eminence arcuata (EA).
View Figure 4
William house technique [2]: This is the technique we have adopted. The greater superficial petrosal nerve (GSPN) is the major landmark (Figure 3).
The operation consists of following the greater petrosal nerve from medial to lateral until the geniculate ganglion is exposed. The IAC dura can be found approximately 60 ° posteriorly from the long axis of the GSPN.
The bone superficial to the greater superficial petrosal nerve and geniculate ganglion is carefully removed by means of a rotating diamond drill under continuous irrigation with saline solution. It is not necessary to remove all the bone completely. A very thin transparent layer can be left over the structures so that their position and direction can be visualized. After identifying the geniculate ganglion, the labyrinthine portion of the facial nerve is located medial to the ganglion. Care must be taken to avoid the cochlea, which lies < 1 mm anterior to the labyrinthine portion of the facial nerve. The facial nerve is then followed in its labyrinthine portion until it enters the internal auditory canal. The lateral end of the IAC (Fundus) is dissected, and Bill's bar and the superior vestibular nerve are identified.
Fisch. U technique [5]: The eminencia acruata is considered the essential landmark for identifying the meatal plane. This method reduces the risk of an accidental traumatization of facial and cochlear nerves.
In fact, the eminence arcuata usually indicates the position of the SSCC, however the exact dimensions do not necessarily correlate with exact position of the SSCC. Location of the SSCC relies on determining the differences in bone density and color between the whiter membranous bone of the skull base and the yellow denser of the endochondral bone of the otic capsule. Another important relationship is that the lumen of the SSCC is perpendicular to the plane of the petrous ridge.
The technique used for the identification of the internal auditory canal is the following: The arcuate eminence and the meatal plane are placed in the center of the operating field. Using the operating microscope, the diamond drill and continuous irrigation, the bone is carefully removed over the arcuate eminence. Following identification of the labyrinthine capsule the bone removal is continued until the blue line of the SSCC is clearly visible. The blue line of the SSCC is found perpendicularly to the superior petrosal sulcus, at the center of the exposed labyrinthine bone. The bone situated in a sector limited by the exposed blue line and an imaginary line forming an angle of 60° with it, and centered over the superior ampulla is carefully removed with diamond drills of diminishing size. In order to expose the blue line, one has to stay as close as possible to this landmark. In the course of this procedure the posterior half of the internal auditory canal appears as a bluish area in the center of the described sector.
When the position of the internal auditory canal has been identified, the superior aspect of the dural lining of the meatus is entirely exposed from the fundus to the porus. A bridge of bone is, however, left over the porus in order to secure support for the spatula retracting the temporal lobe. The last shell of bone covering the meatal dura is removed with a fine excavator.
Garcia-Ibanez E technique [6]: This technique was considered as rapid with the objective of decrease the time of retraction of the temporal lobe.
The eminencia acruata and GSPN are the essential landmarks for identifying the meatal plane. This method consists in drill directly over the bisection of the angle formed by the petrosal nerve and the eminence arcuate (Figure 4). Removing the bone medially in this area, the dura of the internal auditory canal was exposed. The drilling is continued by removing bone laterally until the end of the internal auditory canal is identified.
The removal of the bone begins from the superior surface of the IAC, medially at the porus acusticus. The fundus of the IAC is dissected, and Bill's bar and the superior vestibular nerve are identified (Figure 5). Medially, 270° of bone can be removed from its circumference. Once the IAC exposure is complete, the thin bony layer is removed [5].
