Parotid region swellings are the most commonly encountered presentations in ENT OPDs, the causes of which range from inflammatory conditions to benign/malignant parotid tumors and at times can be a manifestation of an underlying systemic disease. Multiple myeloma is a rare type of blood cancer characterized by monoclonal proliferation of plasma cells and its presentation as a parotid region swelling is very rare. We report a case of a 57-year-old female with swelling over the parotid region of one-month duration. Fine needle aspiration cytology revealed plasma cell neoplasm. On further evaluation, lytic lesion over the mandible along with multiple lytic lesions over the skull and ribs were noted. Relevant blood investigations were done and a final diagnosis of multiple myeloma was made. We report this case due to its uncommon presentation at an unusual site (parotid region) as the first evidence of underlying systemic disease diagnosed on fine needle aspiration cytology.
Multiple myeloma, Plasmacytoma, Extramedullary plasmacytoma, Parotid, Fine needle aspiration
Multiple myeloma [MM] is a B-cell malignant lymphoproliferative disorder with monoclonal plasma cell proliferation and has varied clinical presentations [1]. It can present at unusual sites with uncommon symptoms in day-to-day clinical practice making it a diagnostic challenge for both clinicians and pathologists. We report a case of a 57-yrs-old female with swelling over the parotid region referred from ENT OPD for fine needle aspiration. Cytological features suggested plasma cell neoplasm. We report this case due to its uncommon presentation at an unusual site (parotid region) as the first evidence of underlying disease diagnosed on FNAC. So far less than 25 published cases of such rare presentation have been reported in literature diagnosed by fine needle aspiration [1,2].
A 57-yr-old female presented to ENT OPD with swelling over the left parotid region measuring 5 × 4 cm of 1 month duration (Figure 1). The patient has been a betel nut chewer for 30 yrs and had consulted with a dentist initially for the swelling and then referred to our center for further evaluation. The swelling was gradually increasing in size with mild dragging pain. She further complained of generalized body weakness and dull aching headache occasionally. Fine needle aspiration was done using a 22 G needle and a 10 cc syringe. Alcohol-fixed smears and air-dried smears were examined with H&E, PAP, and Giemsa staining. Highly cellular smears revealed pleomorphic looking plasma cells with eccentrically placed nuclei with high nuclear cytoplasmic ratio and abundant eosinophilic cytoplasm (Figure 2 and Figure 3). A preliminary diagnosis of plasmacytoma was considered and further work-up was suggested to look for systemic involvement of the disease. Routine blood investigations revealed Hb: 8.5 mg/dl, WBC: 6660 cells/µl and platelet count: 2.13 lakh/µl. Peripheral smear examination revealed a dimorphic blood picture with increased rouleaux formation. ESR was 100 mm/1 st hr. Serum creatinine levels were 3.38 mg/dl and blood urea nitrogen 35 mg/dl. Serum Calcium levels were 13.5 mg/dl and elevated. Meanwhile, an X-ray skull showed multiple lytic lesions and a lytic lesion over the mandible corresponding to the swelling (Figure 4). CT scan further confirmed multiple lytic lesions over the skull and ribs. The urine routine showed trace albumin. Bence Jones protein test on the urine sample was performed and turbidity appeared at 60 °C on heating, dissolved at 100 °C, and reappeared after cooling thereby contributing to the diagnosis. A final diagnosis of multiple myeloma was made after clinical, radiological, and cytological correlation.
