In Al-Baha City, Saudi Arabia, there have been few or no statistical studies evaluating the prevalence and pattern of Head and Neck malignancies and till today no published data. The current study was conducted to analysis the different clinical and pathological features of head and neck cancers at Al-Baha region, Saudi Arabia.
This is a retrospective, cross-sectional study, in which the records of patients presented to the Otorhinolaryngology (ENT), and various surgical departments at King Fahd Hospital at Al-Baha region and the documents of patients referred from Al-Baha region to the nearby specialized and oncology centers over ten years (January 2009-December 2019). A total of 470 patient's records were reviewed for the following variables: Age, sex, occupation, smoking and alcohol consumption habits, primary tumor location, clinical tumor stage, histological type and grade, diagnosis, and patient survival.
The age ranged from 36 to 91 years with a mean 63.4 years, the most prevalent age groups were from 51 to 60 years (30.4%) and between 61 to 70 years (30%). Four hundred and five patients (86.2%) of the studied cases were males. Smoking was recorded as a habit in 86.5% male patients. Oral cavity and laryngeal malignant tumors were the most common, 35.1% and 32.1% respectively. The most found risk factor was smoking (86.5%) followed by oral unhygienic conditions & periodontal diseases (43.6%). Squamous cell carcinoma was the most frequent histopathological type 91.3%. Early stage tumors were observed in oral cavity and laryngeal carcinomas.
This study was invariably required to show how serious the likely problem of head and neck cancer is typically and how it affects the local health system in Al-Baha area. The study revealed that smoking with its consequences is a significant risk factor for head and cancer in Al-Baha city.
Al-Baha region, SA, Head and neck cancers, Epidemiology
Head and neck cancers comprise malignancies of the upper aerodigestive tract [1]. They are usually reported together due to their epithelial origin and possible etiological relationship, ranking as the sixth most common malignancy worldwide and are expected to occur in 560,000 patients per year and cause 380,000 deaths [2]. In the United States, about 63,000 cases and 13,000 deaths were reported annually [3]. About 90% of head and neck tumors are squamous cell carcinomas, originating from the mucosal lining of upper aerodigestive tract including the lips, oral cavity, oropharynx, hypopharynx, nasal, paranasal sinuses, nasopharynx and larynx [4-7]. This heterogeneous category of malignancies has distinct epidemiological and pathological characteristics in addition to special treatment requirement. As the majorities of the patients usually diagnosed at advanced stage disease and require a multidisciplinary management [8].
The development of head and neck tumors is multifactorial as a result of some carcinogens like smoking and alcohol in addition to interaction of both environmental factors and genetic inheritance. The vast majority of patients, 85% or more, with cancer of the head and neck have a history of alcohol use, smoking, or both (including smokeless tobacco, sometimes called "chewing tobacco" or "snuff"), especially cancers of the oral cavity, oropharynx, hypopharynx, and larynx [9-11]. Other prevalent risk factors include Human papilloma virus (HPV), poor diet, certain occupations, and occupational exposures, low education and socioeconomic status, immunodeficiency, poor oral hygiene, family history of cancer and other [12-14].
Diagnosis and staging of head and neck malignancy will normally include clinical examination by an experienced clinician, fine needle aspiration (FNAC) &/or core biopsy of any neck masses, followed by further examination under anesthetic with additional operative biopsies if needed [15]. Oral lesions are evaluated with an incisional biopsy or a brush biopsy, while nasopharyngeal, oropharyngeal, or laryngeal lesions are biopsied endoscopically [16].
In High altitude region; Al-Baha City the biggest town in Al-Baha region, Saudi Arabia, there have been few or no statistical studies evaluating the prevalence and pattern of Head and Neck malignancies. The current study aims to analyses the pattern of various pathological entities of head and neck malignancies identified in patients presented to the Otorhinolaryngology Unit at King Fahd Hospital as a referral institute at Al-Baha region which include many small towns, Saudi Arabia (KSA).
This is a retrospective, cross-sectional study. Regarding to data collection; it is important to mention that no oncology center in Al-Baha region and the patients once diagnosed they referred to oncology centers in three different cities which are usually Jeddah and Makkah cities and rarely to Riyadh city. We analyzed all clinical and histological data from records of patients presented to the Otorhinolaryngology (ENT), and different surgical departments at King Fahd Hospital at Al-Baha city and other record from different referral centers were the patient usually referred to oncology centers in over ten years (January 2009-December 2019). A total of 470 patient's records were reviewed for the following variables: Age, sex, occupation, smoking and alcohol consumption habits, primary tumor location, clinical tumor stage, histological type and grade, diagnosis, and patient survival.
