Background: Acute kidney injury is an important risk factor for morbidity and mortality during critical illness notably in very old patients admitted to intensive care units. This study was performed to identify prognosticators for these patients.
Methods: This single-center retrospective study is based on a patient registry of a medical intensive care unit. Hospital records of patients aged 80 years or older who were admitted between 2005 and 2015 were examined. Patients who developed AKI according to KDIGO guidelines within 4 days after admission were included in this study.
Results: Ninety six (96) patients with AKI and 81 age- and gender-matched controls without AKI were included in this study. Mean APACHE II score was 30 with an ICU mortality of 27% in very old patients with AKI. The odds ratio to die in hospital for these patients was 5.02 in comparison to controls (49 vs 16%). APACHE II score and fluid balance in the first 2 days of ICU admission were the strongest predictors of ICU mortality with an AUROC of 0.76. Of the 47 patients with AKI who survived hospital admission, 30 were discharged home.
Conclusion: Mortality is increased in very old ICU patients with AKI. Among survivors, two-thirds returned home.
Very old, Intensive care, Acute kidney injury, Fluid overload
AKI = acute kidney injury; CKD = Chronic kidney disease; VOP = very old patients; RRT = renal replacement therapy; MICU = medical intensive care unit.
Acute kidney injury (AKI) is a risk factor for morbidity and mortality during critical illness [1]. Age-related changes in renal anatomy and physiology expose very old intensive care patients (VOPs, age ≥ 80 years) to an increased risk for AKI [2]. Moreover, multimorbidity and polypharmacy, which are prevalent in this age group, may further increase that risk. There is limited information about the short and long-term mortality in these patients after AKI. Prognostication is still based on studies which involved younger patients [3] and, hence, may be imprecise when applied to the very old.
Intensive care can provide a survival benefit to some VOPs [4]. However, this group of patients is very heterogeneous regarding resilience and response to intensive care treatment. Importantly, elderly survivors of AKI often have a reduced functional capacity and quality of life after discharge from hospital. They consume substantially greater healthcare resources than the general population as a result of longer hospitalizations as well as rehospitalizations [5]. Thus, a robust decision-making becomes especially important in VOPs to prevent inappropriate interventions [6] or underutilisation of appropriate technologies. Chronological age is considered a poor predictor of outcome [7]. Additional predictors, that would ideally be available early in the course of a critical illness, are required to inform decision-making. This study investigated prognosticators in VOPs who developed AKI within 4 days of admission to a medical intensive care unit.
A retrospective review of the medical intensive care unit (MICU) database and charts as well as the electronic health records system of the Hadassah University hospital was performed on patients 80 years and older (VOPs) admitted to the MICU between 1 January 2005 and 31 December 2015. Length of survival was determined from hospital files or from Ministry of Interior records. Permission was obtained from the Hadassah Hebrew University Medical Center review board (Approval number 0157-17-HMO). We screened for patients 80 years of age or older who were transferred to MICU within 72 hours of hospital admission and had a serum creatinine level of 140 µmol/l or higher. This value represents a 1.5 fold increase in the upper limit of the normal range for creatinine in the hospital and is the upper limit for initial scoring using the APACHE II score. The range for hospital admission creatinine values for this group was 42 to 798 µmol/l. These patients were then rechecked to confirm that they fulfilled the criteria for AKI according to the KDIGO guidelines [8] within the first 4 days after ICU admission. Both creatinine and urine output criteria were used. Urine output criteria was based on an estimated 80 kg body weight (less than 40 mls / hr = urine output of 0.5 mls/kg/hr) for all patients. Patients who were on chronic dialysis, or who were discharged from ICU within 24 hours or required renal replacement therapy (RRT) within 24 hours of ICU admission were excluded (Figure 1). These patients were excluded as 24 hours is insufficient time to investigate the effect of parameters on predictive modelling, e.g. fluid balance. The control group consisted of age and gender matched VOPs who were not in AKI or who were not receiving chronic dialysis.