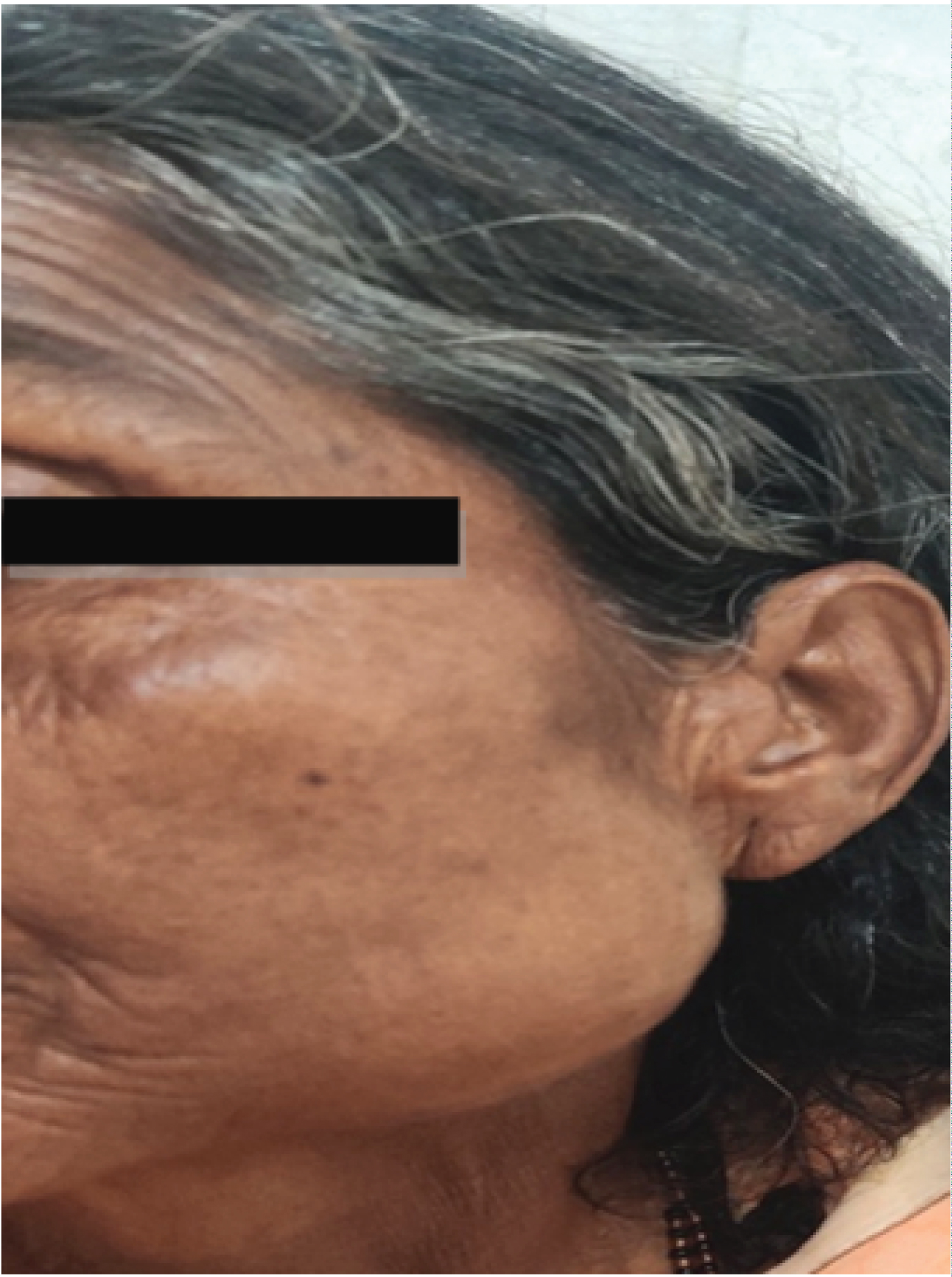 Figure 1: Left parotid region swelling measuring 5 × 4 cm.
View Figure 1
Figure 1: Left parotid region swelling measuring 5 × 4 cm.
View Figure 1
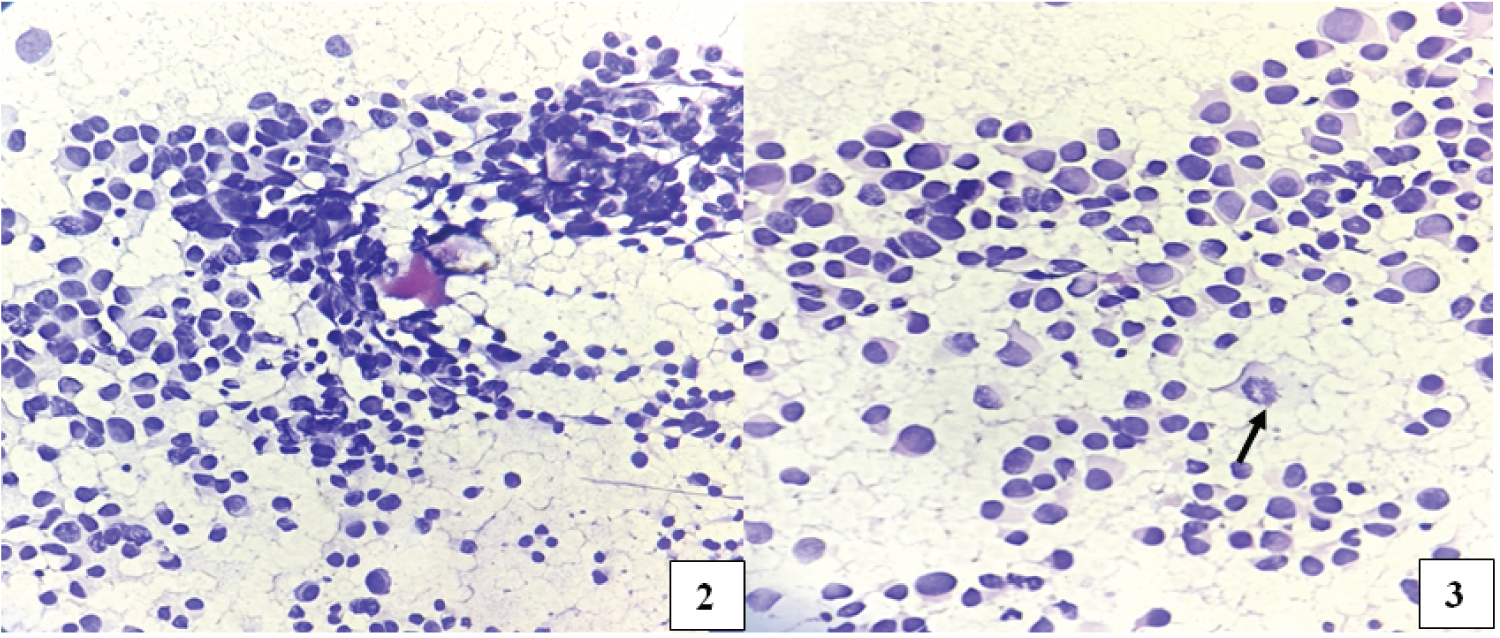 Figure 2 and 3: Highly cellular smears round oval to plasmacytoid looking cells in sheets and clusters. Papanicolaou stain 10x.