Tumors were classified according to the anatomical site into the oral cavity, pharynx, and larynx. The oral cavity included the lips, anterior 2/3 of the tongue, buccal mucosa, the gingiva, hard palate, and the retromolar area. The pharynx was separated into the oropharynx (including soft palate and uvula, the tonsils, and the lateral and posterior walls), the hypopharynx (including the piriform fossae, hypopharyngeal wall, the post cricoid and non-post cricoid regions), and the nasopharynx (lateral walls, choanae). The larynx is separated into three regions the supraglottic, the glottic, and the subglottic regions.
Clinical staging was carried out according to the American Joint Committee on Cancer (AJCC) sixth edition manual [17]. Descriptive analysis was used for frequencies and means.
The present study reviewed and analyzed the records of 470 patients with head and neck cancer during the period from January 2009 to December 2019. There were 405 male (86.2%) and 65 female (13.8%). The age ranged from 36 to 91 years with a mean 63.4 years and a standard deviation of 12.41 years. The age distribution of the patients for each age group was presented in Table 1. The most prevalent ages were from 51 to 60 years (30.4%) and between 61 to 70 years (30%).
Table 1: Distribution of head and neck cancer patients according to the age at Al-Baha. View Table 1
Analysis of the risk factors for head and neck cancer revealed that smoking used to be a habit in 86.5% of the studied group, oral unhygienic conditions & periodontal diseases documented in 43.6%, candida infections in 26.2%, human papillomavirus infection in 19.1% and Epstein - Barr virus-positive recorded in 52% (Figure 1). Table 2, represents the site of primary head and neck tumor, the oral cavity (35.1%) was the common primary tumor site followed by the larynx.
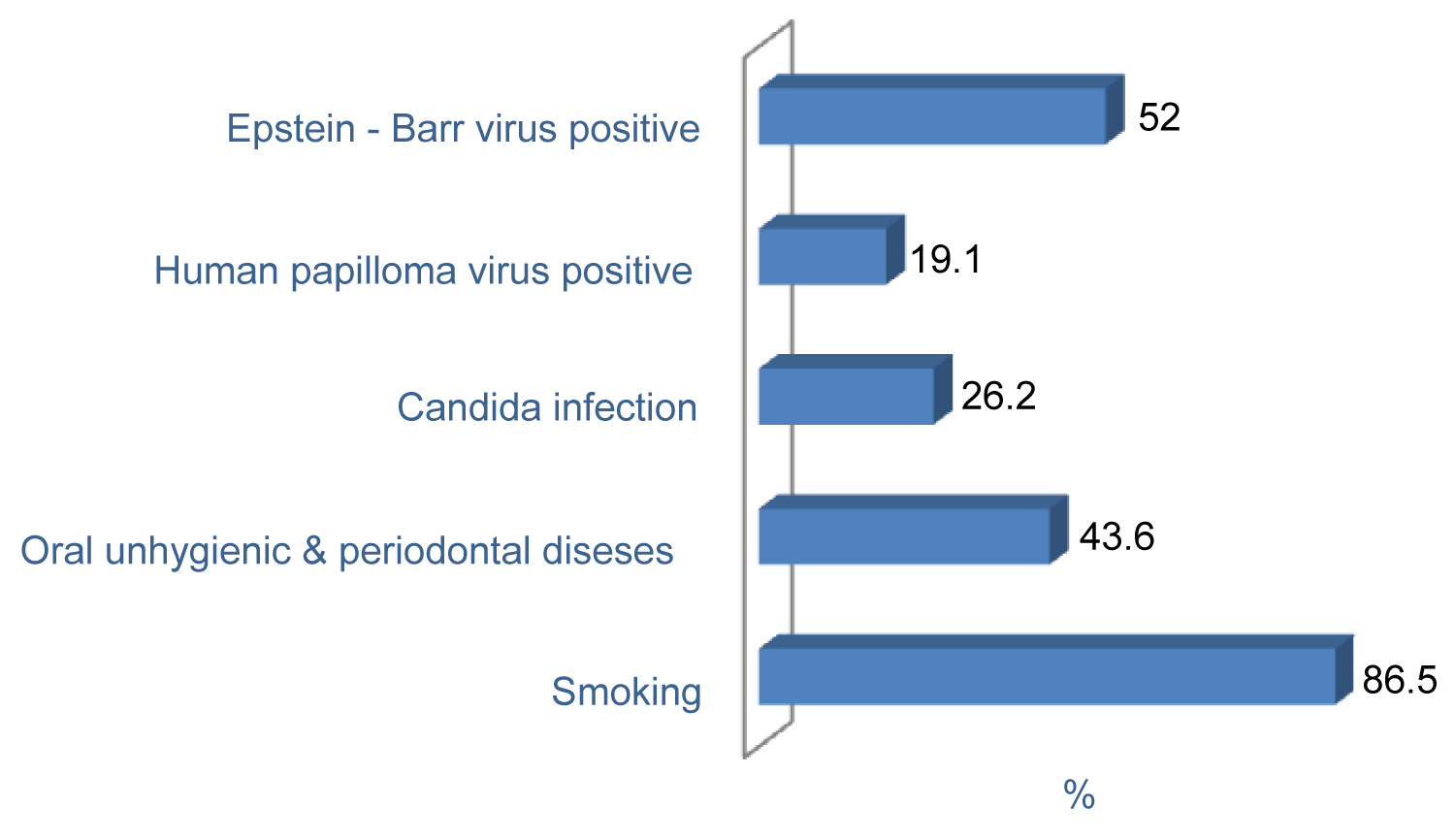 Figure 1: Recorded risk factors in head & neck cancer patients at Al-Baha.
