Elective tracheostomy is routinely performed in conjunction with major head and neck surgery, notably during transoral robotic base of tongue resection and oral cavity/oropharyngeal resection with free flap reconstruction, due to concern for potential post-operative airway compromise. In these circumstances, the tracheostomy is typically intended to be temporary with reversal during the post-operative stay. In order to expedite tracheostomy site closure and preclude development of a tracheocutaneous fistula, we utilize a reversible tracheostomy stitch.
Elective tracheostomy is routinely performed in conjunction with major head and neck surgery due to concern for potential post-operative airway compromise. In particular, securing the airway through tracheostomy placement is often necessary for transoral robotic surgery (TORS) for base of tongue (BOT) resection and for oral cavity or oropharyngeal resections with free flap reconstruction [1-4].
For TORS BOT resection, tracheostomy may be required for circumstances in which presence of an endotracheal tube may obstruct the surgical field. Additionally, tracheostomy may be temporarily required due to post-operative airway concern secondary to post-operative edema or bleeding. In the case of oral cavity or oropharyngeal resection with free flap reconstruction, airway concerns arise secondary to post-surgical edema as well as placement of new soft and/or bony tissue in close proximity to the oral airway [3,4].
Given that tracheostomy is often necessary only intraoperatively for adequate BOT tumor exposure or post-operatively for post-surgical edema or bleeding, we have utilized a reversible tracheostomy stitch to expedite tracheostomy site closure and preclude development of a tracheocutaneous fistula.
After institutional review board approval from our institution, a retrospective review was performed of all TORS BOT resections and oral cavity/oropharyngeal resection with free flap reconstruction from April 04, 2018 through June 15, 2019, the time period at which we began performing reversible tracheostomy stitches. The reversible tracheostomy stitch is performed as follows. The trachea is exposed via the traditional surgical approach. The tracheotomy is performed via a horizontal incision between the first and second, or second and third, tracheal rings. Prior to placement of the tracheostomy, a 0 Prolene® (Ethicon, Somerville NJ) is used to suture a subperichondrial tracheal flap in a horizontal mattress fashion from superior to inferior on one side of the tracheotomy and then inferior to superior on the other side. The loose suture ends are left untied and draped out of the tracheostoma, secured to the chest by Steri-Strips™ (3M, Maplewood MN), for as long as the tracheostomy is required. When the patient is decannulated intra- or post-operatively the reversible tracheostomy stich is tied down and the suture is cut, closing the horizontal tracheotomy (Figure 1). The tracheostoma site was then loosely closed using 4-0 Vicryl® (Ethicon, Somerville NJ) in the deep dermal layer and covered with an adhesive bandage. A gauze dressing overlies this closure and the patient is instructed to cover the stoma while speaking or coughing.
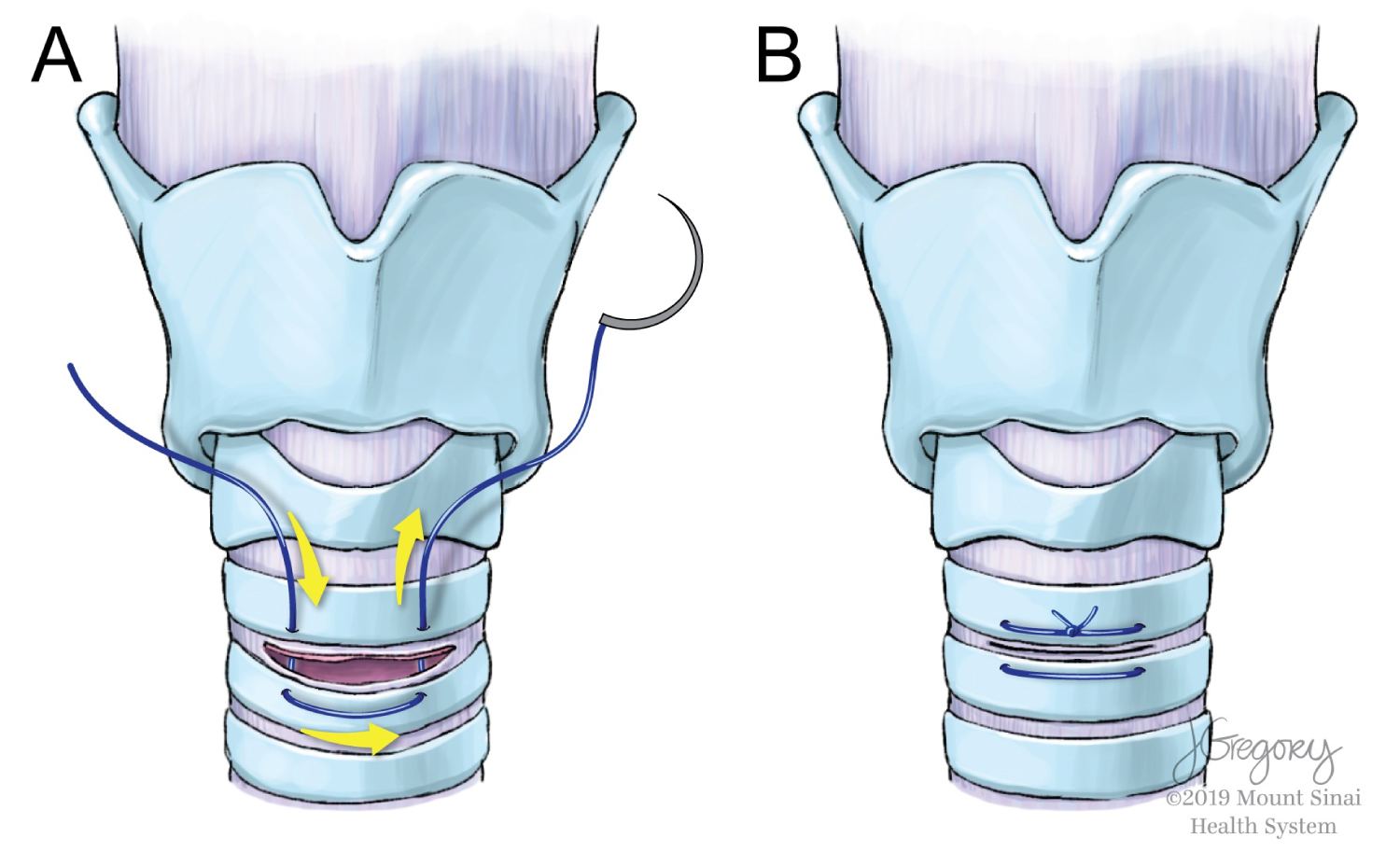 Figure 1: Reversible Tracheostomy Stitch (A) The subperichondrial tracheal flap is sutured using an 0 Prolene® (Ethicon, Somerville NJ) in a horizontal mattress fashion from superior to inferior on one side of the tracheotomy and then inferiorly to superiorly on the other side. The loose suture ends are left untied and draped out of the tracheostoma for as long as the tracheostomy is required; (B) When the patient is decannulated intra- or post-operatively the reversible tracheostomy stich is tied down and the suture is cut, closing the horizontal tracheotomy.
