Congenital cholesteatoma (CC) is a rare disease, it accounts for 2-5% of all cholesteatomas most common site being middle ear.
A 23-year-old female presented with progressive left sided facial asymmetry for 4 years and progressive hearing loss in the left ear for 2 years. She had normal left tympanic membrane and complete left lower motor neuron facial nerve palsy. High resolution computed tomography (HRCT) and magnetic resonance imaging (MRI) temporal bone showed extensive bony destruction, petrous apex and soft tissue lesion.
Patient then proceed with transmastoid translabyrinthine approach. Diagnosis of cholesteatoma confirmed by histopathological examination (HPE).
CC of petrous apex is a rare case. It is a challenge to diagnose CC pre-operatively without specific radiological sign. This is because the disease is generally difficult to differentiate with mucocele and cholesterol granuloma on CT and MRI scan. Therefore, intraoperative diagnosis more accurate rather than the preoperative diagnosis.
CC is one of the rare diseases of temporal bone. However, this disease rarely involves the petrous apex. In addition, it needs to be differentiated from the cerebellopontine angle lesion and the petrous apex's lesions such as acoustic neuroma, epidermis cyst, mucocele, archanoid cyst and cholesterol granuloma. Generally, the incidence involving CC is estimated to be around 2-5 percent of all the cases involving cholesteatoma, where the reported ratio of male to female predominance is 3:1 [1]. Moreover, even in a normal temporal bone, it has been discovered that the CC can occur even in the absence of otorrhoea. The first symptom of the disease is the facial nerve deficit then the unilateral sensorineural hearing loss [1]. In order to investigate various lesions which are involving the cerebellopontine angle, CT and MRI scan recommended, and it is one of most important investigative tools. However, cholesteatoma is very difficult to diagnose because it does not have specific radiological sign [2]. There are several surgical approaches for petrous lesion. The middle cranial fossa approach and retro mastoid approach are preferred by neurosurgeons, and the transmastoid translabyrinthine approach is preferred by otologists.
A twenty-three-year-old female patient presented with progressive left sided facial asymmetry in the past 4 years to complete facial nerve palsy and progressive hearing loss left ear in the past 2 years.
She was treated at peripheral clinic as Bell's palsy. After 1 year, she noticed that facial asymmetry worsening. So, she decided to seek treatment at a hospital, only then patient was referred to us after performing HRCT and magnetic resonance imaging (MRI) mastoid with suspicious of cholesteatoma.
Complete ear, nose and throat evaluation revealed normal tympanic membrane left side with complete left lower motor facial nerve palsy and severe sensorineural hearing loss in the left ear on pure tone audiogram.
Cerebellar sign was negative. HRCT and MRI temporal bone revealed sclerosis of the mastoid bone with loss of mastoid air cells due to chronic mastoiditis. Soft tissue lesion and some fluid in the left middle ear and the attic of the tympanic canal. The left Eustachian tube also occluded with soft tissue lesion or secretion and does not enhance with intravenous contrast. There is bony erosion in the tegmen tympani and expansion of the petrous bone (Figure 1 and Figure 2). This finding suggest cholesteatoma in the left middle ear with erosion of the petrous bone and involvement of the left facial nerve canal. Patient then procced for transmastoid translabyrinthine approach.