View Figure 1
Figure 1: Recorded risk factors in head & neck cancer patients at Al-Baha.
View Figure 1
Table 2: Site of the primary tumor site in head and neck patients. View Table 2
Table 3, Table 4, and Table 5, show the frequency of clinical tumor stage (TNM) according to the site of primary tumors. Squamous cell carcinoma was the most frequent histopathological type representing 91.3% (Table 6). About 48.5% of the studied patients underwent surgery and postoperative radiotherapy.
Table 3: Distribution of the primary tumor size (T) according to the site of primary tumor. View Table 3
Table 4: Distribution of lymph node involvement (N) according to the primary tumor site. View Table 4
Table 5: The frequency of metastatic spread (M) according to the primary tumor site. View Table 5
Table 6: Distribution of Histopathological types. View Table 6
It is important to identify the prevalence of head and neck malignancy in this area and to recognize their burden on the patient. The study included 470 cases over 10 years presented King Fahd Hospital at Al-Baha City, Saudi Arabia.
The incidence of head and neck tumor in Al-Baha according to the current study was found to be about 36.5 cases per year; this may be because of many factors which include: firstly; most of the patients try seeking treatment outside Al-Baha region, which may be because of inaccessibility to an oncology services. Secondly, the awareness of Al-Baha population about these head and neck tumors needs much research and health promotion towards this critical aspect of diseases.
Our analysis showed that most patients were males (86.2%) and females (13.8%). This is agreed with most other reports that recorded a predominance of men [18]. The male predominance may be attributed to their excessive exposure to the risk factors such as smoking and its associated oral unhygienic conditions & periodontal diseases and in our study 86.5% of the studied patients were smokers [19]. Many studies reported the established link between head and neck cancer and smoking [20,21].
The average age of patients in the current study was 63.4 years. Analysis of the prevalence of head and neck cancer according to the age in our study revealed that patients in the 5th and 6th decade of life were highly affected. Our findings agree with that of Alharbi and Issing, et al. who reported an average age of 56.7 and 59.4 years respectively [22,23].
The carcinoma of the oral cavity was the most frequent type of head and neck cancer in our studied group (35.1%) followed by laryngeal cancer (32.1%). This high incidence of oral and laryngeal carcinomas may be related to the increased incidence of the smoking habit in our group. Alharbi also reported a 44.7% incidence of the oral cavity in Al-Baha region [22]. A number of reports addressed a two to threefold increase of oral cancer in smokers [24,25].
We also found that squamous cell carcinoma was the most frequent histopathological type 91.3% in line with Alharbi study [22]. Many literatures reported that over 90% of head and neck cancers are squamous cell carcinoma [26,27].
We noted oral and laryngeal cancers were presented at an early stage than the rest of the head and neck malignancies. This may be explained by the early appearance of symptoms as oral mass and hoarseness of voice. The remaining types of head and neck were presented in advanced stages which could be explained by low educational and public awareness, lack of tertiary specialized hospital, and absence of early detection and preventive programs. In addition, most of those patients did not care to follow up on their disease and treatment. Our observations support the results of Alharbi who previously reported that most of his studied head and neck group of patients presented at stage III or IV [22].
Treatment of T1 or T2 tumors is a single modalities which is traditionally surgery or radiation therapy specifically in most sites surgical except nasopharynx primarily non-surgical treatments modality but advance stages; T3 and T4 are usually multimodalities including surgery, radiotherapy, and chemotherapy with the combination of surgery and radiation therapy in the majority of patients. In the current study 48.5% of our analyzed patients managed with surgery followed by radiotherapy.
There is a lack of national cancer registry and study based on populations in the Kingdom of Saudi Arabia, so there is no evidence of the actual head and neck prevalence in the country. This study was required to show how serious the problem of head and neck cancer is and how it affects the health system in Al-Baha area.
In conclusion, the study revealed that smoking with its consequences is a significant risk factor for head and cancer in Al-Baha city. The development and implementation of various treatment and prevention strategies should be conducted by otolaryngologists, dentists, and public health practitioners. An oncology specialized center should be established to provide all multidisciplinary treatment modalities for head and neck cancer in one place.
None.
The author has no conflicts of interest to disclose.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.