View Figure 1
Figure 1: Reversible Tracheostomy Stitch (A) The subperichondrial tracheal flap is sutured using an 0 Prolene® (Ethicon, Somerville NJ) in a horizontal mattress fashion from superior to inferior on one side of the tracheotomy and then inferiorly to superiorly on the other side. The loose suture ends are left untied and draped out of the tracheostoma for as long as the tracheostomy is required; (B) When the patient is decannulated intra- or post-operatively the reversible tracheostomy stich is tied down and the suture is cut, closing the horizontal tracheotomy.
View Figure 1
On retrospective review, a total of 8 patients underwent tracheostomy placement with a reversible tracheostomy stitch. One patient who underwent a TORS BOT resection had a tracheostomy placed at the onset of the case which was reversed intra-operatively following tumor resection. The remaining patients included three patients who underwent glossectomy and mandibulectomy, two with maxillectomy, and one case each with soft palate resection and reconstruction and laser supraglottoplasty for severe pharyngeal radiation-induced stenosis. The average time from tracheostomy placement to decannulation in this group was 2.5 days (range 0-5 days). All patients were noted to have healed tracheostoma sites by the time of initial post-operative office visit within 3 weeks of surgery. There were no complications associated with tracheostomy or tracheostomy reversal.
Rates of tracheocutaneous fistula in adults vary widely in the literature with some authors advocating for closure of the tracheostoma by re-approximating skin edges with sutures or applying tape across the site [5]. However, we are unaware of any prior reported techniques of closing the trachea during routine decannulation.
This case series demonstrates the possible utility of a tracheostomy stitch in cases where quick decannulation is expected. In particular, this technique is ideal for closure of tracheostomy needed only intra-operatively, such as during a TORS BOT resection during which presence of an endotracheal tube may hinder the procedure. Similarly, the reversible tracheostomy stitch may be useful in association with oral cavity or oropharyngeal resections with free flap reconstruction, for which the tracheostomy is expected to be necessary only for a few days peri- and post-operatively.
In terms of patient selection, we have found that this technique is best accomplished during cases with good exposure of the trachea intra-operatively and in patients with adequate pulmonary reserve, allowing for placement of the reversible tracheostomy sutures during temporary pauses in ventilation.
Overall, the reversible tracheostomy stitch represents a novel method of potentially expedited tracheostomy site closure in a selected patient population.
• Tracheostomy is routinely performed to secure the airway during the intra-operative and immediate post-operative period for TORS BOT resection and oral cavity resection with free flap reconstruction.
• The reversible tracheostomy stitch is a novel method of performing tracheostomy that may help expedite tracheostoma site closure and prevent formation of persistent tracheocutaneous fistula in this population.
• We have found that this technique is best suited during cases with good exposure of the trachea and in patients with adequate pulmonary reserve, allowing for temporary pauses in ventilation so that the reversible tracheostomy stitches can be placed.
There are no financial disclosures or conflicts of interest.