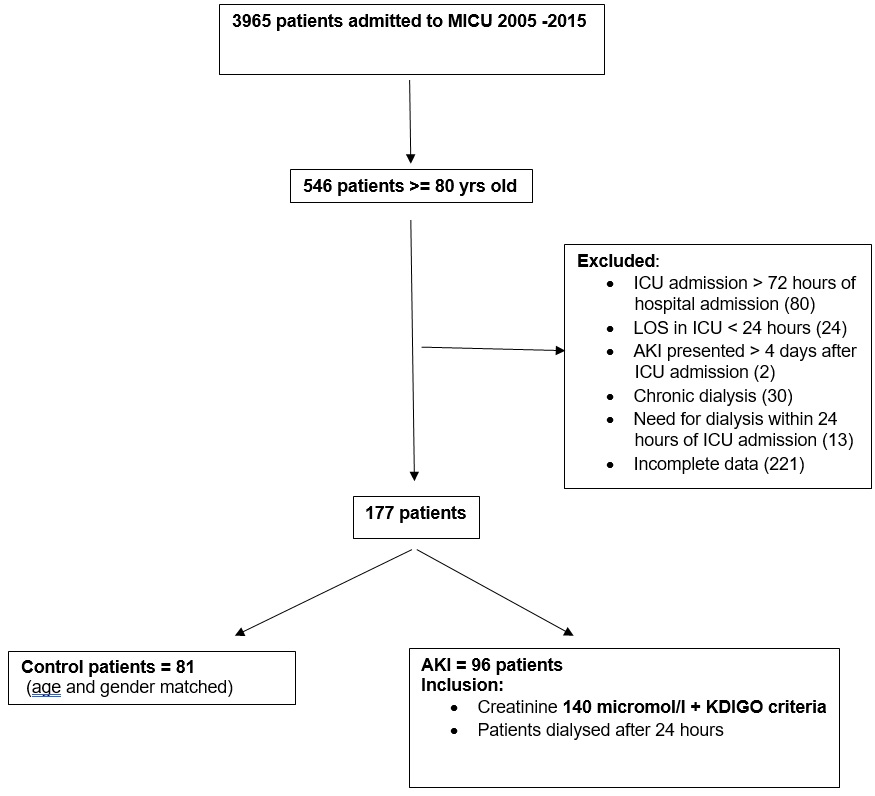 Figure 1: Flow chart indicating the inclusion and exclusion criteria.
View Figure 1
Figure 1: Flow chart indicating the inclusion and exclusion criteria.
View Figure 1
Statistical analysis was performed using JMP_Pro version 14 (SAS Institute Inc.). The distribution of continuous variables is presented as means and standard deviation (SD) for normally distributed data and as medians and ranges for all other data. Comparison of normally distributed continuous variables between groups was performed using Student’s t-test. The Wilcoxon signed rank test was used for comparing other continuous variables. Comparison of categorical values was performed using the chi-square test. A p-value of < 0.05 was considered statistically significant. Kaplan-Meier analysis was performed comparing long-term survival between groups. Cox regression analysis was used to evaluate parameters influencing survival. The area under the receiver operating characteristic curve (AUROC) for the Cox regression analysis was calculated including the 95% confidence interval (CI).
During the period 2005 - 2015, 546 (14.2%) out of the 3965 patients admitted to the MICU were 80 years or older (VOP). Of these, 96 (17.6%) fulfilled the inclusion criteria for this study (Figure 1). Of note, 23 patients with AKI who were admitted to ICU for less than 24 hours, and were therefore excluded from the study group, 18 (78%) died during their ICU admission. Also, of the 13 patients who were dialysed during the first 24 hours of admission, 6 (46%) died in ICU and the remaining 7 patients were weaned from dialysis in ICU and survived till hospital discharge.
