Congenital nasal anomalies are rare. Hypoplasia and atrophic anomalies represent the most common class of congenital nasal anomalies. A 27-year-old female presented with obvious right nostril asymmetry, alar notching, and retraction. The patient underwent a closed (endonasal) septorhinoplasty approach under general anesthesia. The lower lateral cartilage exposed by the cartilage delivery technique was discovered the absence of right lower lateral cartilage. In this case, reconstruction was performed by using two grafts the resected cephalic portion of lateral crura of left lower cartilage as medial crus and harvested septal cartilage as lateral crus, with satisfactory functional and cosmetic results.
Congenital nasal anomalies, Aplasia of lower lateral cartilage, Closed rhinoplasty approach
The congenital anomalies of the nose are rare [1], occur in 1\20000-1\40000 of newborns [2]. The anomalies of the nose range from complete aplasia of the nose to duplications and nasal masses [3]. It was classified into four categories. 1) Hypoplasia and atrophy; 2) Hyperplastic or duplications; 3) Clefts and 4) Neoplasms and vascular anomalies (Losee, et al.) [4,5].
According to this classification, our case was of a type I anomaly. Hypoplasia and atrophic anomalies represent the most common class of congenital nasal anomalies [6]. There are many reported cases of isolated lower lateral cartilage defects. The isolated congenital nasal anomalies that cause remarkable aesthetic deformities are extremely rare [7]. The most reported cases are unilateral [1,6,8]. Bilateral aplasia is rare [2,7,9]. The incidence of Lower lateral cartilage aplasia was reported about 0.016 of consecutive series of primary septorhinoplasty patients [8].
The nasal embryological development occurs between the 3rd and 10th weeks of gestation [1]. The nose developed from neural crest cells. The nasal placodes divided by the nasal pits into medial and lateral nasal processes, the medial processes will ultimately fuse, contributing to the nasal septum and the medial crura of the lower lateral cartilages. The lateral processes develop into the nasal bones, upper lateral cartilages, ala, and lateral crura of the lower lateral cartilages [5].
A 27-year-old female presented complaining of external nasal deformities and nasal obstruction seeking esthetic surgery. There was no history of any genetic conditions, facial trauma, previous nasal surgery.
Nasal inspection shows an obvious right nostril asymmetry (depressed right dome and smaller right nostril), alar notching, and retraction was noted. The absence of any palpable cartilage within the right side of the nasal tip and right nasal ala (Figure1) (Cottles test was +ve at right side showed evidence of nasal valve obstruction. Endoscopic examination, there was right-sided nasal septal deviation (inferior septal spur) with hypertrophied left inferior turbinate. The history and physical examination were otherwise normal. The patient had given informed written consent for publishing their data.
She was treated at Al-twfiq private Hospital, Salah-Eden governorate, Iraq in 2021, for cosmetic and functional correction.
The patient underwent a closed (Endonasal) septorhinoplasty approach under general anesthesia. A bilateral intercartilaginous incision is made along the inferior border of upper lateral cartilage the incision is then curved towards the septum where it meets the transfixion incision that is made at the caudal end of the septal cartilage. A subperichondrial dissection using a Freer elevator was carried out on both sides of the cartilaginous septum, Then perform inferior and posterior septal tunnel bilaterally with subperiosteal dissection, Spur removal was performed by dislocation of deviated inferior part of septal cartilage that forming the spur from deviated maxillary crest by elevator, and bony spur removed by Middleton Jansen septum punch. The inferior cartilaginous spur with part of septal cartilage incised by a knife and harvesting for grafting. Separation of the upper lateral cartilage from the nasal septum. Dorsal hump removal (2-3 mm) bone by osteotome, and 3-5 mm cartilage by angled foeman scissor, with bony rasping for dorsal smoothing. Bilateral lateral percutaneous osteotomies using 2 mm osteotome and in-fracture of the nasal bones.
For the nasal tip, the lower Lateral cartilage is exposed by the cartilage delivery technique using marginal (Rim) incision made along the inferior (caudal) border of the lower lateral cartilages, and intercartilagenous incisions. When the lower lateral cartilage has been delivered found the absence of right lower lateral cartilage on the right side, only a fibrotic band was present in the place (Figure 2A and Figure 2B). After cartilage delivery resection of the cephalic portion of the left lower cartilage was performed leaving 6 mm wide, this remaining caudal part was separated from underlying vestibular skin.