Figure 2 and 3: Highly cellular smears round oval to plasmacytoid looking cells in sheets and clusters. Papanicolaou stain 10x.
Plasma cells with high nuclear-cytoplasmic ratio with eccentrically placed nucleus. Mitotic figures seen (arrow). Papanicolaou stain 40x.
View Figure 2 and 3
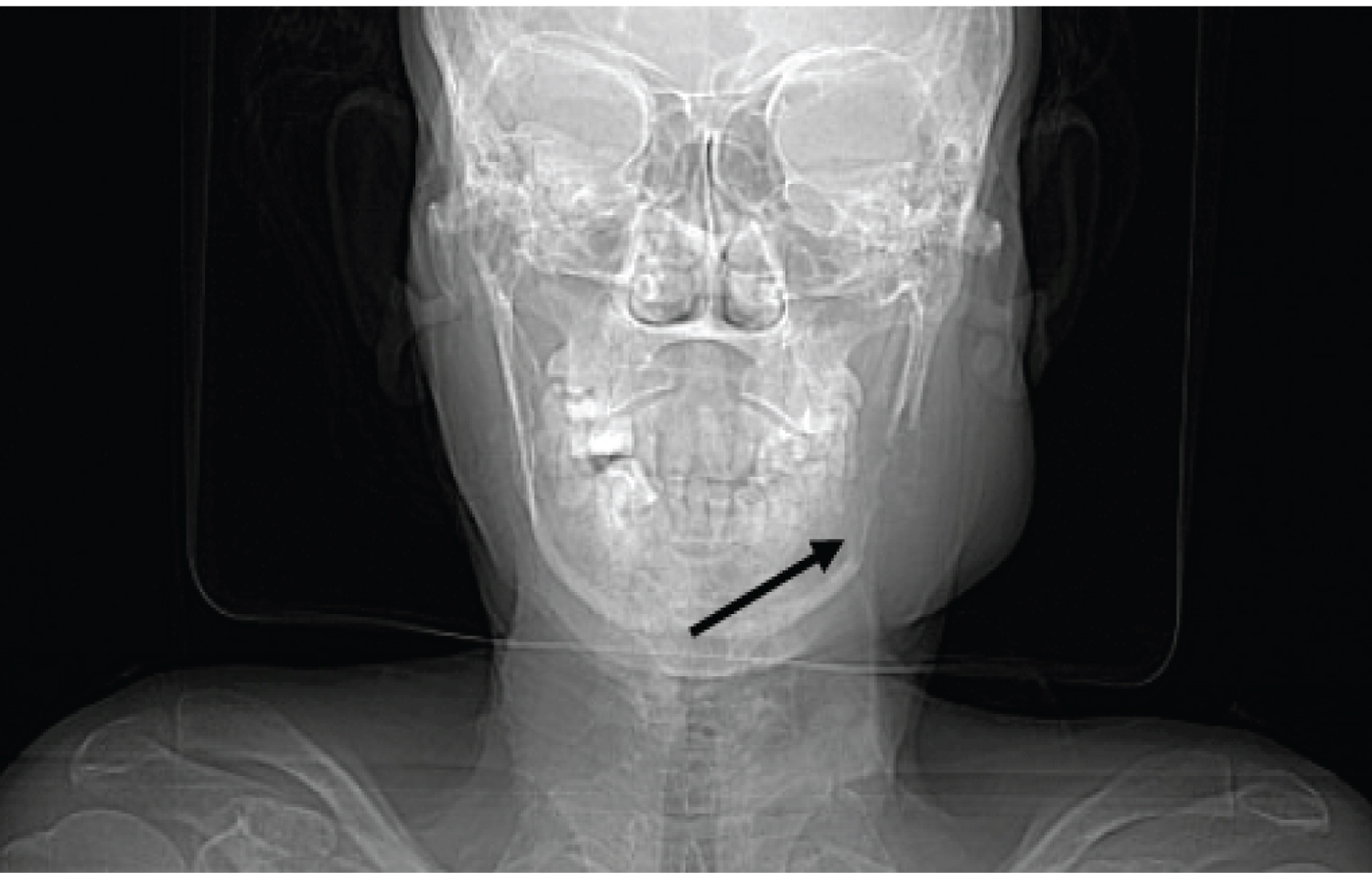 Figure 4: CT scan shows lytic lesion over mandible corresponding to the parotid region swelling.
