Pleomorphic adenoma is one of the most common benign tumors of the major salivary glands. It can also occur in the minor salivary glands, which exist in the nasal cavity. We present a case of pleomorphic adenoma masquerading as squamous cell carcinoma in 61-year-old man. This patient presented with nasal obstruction, nasal bleeding and nasal deformity. Biopsy have reveled moderaletly differenciated squamous cell carcinoma. After surgical procedure (lateral rhinotomy). The final diagnosis affirmed pleomorphic adenoma.
Septal pleomorphic adenoma, Septal tumors, Immunohistopathology, Nasal septum
Pleomorphic adenoma of nasal septum is a rare entity. The first description reported in 1929 by Denker Khaler [1,2]. The clinical presentation is poor, nasal obstruction, bleeding nose, rhinorrhea. Diagnosis is recognized after tumoral biopsy. Imaging is fundamental for fine evaluation and extension diagnosis. Surgery is the main treatment based to complete remove of tumor with clean margin.
M. A 63-year-old man presented to our department with unilateral right-sided nasal obstruction 18 months' evolution associated with epistaxis. In personnel history we find a trace for arterial hypertension since 20 years. Clinical examination found edema with enlargement of the nose root. Palpation notes a depression of the nasal bone with elastic sensation and bone blow impression. Nasal endoscopy shows a gray mass obstructing the right nasal fossa with septal deviation from left side. There are no cervical lymph nodes.
Computed tomography (CT) of nasal cavity and paranasal sinuses show's a mass with tissue density and bad borderline from 37 × 24 mm localize in the anterior part of right nasal cavity. This mass is enhanced heterogeneous after contrast injection. A nasal bony destruction is observed without lesion of adjacent structures (sinuses, orbit) (Figure 1 and Figure 2).
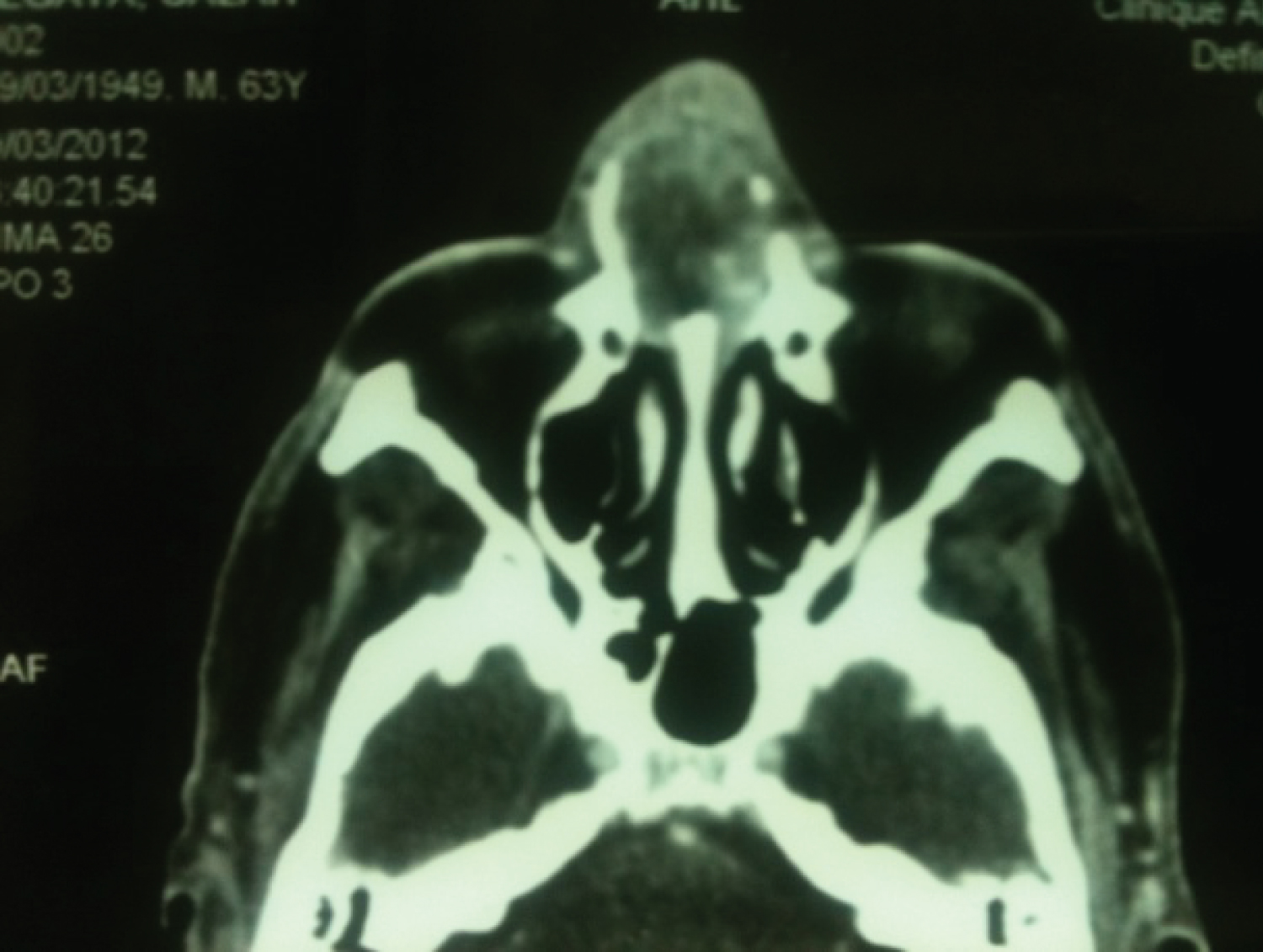 Figure 1: CT scan axial section: Heterogenous septal tumor and bony lysis.
View Figure 1
Figure 1: CT scan axial section: Heterogenous septal tumor and bony lysis.
View Figure 1
 Figure 2: CT scan sagital section: Tumor with septal insertion.
View Figure 2