A further 81 VOPs without AKI were included in a control group. The demographic data as well as admission diagnoses and chronic co-morbidities for both groups are shown in Table 1. Apart from renal conditions, infections were significantly less prevalent in the control group. The overall severity of the critical condition as documented by the APACHE II score was significantly lower in the control group. When the APACHE II score was calculated without the renal component for both groups, the APACHE II score was still significantly lower in the control group (Table 1).
Mortality was significantly increased and median time of survival was significantly decreased in patients with AKI in comparison to controls (Table 1). The odds ratio to die in hospital in the presence of AKI was 5.02 (CI 2.45 - 10.26) in comparison to patients without AKI.
Table 1: Patients’ characteristics and outcome.View Table 1
To match for severity of illness, a sub-group of the control patients with a mean APACHE II of 30 (N = 24) was extracted and ICU and hospital outcomes in these patients were compared with outcomes in the AKI group. Although there was a tendency for an increased ICU and hospital mortality in the AKI group (28% vs 25% for ICU mortality respectively, 49% vs 38% for hospital mortality respectively) this did not reach statistical significance.
Twenty of the patients with AKI (20.8%) required RRT during their ICU stay. Fourteen of these patients started dialysis within the first 2 days of ICU admission. Eleven (72%) of the patients on RRT died in hospital, 8 of those in ICU.
Within the group of patients with AKI, there was no significant difference in age, prevalence of CKD between survivors and non-survivors of ICU or hospital care. The KDIGO stage and peak levels of serum creatinine were not statistically different between these two groups (Table 2). Patients who were exposed to nephrotoxins including aminoglycosides, contrast media, NSAIDs had a significantly lower hospital survival (12 vs 37, p = 0.001). Moreover, the fluid balance differed significantly between survivors and non-survivors both after 2 and 4 days. On day 2, non-survivors had a fluid balance of more than 2 litres greater than the survivors did. On day 4, the difference was even greater with non-survivors having over a 3 litre positive fluid balance. (Table 2).
Table 2: Patients with AKI: characteristics of survivors vs. non-survivors. View Table 2
Table 3 shows the discrimination of various models for survival prediction by their AUROC. The most inclusive model includes fluid balance and APACHE II.
Table 3: Area under the curve obtained by logistic regression models for ICU and hospital mortality. View Table 3
Of the 47 patients with AKI who survived hospital admission, 30 (63%) were discharged home, 2 (4%) were discharged to a long-term ventilation facility and 15 (32%) were discharged to various levels of nursing care homes. Only 1 patient continued dialysis post discharge and 2 patients in the AKI group started dialysis within 6 months of discharge.
AKI is an established predictor of morbidity and mortality in ICU patients [9]. The prevalence of AKI in adults is difficult to estimate, due to differences in the implementation of diagnostic criteria, but may be as high as 66% [9]. It constitutes a substantial challenge in very elderly patients, since advanced age is a risk factor for both developing AKI as well as for morbidity and mortality after AKI [9,10]. AKI in these patients involves a variety of pathophysiological processes [9] proceeding on the background of aged kidneys whicH are characterized by an altered tolerance to hypoxia and inflammatory insults [11]. Moreover, interactions with other acute conditions is most pronounced in the context of multimorbidity which is found in 90% of VOPs [12] and may have an additional impact on long-term outcome [13]. Despite the importance of these topics, there are only few studies which investigated the sequelae of AKI in the very elderly [10,14,15]. In this retrospective study on VOPs with AKI, we have found a significantly reduced survival in the short and long term in comparison to age- and gender-matched controls without AKI. Both groups of patients showed a similar distribution of chronic comorbidities except for CKD. Of note, there is a large variation of reported data between AKI studies despite standardized criteria (KDIGO guidelines [8] to diagnose this condition [9]. The variability of the case mix within the investigated patient populations is a major source for that heterogeneity and underlines the importance of appropriate control groups for the assessment of risk factors and outcome measures.