View Figure 4
Figure 4: CT scan shows lytic lesion over mandible corresponding to the parotid region swelling.
View Figure 4
Myeloma is a plasma cell neoplasm that usually causes bony lesions, renal failure, and hematological abnormalities with hyperviscosity conditions leading to life-threatening, fatal complications. It can present as a solitary intramedullary lesion (plasmacytoma) or may involve multiple sites (multiple myeloma) [3]. Extramedullary myeloma with an unusual presentation of parotid region swelling as the initial symptom of a systematic disease is a very rare occurrence [1]. So far, less than 25 published cases of such a rare presentation have been reported in the literature, diagnosed by fine needle aspiration [1,2]. The exact cause of multiple myeloma is uncertain. Frequent changes and translocations in promoter genes, chromosome 14, have been known for disease progression [4]. Oncogenes, such as NRAS, KRAS, and BRAF, are also known to be associated with neoplastic plasma cell proliferation [5]. Obesity, alcohol consumption, and environmental causes such as pesticides, organic solvents, and radiation exposure are other known contributing factors. It occurs predominantly in the elderly population, with a mean age of presentation of 70 years, and has more predilection in males than females (1.4:1) [6]. Our patient was a 57-year-old female and a chronic betel nut chewer. Parotid region swelling was her first presenting symptom associated with body aches and jaw pain. This case was unusual as the patient was first diagnosed by cytology on fine needle aspiration and later contemplated to look for underlying systemic involvement by multiple myeloma, which was confirmed by a panel of hematological, biochemical and radiological investigations. On further investigation, hypercalcemia with increased creatinine levels and anemia were known. Marrow infiltration with an increased plasma cell population usually results in anemia, thrombocytopenia, and leukopenia. The interaction between myeloma cells and the bone microenvironment results in the activation of osteoclasts and the inhibition of osteoblasts, resulting in bone loss and lytic lesions. In our case, the patient had a lytic lesion over the mandible corresponding to the swelling, with multiple lytic lesions in the skull and ribs. The acronym CRAB was defined as criteria by the International Myeloma Working Group in 2003 to simplify the most typical clinical manifestations of multiple myeloma, which include hypercalcemia, renal failure, anemia, and bone disease [7]. As per CRAB criteria, our patient had hypercalcemia (13.5 mg/dl), renal failure (S. creatinine: 3.38 mg/dl), anemia (Hb: 8 g/dl), and bone disease (multiple lytic lesions). Bence Jones protein in urine turned out to be positive. CRAB criteria are important for the initiation of chemotherapy and to predict the prognosis of the disease [7]. Upon diagnosis, the patient was referred to a tertiary oncology center for chemotherapy and is presently under treatment. The International Myeloma Working Group (IMWG) amended the diagnostic criteria for MM in 2014 [8]. In addition to the established CRAB traits, the diagnosis of MM requires 10% or more clonal plasma cells on bone marrow examination or a biopsy-proven plasmacytoma with the presence of one or more myeloma-defining events [8]. Through this case, we would like to emphasize the importance of fine needle aspiration, which is a minimally invasive rapid technique for the diagnosis of such uncommon lesions for early clinical intervention and better patient prognosis.
This case was unique because the patient came to the ENT department for parotid region swelling and multiple myeloma/plasmacytoma was diagnosed incidentally through FNA. This case report highlights the presentation and diagnostic approach in parotid region swellings which are common in day to day practice and should be considered as a differential diagnosis while evaluating such head and neck lesions.
We thank the Department of Radiology for their expertise and assistance. We thank our technical staff for their constant support throughout the case study.