Figure 2: CT scan sagital section: Tumor with septal insertion.
View Figure 2
Endonasal biopsy of tumor finds a moderately differentiated squamous cell carcinoma.
The pre-therapeutic checkup is without anomalies. The patient is operated by later nasal rhinotomy. A blading tumor of 40 × 25 mm is fund, easily cleavable with 15 mm septal caudal cartilage implantation. The bony nose is completely laminate with cartilaginous pseudo-consistency (loss of ossification).
After septal transfixing incision, we remove in totality the tumor with septal cartilage implantation and a part of vomer and ethmoid (perpendicular lamella) (Figure 3). We preserved a distal part of septal cartilage and make a bilateral nasal packing. Post-operative sequence was simple. Histopathological study of the surgical specimen notes an encapsulated benign tumor with mesenchymal and epithelial contingent. The epithelial component is available in tubular masses and structures contained in mesenchymal loose tissue and myxoid.
 Figure 3: Surgical specimen: Tumor with septal cartilage insertion.
View Figure 3
Figure 3: Surgical specimen: Tumor with septal cartilage insertion.
View Figure 3
The final pathologic diagnosis made from the resected specimen was pleomorphic adenoma of the septum without malignancy.
The pleomorphic adenoma is a mixed epithelialy-mesenchymal lesion developed at salivary gland. In upper airways the first site is the nasal cavity before sinus and nasopharyngeal location. The septal location sees in 80% of the nasal variety against 20% for the lateral wall, especially the turbinate structures. For pathogeny, STEVENSON.HN considered the development of nasal pleomorphic adenoma is possible after modification of vomero nasal unit of Jackobson or could be induced by a viral infection [3,4].
Matthew S believes that the genesis of these tumors might happen to after migration of ectodermic epithelial cells from the nasal point to the septal region [5].
The pleomorphic adenoma of the nasal septum is an adult pathology most occur 30 and 60-years-old without preponderance of sex. Female preponderance is reported in some publications. The average time of consultation is between 1 and 2 years [2].