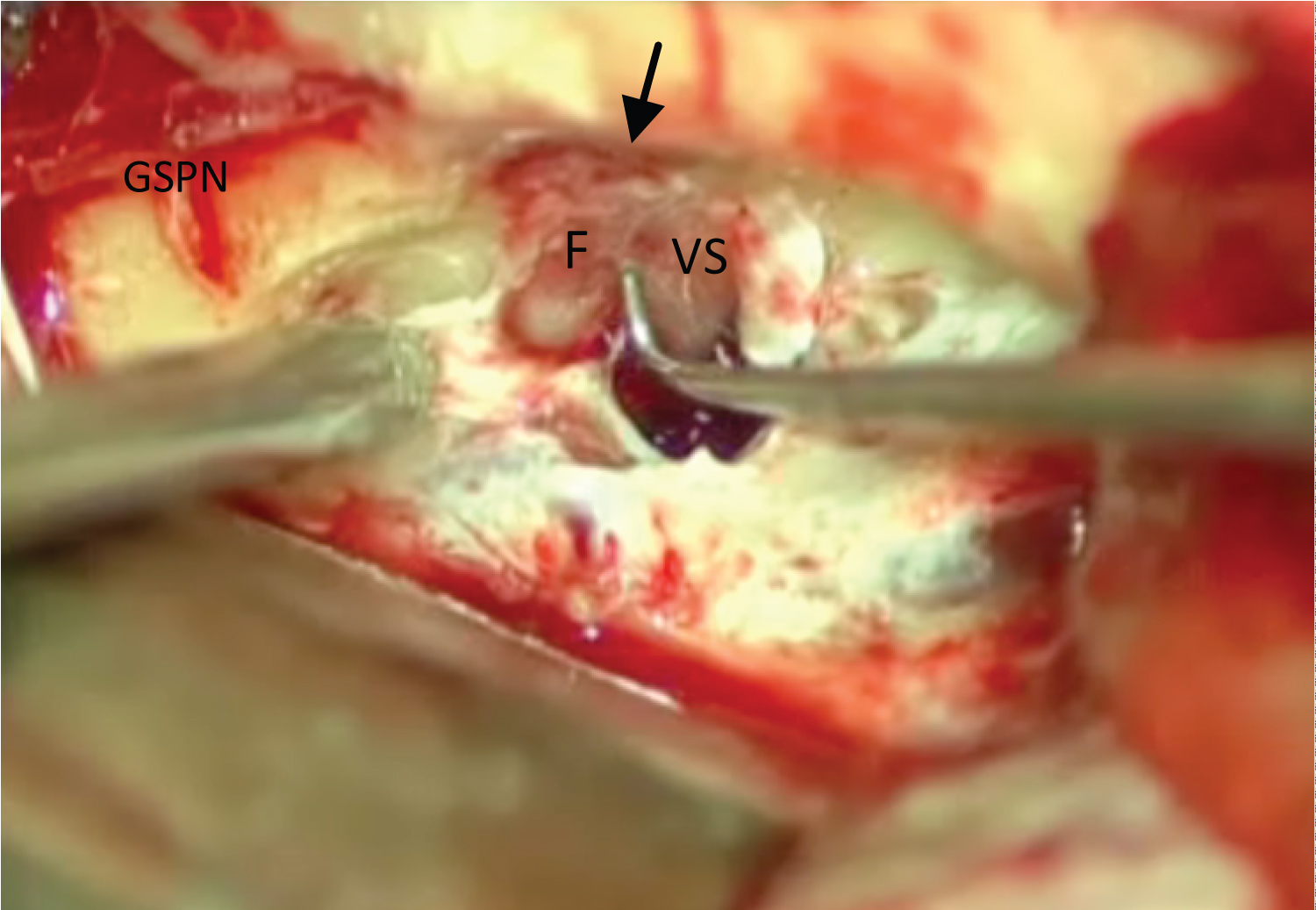 Figure 5: The dura of AIC was opened. Dissection of Bill’s bar (Black arrow) and identification of superior vestibular nerve SV and facial nerve FN.
View Figure 5
Figure 5: The dura of AIC was opened. Dissection of Bill’s bar (Black arrow) and identification of superior vestibular nerve SV and facial nerve FN.
View Figure 5
Care must be taken to open the IAC dura as the facial nerve can be pushed against the dura by the tumor. One strategy to avoid the injury to the facial nerve is to open the dura on the posterior side of the superior surface of the IAC dura as the facial nerve is typically pushed anteriorly [3]. The facial nerve is identified anatomically and physiologically with a nerve stimulator (Figure 5).
Muscle graft is used to close the defect in the IAC (Figure 6). The muscle fragments will be taken from the temporalis muscle. The autostatic temporal lobe retractor is removed. The dura mater was suspended. The bone flap is then returned into its anatomic position and fixed. The tem- poralis muscle and skin flaps are then sutured back into place. The uses of percutaneous drains are not typically needed when the hemostasis has been well assured.