The odds ratio for hospital mortality in VOPs that is due to AKI was found to be 5 in our study. This is higher than previously reported in a large study on hospitalized elderly patients [16]. However, the patients in the report by Ishani, et al. were younger and managed outside intensive care units. To some extent, the increase of mortality due to AKI could reflect the increased severity of the critical condition with AKI being an early visible marker. This hypothesis is supported by the finding that the quantitative difference between the mean APACHE II score of AKI patients and that of controls exceeds the maximum difference that could be caused by the renal component (serum creatinine level) of this score alone. As we have shown, corrected APACHE II scores without the renal aspect in the AKI group were still significantly higher than the controls. Alternatively, AKI might be the leading condition in some patients causing impairment of other organs, e.g. by promoting a systemic inflammatory response [9]. However, such a causality will be difficult to prove in multimorbid patients.
Improving prognostication would facilitate decision-making about further management of patients in ICU. Thus, this study was also aimed at identifying those characteristics in VOPs with AKI, which may predict non-survival at an early stage. These characteristics include pre-existing features of patients, such as demographics or chronic conditions, as well as clinical features of the acute condition. As expected, exposure to nephrotoxins or hypotensive episodes were found to be more prevalent in non-survivors. Importantly, the KDIGO stage of AKI or the peak creatinine level alone did not differ significantly between survivors vs. non-survivors of AKI in our study. However, previous investigations in younger patient populations in ICU [17] or in non-ICU settings [14,15] reported a significant association between these two parameters and survival. The negative findings in our study suggest that other conditions override the contribution of AKI on outcome in this particular age group and setting. CKD, for example, is known to attenuate the mortality difference between AKI stages [9].
A substantially negative or positive fluid balance in intensive care patients appears to be correlated with a lack of recovery from AKI that was associated with increased mortality [18,19]. One study by Zhang, et al. [19] even showed that an increase by only 1 litre over 72 hours was associated with an increase in mortality. In our study, the fluid balance during days 1-2 and 3-4 was significantly higher in non-survivors compared to survivors. Non-survivors had a greater than 2 liter positive fluid balance when compared to survivors. The positive fluid balance was due to increased fluids received and due to decreased fluid output. Importantly, the fluid balance during day 1 and 2 was found to have a similar value in predictive modelling as the APACHE II score. This further emphasizes the impact of AKI on mortality in VOPs.
This study is important as it focuses on the very elderly in the ICU. Despite overall Apache II score being high and the presence of AKI, 49% of these patients survived and many (63%) were discharged home in a good functional state. This finding was also reported by Druml, et al. that despite increased disease severity over the years, age is not an important determinant of survival in patients with AKI [21].
The importance of a preventing fluid overload was further highlighted in this study.
This study is limited by the fact that it is a single center, retrospective study in a dedicated medical ICU. A further limitation is relying on creatinine as a marker for disease progression in this age group where a baseline creatinine was not always available and where CKD was prevelant. Our initial criteria of a raised creatinine above 140 micromol/l may have missed some patients who are sarcopenic [21].
A multicenter prospective study should be performed in the medical and surgical ICUs to further evaluate the prognostic factors affecting the very elderly patients. A study using creatinine trajectory may also be warranted.
AKI in VOPs, who survived the first 24 hours of ICU admission, is associated with a significantly increased mortality in comparison to age- and gender-matched controls. The most important predictors of mortality include positive fluid balance and APACHE II. Despite AKI, 63% of the survivors were discharged home to return to their previous lives indicating preservation of their quality of life. This is an important consideration when allocating ICU beds to the aging population.
M.R, S.S and M.B wrote the manuscript and assisted in the statistical analyses / concept for the research.
T.L and I.S performed the statistical analyses and formatted the tables / figures.
J.M, I.S and T.L performed the data collection.
PVH reviewed the data / statistical analysis and assisted with the final manuscript.
- Mortality in very old patients (age ≥ 80 years) with AKI admitted to ICU is high in comparison to age-matched controls (49 to 16%)
- Good prediction of ICU mortality with 2 parameters - APACHE II and fluid balance (AUROC 0.76)
- Two-thirds of survivors were discharged home
None.