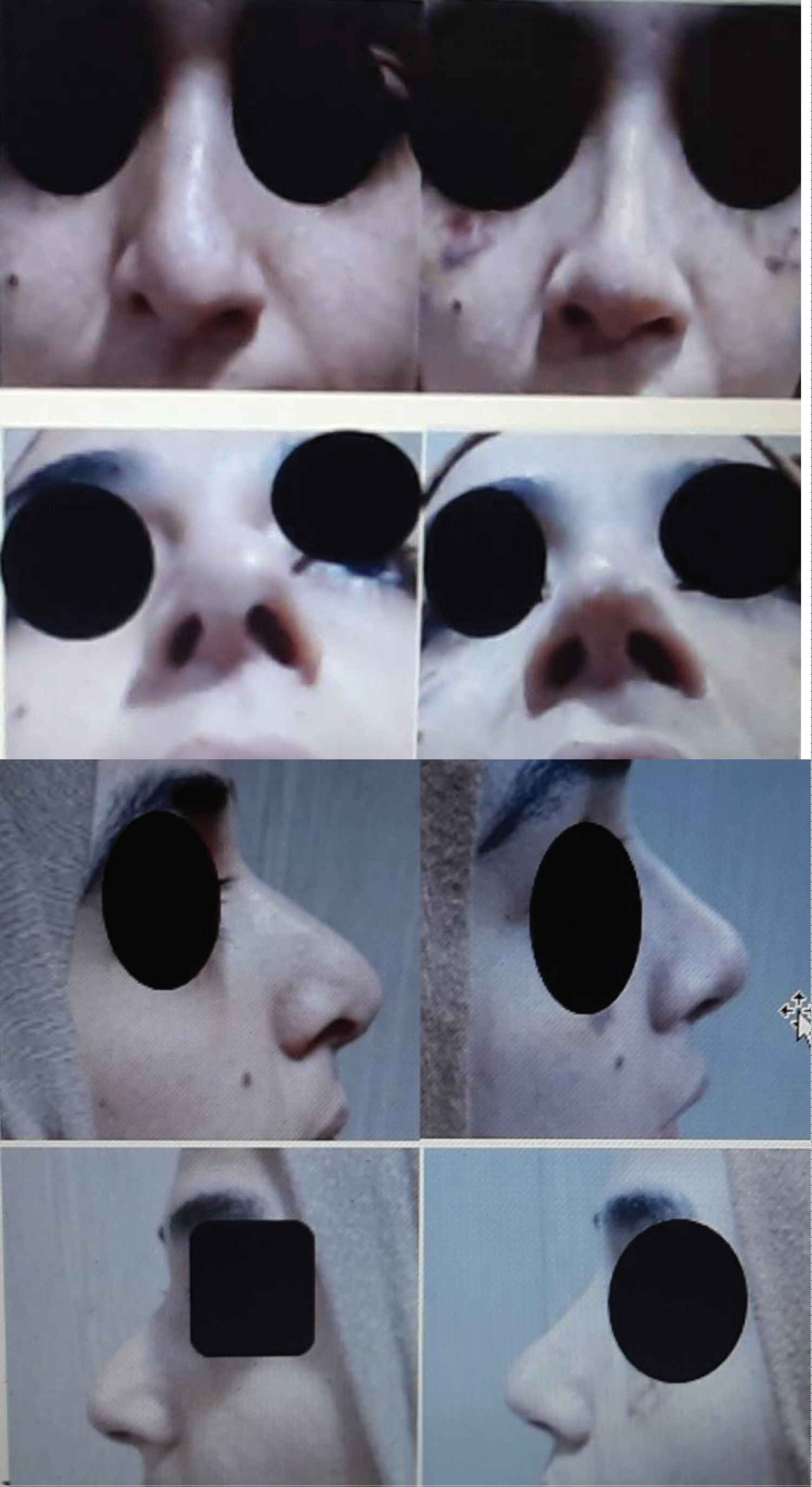 Figure 1: Preoperative and postoperative appearence. Left (Preoperative): An obvious nostril asymmetry (depressed right dome, Smaller right nostril), alar notching and retraction was noted (furrow at soft triangle); Right (Postoperative results).