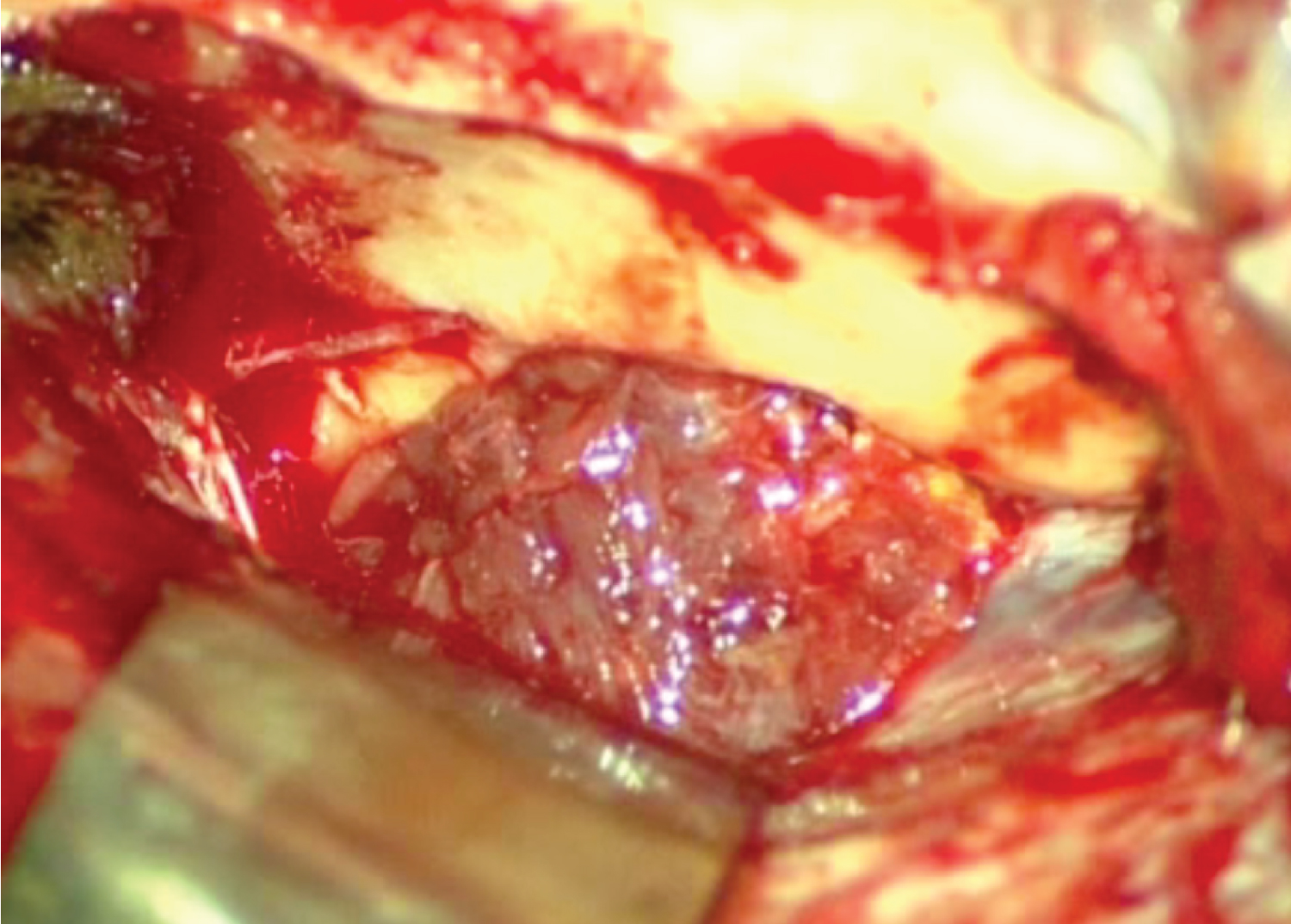 Figure 6: The defect in the IAC was closed by muscle graft.
View Figure 6
Figure 6: The defect in the IAC was closed by muscle graft.
View Figure 6
The middle fossa technique requires special knowledge of the anatomy to reduce the risk of damage to the labyrinthine segments of the facial nerve, geniculate ganglion, cochlea, labyrinthine structures and carotid artery.
As hearing preservation is the hallmark of the middle fossa approach, a detailed knowledge of the microsurgical anatomy of the middle fossa floor is mandatory to define the surgical limitations and to avoid any complications.
It’s a good approach for small intracanalar symptomatic or size increasing vestibular schwannomas with normal hearing (serviceable hearing) and for vestibular neurotomy for Ménière's disease.