Squamous cell carcinoma in pinna and external auditory canal is rare and aggressive variant of cell carcinoma. We report the case of squamous cell carcinoma in pinna and external auditory canal.
The case is presented, along with a brief literature review concerning squamous cell carcinoma in pinna and external auditory canal.
The patient experienced locally invasive squamous cell carcinoma in his right pinna and external canal with invasive of the right parotid, temporomandibular joint, external auditory canal and middle ear, and the metastasis of the right neck lymph node. Biopsy in the operating theatre revealed a squamous cell carcinoma.
This is the case to be rarely reported in the literature. Aggressive management with surgical resection and treatment with appropriate intravenous antibiotics is necessary to give the best chance for cure.
Squamous cell carcinoma (SCC), Pinna, External auditory canal
Squamous cell carcinomas (SCC) arise from the skin of the external auditory canal and are relatively rare entities [1]. Primary carcinoma of the pinna and external canal is rare and the prognosis is ominous except for those cases diagnosed incidentally following external otitis. They may be related to chronic infection, radiation exposure, and sun or cold exposure.
Both squamous cell carcinomas of the external auditory canal and malignant otitis externa can present with a painful, discharging ear with granulation tissue involving the external canal refractory to initial antimicrobial therapy [2]. However, the challenging anatomical location and invasive nature makes this type of cancer extremely difficult to treat, particularly in more advanced stages [3].
There is no established consensus on treatment because of the limited number of cases of squamous cell carcinoma pinna and external canal.
The most frequently reported treatment involves surgical resection with or without adjuvant radiotherapy. Chemotherapy, brachytherapy or alternative treatment methods such as superselective intra-arterial chemotherapy injection have been described in the literature, however, their exact role remains to be determined [4,5]. We present here a patient with squamous cell carcinoma of the pinna and external auditory canal, and discuss the challenges associated with the diagnosis and treatment of the disease, and review the literature for trends while outlining the most beneficial treatment strategy for this patient population.
A 42-year-old Chinese man presented with a eight- years history of right sided otalgia and discharge. The patient have not a history of ultraviolet light exposure, thermal injury (cold), radiation exposure. He has the chronic infection of the external auditory canal. At the beginning, the treatment included ear toilet with dry suction, pain control, and topical antibiotics. The neoplasm initially was the size of peanut, and gradually increased about 4 cm × 5 cm. And the patient was with the sense of hearing loss, ear fullness which resembled, otalgia, itching. He was admitted to our hospital.
On examination, the patient's symptoms were associated with right auricle having irregular cauliflower-like uneven neoplasm with stench and yellowish-white discharge, and the ulcer was easy bleeding, which size was 5 cm × 6 cm, and the sign with right supraclavicular fossa palpation of swollen and movable lymph nodes which size was about 1 cm × 1 cm (Figure 1).
 Figure 1: Photographs of case squamous cell carcinoma in pinna and external auditory canal. Published with patient's permission. View Figure 1
Figure 1: Photographs of case squamous cell carcinoma in pinna and external auditory canal. Published with patient's permission. View Figure 1
Computed tomography revealed a tumor mass filling his right pinna and external auditory canal and infiltrating the right parotid, temporomandibular joint, external auditory canal and middle ear, and the metastasis of the right neck lymph node (Figure 2). No abnormality was found on clinical examination, including neurotological examination, the chest roentgenogram, nasoendoscopy and laryngoscopy.
