Star fruit (Averrhoa carambola) and Bilimbi fruit (Averrhoa bilimbi) are fruits under oxalidaceae and exhibits similar biochemical characteristics. There are several reports enumerating the harmful effects of these fruits in healthy persons leading to acute kidney injury and even chronic kidney disease requiring renal replacement therapy. There are occasional reports of neurotoxicity related to consumption of these fruits in patients with chronic kidney disease, especially those receiving maintenance dialysis. We report an interesting case of an elderly female on maintenance hemodialysis who had developed neurotoxicity after consuming these fruits and succumbed owing to intractable seizures.
Star fruit, Bilimbi, Dialysis, Status epilepticus
Star fruit and Bilimbi fruit are available as seasonal fruits (Figure 1). Several studies have analyzed the nephrotoxic and neurotoxic effects of the two components of these fruits: Oxalic acid and caramboxin respectively. Nephrotoxicity is due to oxalate crystal deposition resulting in acute oxalate nephropathy which can occur even in people with normal kidney function, but more commonly in those with renal dysfunction. Caramboxin, which is the neurotoxin present in these fruits, is excreted out by the kidneys without any deleterious effect, but in those with kidney disease this toxin accumulates and eventually enters the brain and results in neurotoxicity. These fruits are easily available and popular worldwide, hence it is important to impart awareness of the harmful effects of excessive consumption of these fruits on normal kidney function and potential lethal neurotoxicity in CKD patients. Here we describe an elderly CKD patient on maintenance hemodialysis (weekly three dialysis) who developed neurotoxicity in the form of refractory seizures resulted in death after consuming a couple of these fruits.
 Figure 1: Showing Star fruit (Averrhoa carambola) on left and Bilimbi fruit (Averrhoa bilimbi) on right.
View Figure 1
Figure 1: Showing Star fruit (Averrhoa carambola) on left and Bilimbi fruit (Averrhoa bilimbi) on right.
View Figure 1
An 82-year-old woman with end stage renal disease on regular thrice weekly maintenance hemodialysis, presented to the emergency room with complaints of acute onset of intractable hiccups, vomiting followed by altered sensorium. Attenders could not give any remarkable history except for ingestion of 3 to 4 star fruit and bilimbi fruit each from her kitchen garden on the previous day around 4 pm and became symptomatic from 8 am next day (admission day). She had other comorbidities like type 2 diabetes mellitus, hypertension, hypothyroidism. Her regular medication list consisted of antihypertensives like nebivelol, prazosin, clonidine, cilnidipine, antiplatelets, statins, thyroxine, calcium supplements and insulin.
On arrival she was afebrile, conscious but confused. Her neurological examination was normal except for altered sensorium. There was no meningeal irritation or focal deficits. Initially diagnosed as acute gastritis with possible uremic encephalopathy and decided to manage symptomatically. She was immediately taken for hemodialysis of 4 hour duration. Initial blood investigations were unremarkable, random blood sugar 145 mg/dl, C-reactive protein 1.2 mg/litre, calcium 11.6 mg/dl which on next day after stopping calcium supplements 9.6 mg/dl, sodium 128 mEq/L, potassium 4.9 mEq/L, blood urea 103 mg/dl, creatinine 7.3 mg/dl, ammonia 10 micromol/l, liver function test and complete blood count were within normal limits. Blood gas analysis revealed only mild metabolic acidosis with normal lactate level. Computed Tomography (CT) brain was normal except for age related changes. Despite dialysis, her Glasgo Coma Scale (GCS) worsened over few hours and was intubated to secure the airway. She remained a febrile but stuperous, hence Magnetic Resonance Imaging (MRI) brain was taken one day after admission. MRI was normal except for the chronic ischaemic changes and the neuro parenchymal atrophy of basal ganglia which is often found in end stage renal disease patients. Initial Electroencephalogram (EEG) taken one day after admission showed epileptiform discharges in bilateral posterior head region and she was started on intravenous antiepileptic.