View Figure 1
Figure 1: Preoperative and postoperative appearence. Left (Preoperative): An obvious nostril asymmetry (depressed right dome, Smaller right nostril), alar notching and retraction was noted (furrow at soft triangle); Right (Postoperative results).
View Figure 1
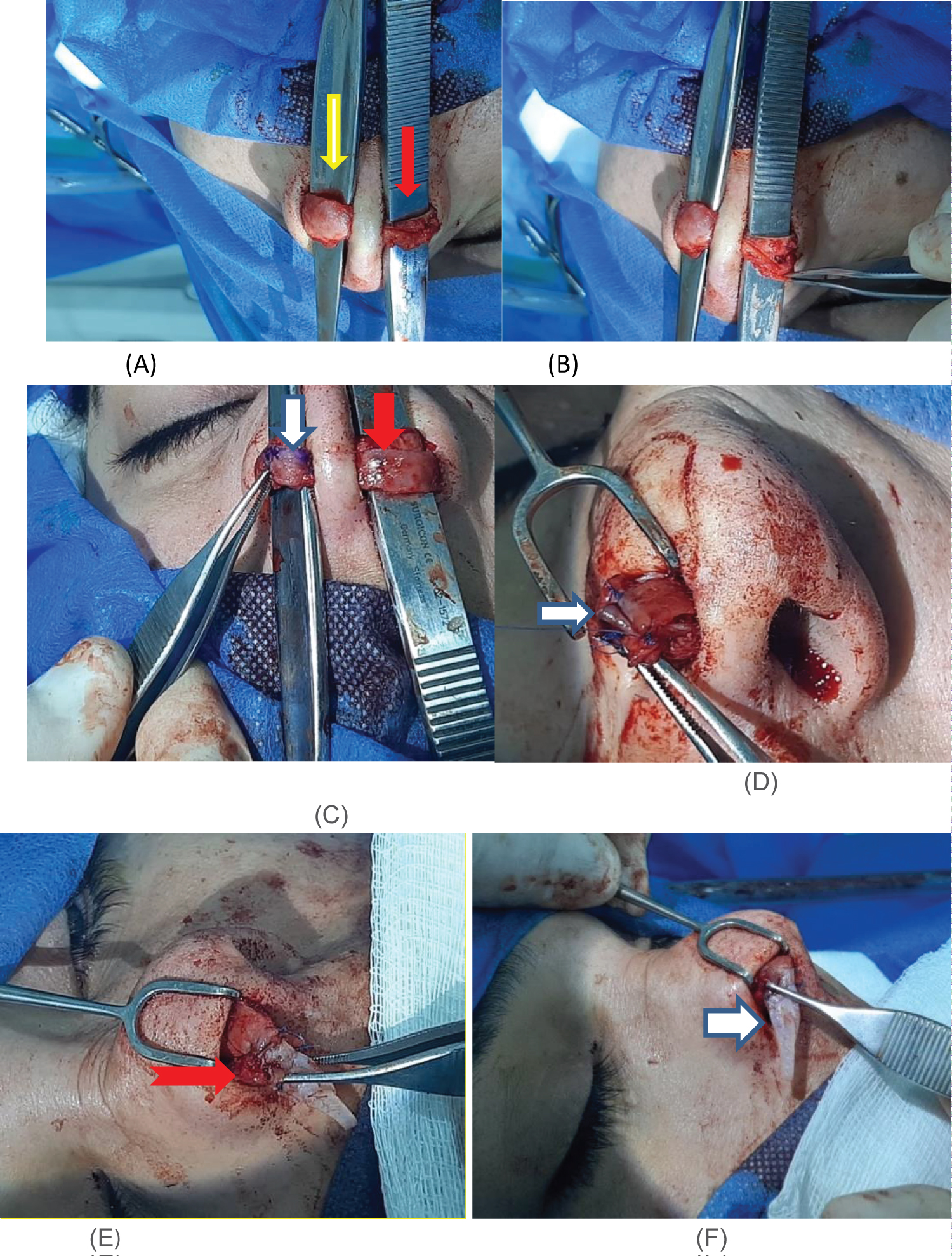 Figure 2: Operative pictures. (A,B) Cartilage delivery technique was discovered the absence of right lower lateral cartilage (Yellow arrow), normal loer lateral cartilage (Red arrow); (C) The resected cephalic portion of the left lower lateral cartilage (Red arrow), transfer to the right side (White arrow); (D) Suture the dome of left lower lateral cartilage to the cephalic portion of left loer lateral cartilage on right side; (E,F) A harvested septal cartilage graft, used as extender alar rim graft fixed medially to the dome (E red arrow) and laterally insert in the tunnel at the alar margin extending to the alar base (F white arrow).
