Open rhinoplasty, Aneurysmal fibrous histiocytoma, Aneurysmal dermatofibroma, Nasal tip mass
Aneurysmal fibrous histiocytoma (AFH), also known as aneurysmal dermatofibroma, is a rare variant of the more common and benign dermatofibroma (fibrous histiocytoma). AFHs account for approximately 2% of all cutaneous fibrous histiocytomas, and have been reported to occur most often on the extremities of young to middle aged adults, with a slight female predominance [1,2]. To our knowledge, an AFH of the face has only been reported once in the literature and was found on the forehead.
Fibrous histiocytomas are generally considered to be benign lesions, however, they have a local recurrence rate as high as 20% and a subset is also believed to have malignant potential [3-5].
Although many surgical approaches to excise cutaneous and subcutaneous lesions have been described, including Moh's micrographic surgery [4], special consideration is needed when approaching lesions in the face [6]. We will present an underutilized approach to this subcutaneous supratip lesion via an open rhinoplasty approach. The open rhinoplasty approach allowed for complete excision of the mass while simultaneously avoiding a scar in one of the most conspicuous subunits of the face.
A 24-year-old female with a past medical history significant for asthma and Crohn's disease on adalimumab presented to the senior author's office with a painless supratip mass that fluctuated in size and had been present for 6 months despite oral antibiotics and topical steroid creams. Examination of the nose revealed a non-tender, subcutaneous, soft, smooth, raised, round mass in the right supratip region, measuring 8 mm in diameter. The mass appeared cystic on bimanual palpation of the right nostril and ala (Figure 1). Preoperative computed tomography (CT) with contrast was obtained to evaluate the relationship of the mass to the nasal bones. This revealed an asymmetric, enhancing soft tissue swelling of the right nasal tip measuring 8 mm × 9 mm × 4 mm (CC × AP × TR) without involvement of the nasal bones (Figure 1). Based on imaging alone, the differential diagnosis included dermoid cyst, sebaceous hyperplasia and fibrous papule.
 Figure 1: Preoperative photo showing a non-tender, subcutaneous, soft, smooth, raised, round mass in the right supratip region, measuring 8 mm in diameter (Left).
Figure 1: Preoperative photo showing a non-tender, subcutaneous, soft, smooth, raised, round mass in the right supratip region, measuring 8 mm in diameter (Left).
CT with IV contrast showing axial (middle) and coronal (right) images of the enhancing nodular nasal mass measuring 8 mm × 9 mm × 4 mm (CC × AP × TR). The mass was situated over the right nasal cartilage without involvement of the nasal bones or sinuses.
View Figure 1
The mass was excised en bloc using an open rhinoplasty approach. Once the nasal skin-SMAS envelope was elevated, a lobular, cystic appearing mass was again noted in the right supratip area lateral to the upper lateral cartilage. The cephalic margin of the mass was fused onto the upper lateral cartilage and was sharply separated (Figure 2).
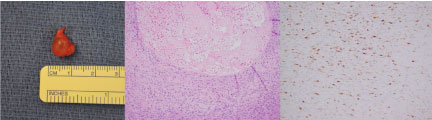 Figure 2: Left: Resected mass. Histological cross section of resected mass showing characteristic features of an aneurysmal fibrous histiocytoma.
Figure 2: Left: Resected mass. Histological cross section of resected mass showing characteristic features of an aneurysmal fibrous histiocytoma.
Middle: A cystic space filled with blood products, amplification 10×).
Right: Immunohistochemistry: Factor XIIIa (histiocyte marker), amplification 20×. View Figure 2
Final pathology revealed a spindle cell lesion with cystic spaces with fibrin and blood contents, consistent with an aneurysmal fibrous histiocytoma (Figure 2). The tumor cells were partially and weakly positive for smooth muscle actin, factor XIIIa, CD68; and negative for CD34, S- 100, Bcl-2, and cytokeratin AE1/AE3.
Aneurysmal fibrous histiocytoma is a rare variant of the cutaneous fibrous histiocytoma with distinctive clinical and pathologic features. AFHs are confined to the dermis and have a cystic consistency, and are blue, black or dark red in appearance. They are generally < 1 cm in diameter and can quickly expand and change in color as blood extravasates into the tumor. In our patient, the typical dark red appearance could not be appreciated until after the nose was opened.
Any transcutaneous approach, including a Moh's excision, would have left a significant defect in the nasal tip. However, the open rhinoplasty approach allowed for optimum visualization while obviating the need for reconstruction after the mass was excised.
The patient had an excellent postoperative cosmetic result and has not had recurrence at two-year post-operatively.
We report the first case of nasal aneurysmal fibrous histiocytoma. The open rhinoplasty approach provided excellent exposure of the lesion intraoperatively and optimized postoperative cosmesis.