On the second day, she developed focal motor seizure involving left upper limb with further worsening sensorium and vasomotor over activity in the form of uncontrolled hypertension. EEG at that time showed epileptiform discharges in the posterior scalp leads. She was added with intravenous fosphenytoin and lacosamide in addition to leviteracetam. Her inflammatory and infection markers at that time were reviewed and found to be normal. Her metabolic parameters were also within acceptable limits. CSF study was considered but deferred, since her relatives were not keen for it. At that point especially with the history of ingestion of these fruits and intractable seizures, the possibilities of neurotoxicity owing to those were considered. She was given three sessions of one volume plasma exchange in addition to alternate day hemodialysis for better clearance of toxins. But her seizure remained intractable, despite adding propofol, midazolam and ketamine. Further EEG monitoring showed bilateral fronto central and centro temporal spike and wave discharges along with periodic spikes from right fronto central region. We repeated MRI brain 4 days after admission, which showed "interval appearance" of gyriform T2/FLAIR hyperintense signals involving bilateral parietooccipital cortex (left > right), cingulate gyrus and left medial frontal and inferior temporal cortex demonstrating mild restricted diffusion (L > R) suggestive of star fruit neurotoxicity (Figure 2, Figure 3 and Figure 4). Despite aggressive intravenous antiepileptics and other supportive measures we could not control her seizures and she succumbed on the fourteenth day after admission.
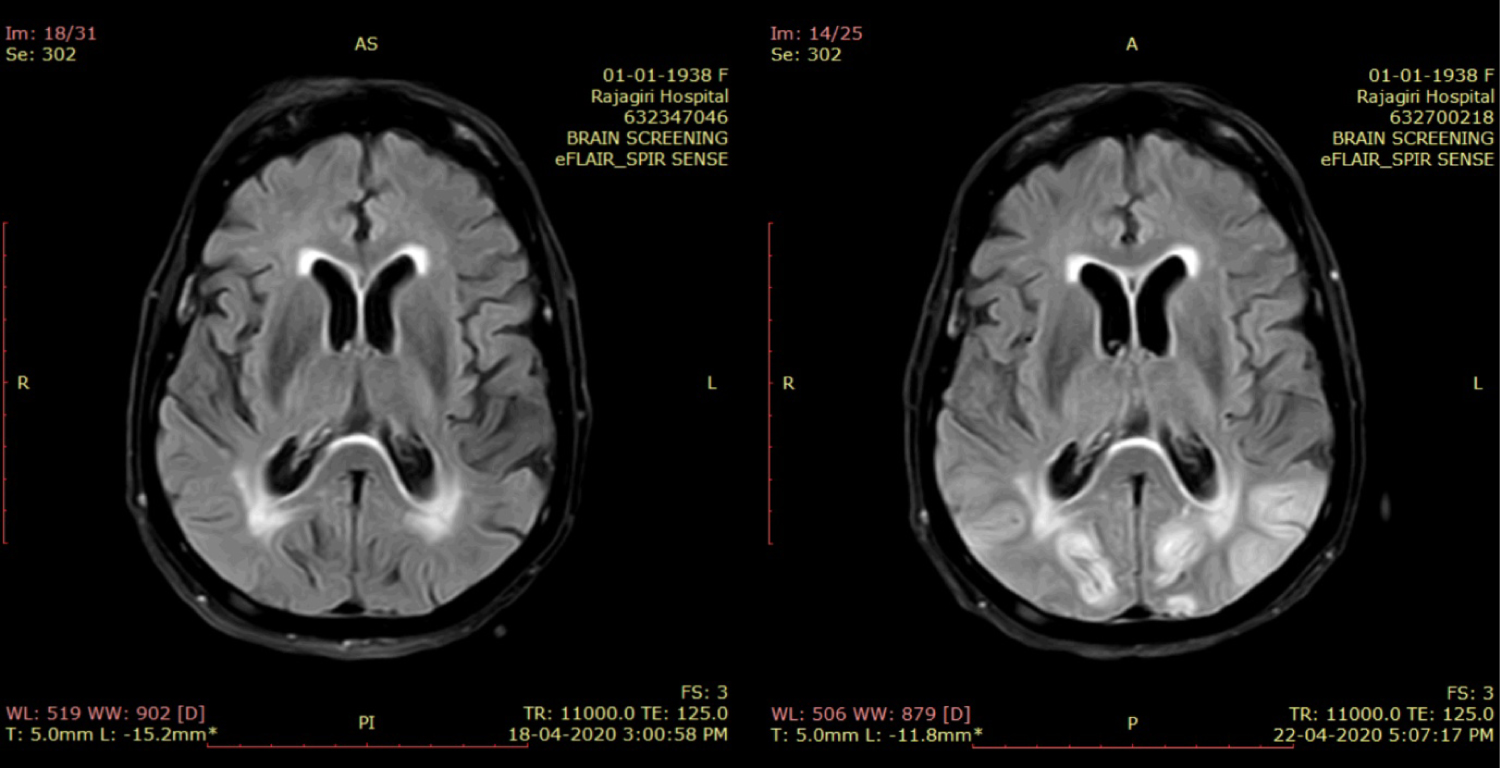 Figure 2: T2 FLAIR axial image taken at the level of the lateral ventricles shows asymmetrical hyperintensities involving the cortex of the bilateral occipital lobes as well as in the regions surrounding the occipital horns of the lateral ventricles in comparison with the first study on left.