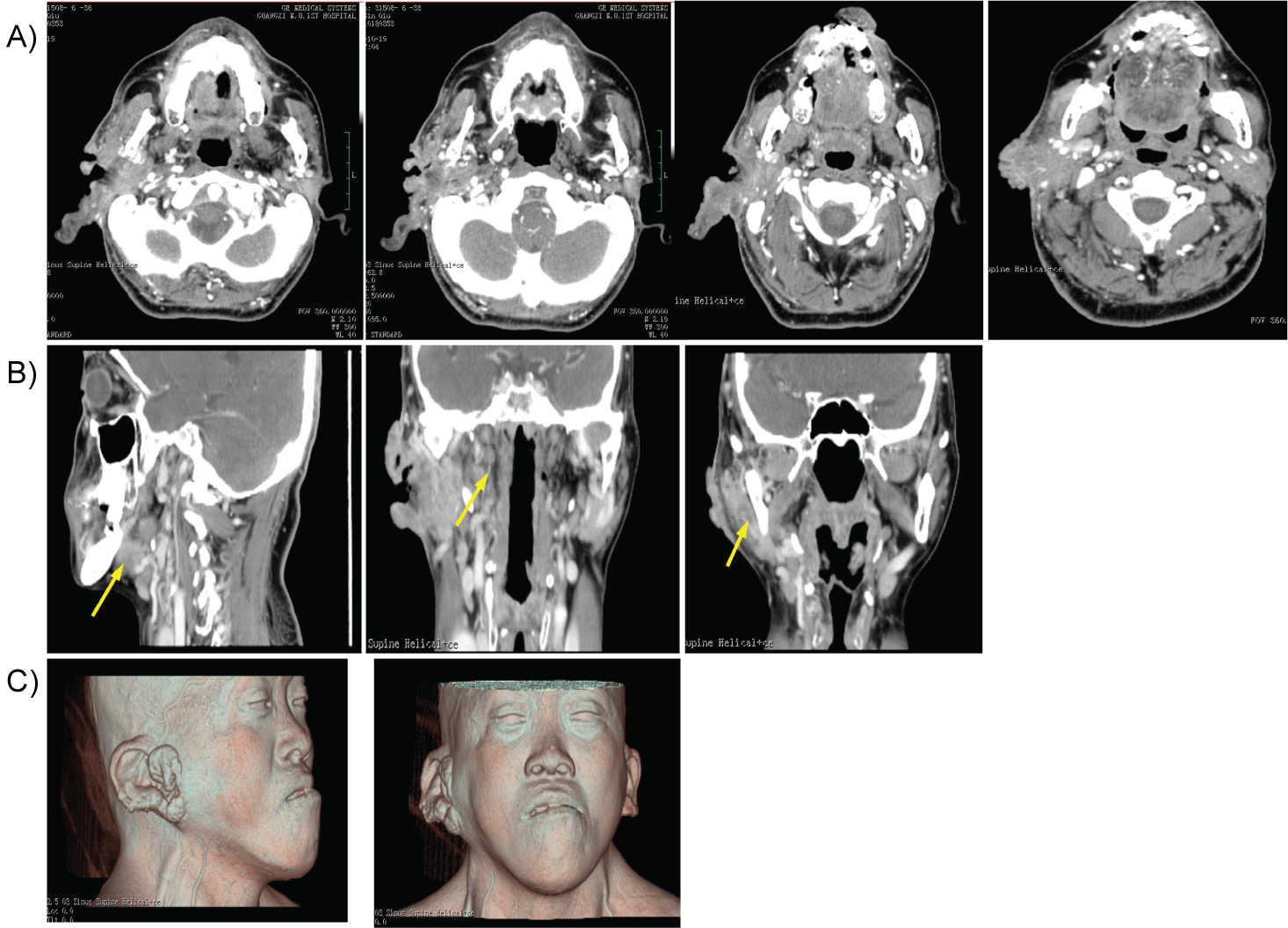 Figure 2: Contrast-enhanced computed tomography scans. a) Contrast-enhanced computed tomography reveals a right in pinna and external auditory canal, and shows a large soft tissue mass extending to the floor of the right middle cranial fossa with mild mass effect on the inferior temporal lobe. Destruction of the right parotid, mandibular condyle, temporomandibular joint, external auditory canal and middle ear are evident with the neck lymph node metastasis .The left pterygoid muscle and Temporomandibular joint are also involved in the malignant process; b) Coronal and sagittal CT scanning reveals the destruction of submandibular gland and lymph, parapharyngeal space, masseter; c) 3D computed tomography reveals the neoplasm. View Figure 2
Figure 2: Contrast-enhanced computed tomography scans. a) Contrast-enhanced computed tomography reveals a right in pinna and external auditory canal, and shows a large soft tissue mass extending to the floor of the right middle cranial fossa with mild mass effect on the inferior temporal lobe. Destruction of the right parotid, mandibular condyle, temporomandibular joint, external auditory canal and middle ear are evident with the neck lymph node metastasis .The left pterygoid muscle and Temporomandibular joint are also involved in the malignant process; b) Coronal and sagittal CT scanning reveals the destruction of submandibular gland and lymph, parapharyngeal space, masseter; c) 3D computed tomography reveals the neoplasm. View Figure 2
On histopathological examination demonstrated an inflamed stratified squamous epithelium with dysplasia and cellular atypia. Within this, there were embedded irregular nests of atypical squamous cells infiltrating the underlying stroma (Figure 3). Based on the Pittsburgh staging system, the diagnosis of a stage VI squamous cell carcinoma was made [6].