View Figure 2
Figure 2: Operative pictures. (A,B) Cartilage delivery technique was discovered the absence of right lower lateral cartilage (Yellow arrow), normal loer lateral cartilage (Red arrow); (C) The resected cephalic portion of the left lower lateral cartilage (Red arrow), transfer to the right side (White arrow); (D) Suture the dome of left lower lateral cartilage to the cephalic portion of left loer lateral cartilage on right side; (E,F) A harvested septal cartilage graft, used as extender alar rim graft fixed medially to the dome (E red arrow) and laterally insert in the tunnel at the alar margin extending to the alar base (F white arrow).
View Figure 2
The reconstruction of neo lower lateral cartilage was performed by suturing the resected alar cartilage with the dome of left lower lateral cartilage (transdomal suture) by 6/0 PDS as medial crura (Figure 2C and Figure 2D). The harvested septal cartilage graft (24 mm length, 8 mm-3 mm wide) was fixed medially to the dome by 6/0 PDS and laterally insert the cartilage in the dissected tunnel at the alar margin extending to the alar base as lateral crura (Figure 2E and Figure 2F).
For hypertrophied inferior turbinate underwent microdebrider assisted turbinoplasty. A satisfactory functional and cosmetic result was achieved (Figure 1).
Nasal tip deformities can be congenital or acquired secondary to nasal trauma or previous nasal surgeries [10]. Isolated non-syndromic congenital nasal anomalies including aplasia or absence of lower lateral cartilage are rare [6].
The lower lateral cartilages of the nose have three components lateral crus, middle crus, and medial crus. It is configuration gives the characteristics of the nasal tip (shape, volume, width, definition, tip projection, and rotation), alar rim, and tip support. The atrophy or weakness of lateral crura causes alar rim notching with retraction and lateral nasal wall weakness and the underdeveloped medial crura present with under projected tip and lack of tip definition [10] and external nasal valve dysfunction [11]. The patient will complain of nasal obstruction and aesthetic consequences.
Multiple techniques of varying complexity have been described for reconstruction of the congenital aplasia or atrophy of lower lateral cartilage with autologous cartilage grafts from the nasal septum and conchal cartilage or allogenic grafts, using open rhinoplasty approach [1,2,8-10] that permits direct exposure of the lower lateral cartilage providing a more accurate diagnosis and surgical intervention. In this case, the author used the endonasalrhinoplasty approach for reconstruction of aplasia of lower lateral cartilage to show that the endonasal approach can achieve as good results as the open approach while avoiding the columellar scar, has a shorter recovery period and less swelling. The limitations of this procedure are that the surgeon requires more surgical Skill and experience in the endonasalrhinoplasty approach. In this case reconstruction of aplastic lower lateral cartilage was done via the endonasalrhinoplasty technique using two autologous grafts. 1) The resected cephalic portion of lateral crura of lower lateral cartilage of normal side which sutured with left lower lateral cartilage by transdomal suture for tip projection; 2) A harvested septal cartilage graft was used as graft sutured on the lateral crura graft. This method of reconstruction resulted in satisfactory functional and cosmetic results (Figure 1).
Aplasia of lower lateral cartilage is a technical challenge in rhinoplasty. Several reconstructive methods have been recorded, all of which are used the open rhinoplasty approach. In this case, the endonasalrhinoplasty approach was used to reconstruct aplasia of lower lateral cartilage using the resected cephalic portion of lateral crura from the other side and harvested septal cartilage grafts, with satisfactory functional and cosmetic results.
The authors have no conflicts of interest to declare.
The patient had given informed written consent for publishing their data.