View Figure 2
Figure 2: T2 FLAIR axial image taken at the level of the lateral ventricles shows asymmetrical hyperintensities involving the cortex of the bilateral occipital lobes as well as in the regions surrounding the occipital horns of the lateral ventricles in comparison with the first study on left.
View Figure 2
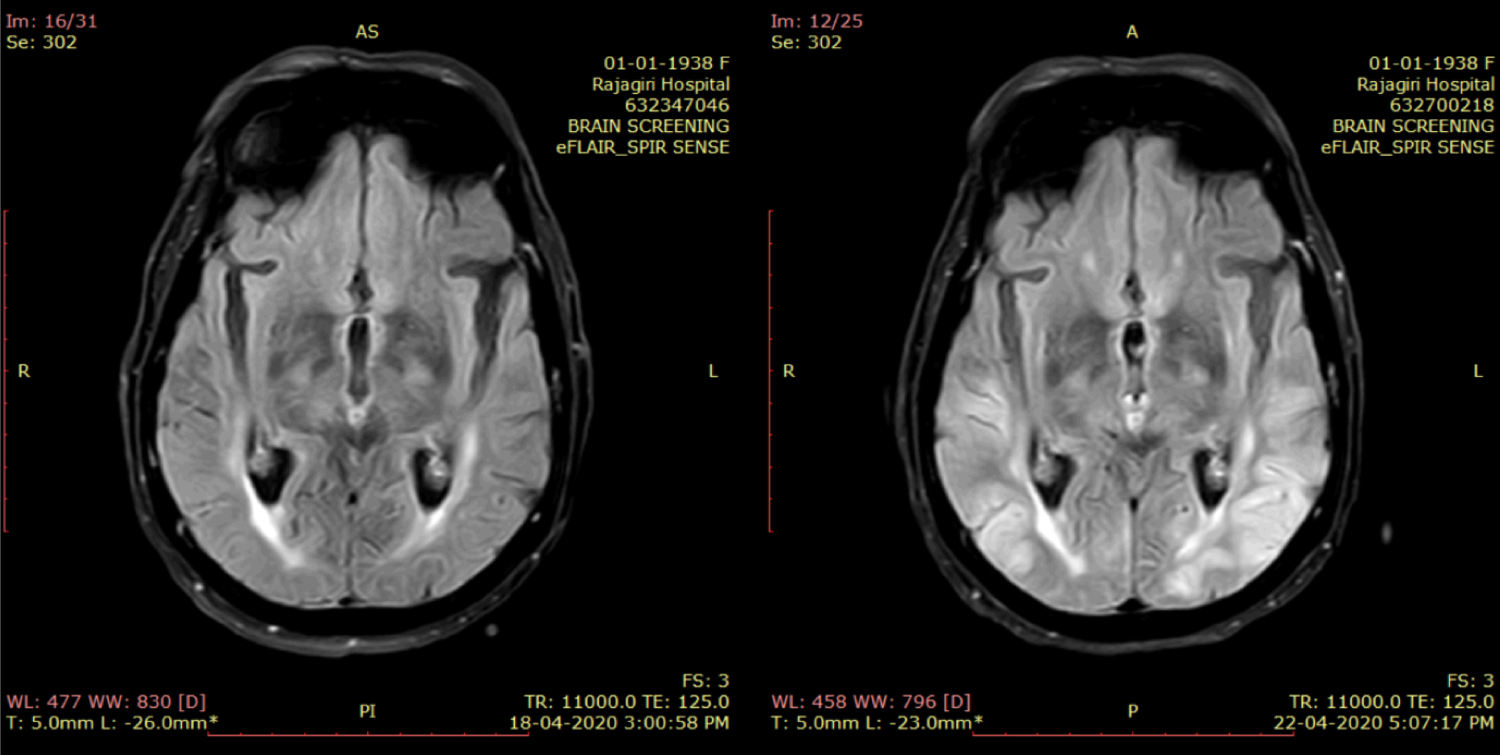 Figure 3: T2 FLAIR axial image taken at the level of the third ventricle shows asymmetrical hyperintensities involving the cortex of the bilateral occipital lobes as well as in the regions surrounding the trigones of the lateral ventricle in comparison with the first study on left.