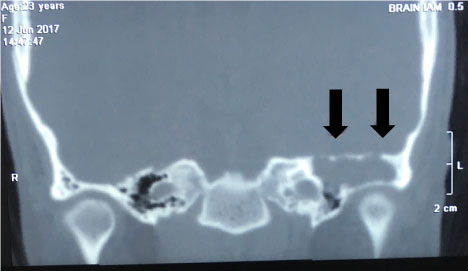 Figure 1: CT mastoid. Shows bony expansion of the petrous bone with soft tissue lesion in the tympanic cavity and attic. View Figure 1
Figure 1: CT mastoid. Shows bony expansion of the petrous bone with soft tissue lesion in the tympanic cavity and attic. View Figure 1
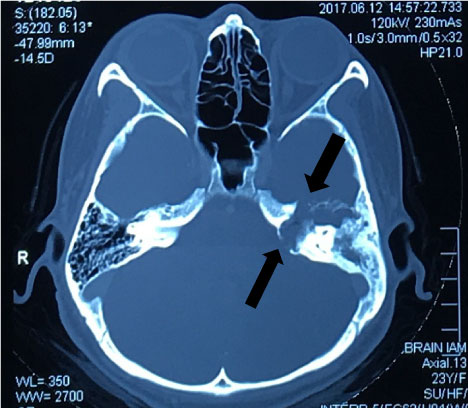 Figure 2: MRI brain and internal acoustic meatus (IAM). Shows bony expansion of the petrous bone with soft tissue lesion in the tympanic cavity and attic. View Figure 2
Figure 2: MRI brain and internal acoustic meatus (IAM). Shows bony expansion of the petrous bone with soft tissue lesion in the tympanic cavity and attic. View Figure 2
Intraoperative finding showed that cholesteatoma occupying petrous apex of temporal bone, dura, tegmen tympani and superior posterior cranial fossa exposed. Long process of incus, stapes and oval window eroded. Tympanic part of facial nerve damaged. Neuroma at proximal part of chorda tympany noticed. Temporomandibular joint exposed. In this patient, we did not try for nerve repair or grafting as symptom of facial paralysis persist more than 6 months. Cholesteatoma completely removed. Diagnosis of cholesteatoma confirmed by HPE taken intraoperative.
Post-operative patient was kept in ward for 2 days for intravenous antibiotic and close monitor. Regular follow up and 6 monthly MRI planned for this patient.
The diagnosis of Bell's palsy if often regarded as a diagnosis of exclusion, thus all patients must be check thoroughly to find the cause [3]. In this case, the patient has CC of petrous apex. This disease can be either acquired or congenital. However, it is believed that the CC of petrous apex is caused by the resting squamous cell [1]. The disease described as congenital when it manifests itself without a past history of trauma or infection with intact and located behind the tympanic membrane [4]. This disease is destructive in nature; most of CC appear to be asymptomatic and appear to be innocuous keratin pearl. In severe conditions, they can enlarge and caused serious complications that include the ossicular destruction, base of skull complications and facial paralysis [4]. Patients suffering from CC often have symptoms which are dependent on the direction of the extension of the disease. Those who are suffering from posterior mesotympanum lesions usually anticipated that conductive deafness will be present owing to the ossicles' earlier erosion [5].
As mention earlier, it is a challenge to diagnose CC by using radiological investigation. This is because the disease is generally difficult to differentiate with mucocele and cholesterol granuloma on CT and MRI scan. Therefore, this case preferred intraoperative diagnosis rather than the pre-operative one due to such challenges [6].
To remove the cholesteatoma of the petrous apex, transmastoid translabyrinthine method is the most basic technique to be considered, with or without transcochlear technique. However, these techniques cannot adequately remove cholesteatoma that is located deep down the petrous apex, which is fixed firmly onto the middle cranial fossa dura. In this case, the middle cranial fossa approach can be effective method [6].
In our case, we proceed with transmastoid translabyrinthine approach to remove the entire disease deep down the middle of the cranial fossa dura. This is possible through performing the partial labyrinthectomy. However, we are not considering for cochlea's preservation and the vestibular function during the removal extensive cholesteatoma of petrous apex.
In cases where damage to the facial nerve in the extensive cholesteatoma of petrous apex, the existing literature seem to favor sacrificing the official nerve having the residual function needed for complete removal [7].
It is however, not recommended to completely obliterate the cavity because there could be residual cholesteatoma as well its complications such as the rapture of dura, jugular valve and the internal carotid artery. If cholesteatoma recurs, it would be difficult to investigate it in the obliterated cavity through CT and MRI [8].
CC of petrous apex is a rare disease of temporal bone. Early diagnose of CC will reduce the damage and high chances to preserve the facial nerve. With no specific radiological signs, it is difficult for surgeon to diagnose pre-operatively.
Careful surgical planning is very important to avoid injury to any adjacent tissues and structures, a multidisciplinary approach is warranted. A team of experienced surgeons from varying fields including otolaryngology, neuro-otology and neurosurgeon will help to ensure a successful surgical outcome.
We have no conflict of interest to declare.