Clinically the most symptom is unilaterally and progressive nasal obstruction, rhinorrhea, epistaxis and rarely an external nasal deformity. Painful forms are uncommon.
Nasal endoscopy can show an obstructive gray mass sometimes hemorrhagic. She takes sometimes a translucent polypoid aspect [2,3]. The mass is frequently localize on the septal cartilage, but sometimes can be seen at the posterior part (bone).
Usually the tumor is covered with a normal mucosa (ulceration is view in case of traumatism or infection) respecting nasal cartilage with a capsule (more or less regular). Generally there is a cleavage way between tumor and cartilage.
Imaging is fundamental examination from all progressive obstruction tumors. In all cases we realized a computer tomography (CT) and MRI. Computed tomography scans revealed the tumor involvement location (septum), the tumor volume, sessile or pedicular aspect, tumor extensions, mensurations, vascular affinity, organs (orbit, paranasal sinuses, skull base) and could suggest an aggressive type if destruction of bone is seen.
The CT scan visualizes a regular, homogeneous tumor without taking that contrast. Fine calcifications may be to visualized.
MRI shows intense is homogeneous mass in T1 with a hyper-signal in T2. The intra-tumor necrosis is represented by a hypo-signal in T1 with a hyper-signal in T2. The tumor capsule generates a signal of low intensity in T2 with the loss of great signal in T1 [6].
Diagnosis of pleomorphic adenoma is anatomopathological. Biopsy is often hemorrhagic.
Macroscopically the tumor is closed, gray-white with irregular and granular surface. Voluminous tumors appear lobulated.
On the microscopic study the pleomorphic adenoma in nasal location (septal) is different from the classic form (parotid, sub-mandibular gland). It is characterized by a great cellular wealth (hypercellularity) and a very poor stroma. Some varieties are exclusively cellular without associated stroma.
Furthermore biopsy specimen (area and deep of biopsy) and hypercellularity might have been interpreted as malignant variety. This difficulty is noted by the publicaton of Compagno and Wong in which 55% of the cases initially misdiagnosed [7].
In our review of the literature we have found a few reported observations with initialy malignant diagnosis after tumoral biopsy (squamous cell carcinoma, cystic adenoid carcinoma) rectified after final anatomopathological examination of the surgical specimen removed with pleomorphic adenoma ultimate diagnosis [8,9] (Table 1).
Table 1: Nasal pleomorphic adenoma: Cases misdiagosis with malignant variety. Report of Literature. View Table 1
Our observation is an illustration of difficulties performance of nasal tumor biopsy. In first the diagnosis performed septal squamous cell carcinoma (specimen biopsy) or final examination of the operative specimen removed attested a benign variety pleomorphic adenoma.
Differential diagnosis may be possible with an inverted papilloma, angiofibroma, chondromyxoma, oncocytoma, schwannoma, epidermoid carcinoma.
Evolution after complet removing (clean margins) is favorable. For Compagno J, conservative tumoral removing is associated with 10% of recovery [7]. The main risks are local reccurence.
A myxoid stroma may also promote recurrence.
Malignant transformation of this tumors is possible in 6% and may to be transformed at adenocarcinoma, squamous cell carcinoma or mucoepidermoid carcinoma [4,5].
In addition of this clinical presentation, Freeman SB reported observation of a metastatic pedomorphic adenoma at the nasal septum after an initial sub-mandibular localization. These forms correspond to metastasizing pleomorphic adenoma entity (MPA) with similar histologic presentation of initial localization [10].
Surgery that achieves clear margins is the treatment of choice. Actually the endonasal endoscopic procedure is the first choice. Many authors have reported good results and appreciable follow ups. In other cases we can do an external surgical way (lateral rhinotomy nasal, degloving).
Pleomorphic adenoma of the nasal septum is uncommon tumor, without specific symptoms and generally histological discovery. Microscopically cellularity fullness of these tumors can make some difficulties to evaluate specimen biopsy with possible initially pejorative diagnosis (malignancy feeling).
Surgical approach is habitually making with endoscopic endonasal procedure. Recurrence occurs after incomplete removing or positive mucous margins.