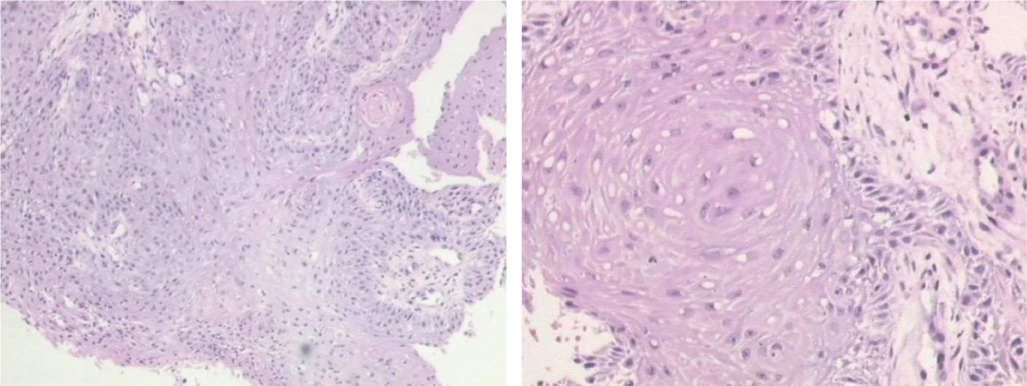 Figure 3: Histological images. (squamous cell carcinoma type II) On histopathological examination demonstrated an inflamed stratified squamous epithelium with dysplasia and cellular atypia. Within this, there were embedded irregular nests of atypical squamous cells infiltrating the underlying stroma. View Figure 3
Figure 3: Histological images. (squamous cell carcinoma type II) On histopathological examination demonstrated an inflamed stratified squamous epithelium with dysplasia and cellular atypia. Within this, there were embedded irregular nests of atypical squamous cells infiltrating the underlying stroma. View Figure 3
Considering the advanced stage, the patient was deemed not to be a surgical candidate. He don't received a course of specific palliative radio -therapy for advanced head and neck cancer, with concurrent carboplatin radiosensitization because of the economic reason.
Squamous cell carcinoma (SCC) of the external auditory canal is an rare malignant carcinoma [7] that arises from the external ear and spreads to the temporal bone and surrounding sites. Periauricular soft tissues, the parotid gland, temporomandibular joint and mastoid are common sites of tumour progression. The carotid canal, jugular foramen, dura, middle and posterior cranial fossae are invaded in advanced stages. Ear pain and discharge may initially be mistaken for external otitis [8]. Involvement of the ear and lateral skull base by squamous cell carcinoma is usually the result of a cutaneous neoplasm that originates from the skin of the pinna or the external auditory canal. Ultraviolet light exposure or thermal injury (cold) and radiation exposure and chronic infection are thought to predispose patients to this disease [2,9]. The lack of a unifying classification system in the past, along with the rarity of the disease has made the development of clear treatment guidelines difficult.
Aggressive surgery with postoperative radiation is the usual treatment [10,11]. The complex anatomy and changing relationships between the tumour and contiguous tissues within a limited space make it complicated for surgery to achieve tumour-free margins. There has been a slow evolution of the treatment of squamous cell carcinoma in pinna and external auditory canal [12]. Treatment of squamous carcinomas of the external canal should be aggressive because of the high rate of recurrence. Treatment with en-block resection, selective neck dissection, and radiotherapy is recommended in cases if the patient would like, as recurrence rates and nodal metastasis are relatively high. However, the prevention was important. Appropriate clothing, sunscreen with at least SPF 30, and avoidance of intense sun exposure may prevent skin cancer [13]. This case and the other cases [14-16] reported in the literature highlight the importance of surgery and biopsy in the investigation and diagnosis of squamous cell carcinoma in pinna and external auditory canal when the cause is a chronic infection of the external auditory canal (malignant or necrotizing otitis externa) refractory to standard treatment regimes. Successful diagnosis and management of both these pathologies involve a multidisciplinary team approach and a meticulous unification of a detailed clinical examination, laboratory investigations, appropriate radiology, and biopsy to create a complete clinical picture.
Hence, in this report, we describe a case of a rare and aggressive tumor type for which the most beneficial therapeutic approach remains to be determined. It is clear however, that, if diagnosed late, this disease exhibits poor outcomes, while it is associated with higher response rates and increased survival at early stages. Thus, emphasis should be placed on the importance of early detection, diagnosis and treatment of squamous cell carcinoma of the temporal bone and middle ear as the simplest and most effective measure to increase patient survival.
Squamous cell carcinoma in pinna and external canal is a rare disease of skin malignant tumor. It is likely to be under-reported. Emphasis should be placed on the importance of early detection, diagnosis and treatment of squamous cell carcinoma of the in pinna and external auditory canal as the simplest and most effective measure to increase patient survival.