View Figure 3
Figure 3: T2 FLAIR axial image taken at the level of the third ventricle shows asymmetrical hyperintensities involving the cortex of the bilateral occipital lobes as well as in the regions surrounding the trigones of the lateral ventricle in comparison with the first study on left.
View Figure 3
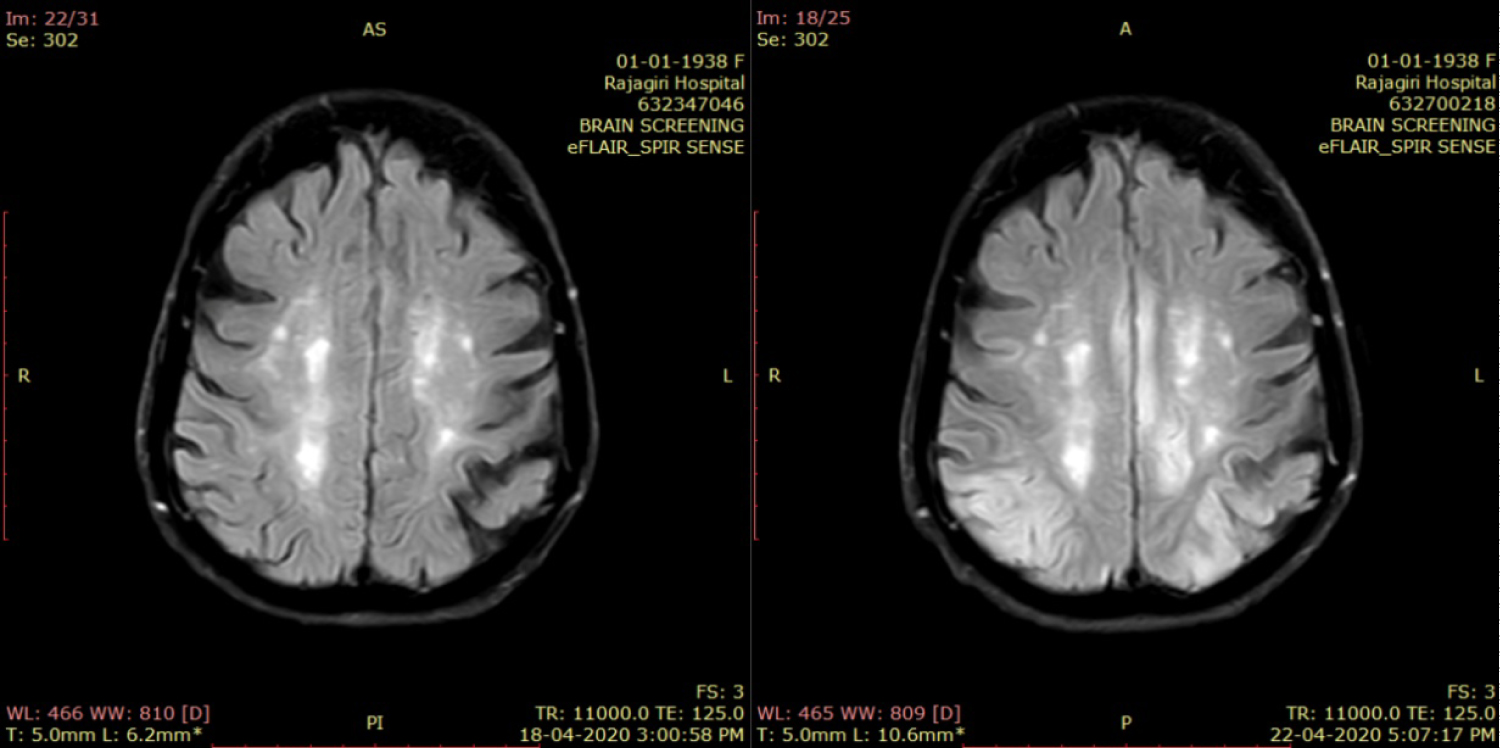 Figure 4: T2 FLAIR axial image taken at the level of the centrum semiovale shows asymmetrical hyperintensities in the bilateral centrum semiovale and he cortex of the posterior parietal lobes in comparison with the previous study on left.
View Figure 4
Figure 4: T2 FLAIR axial image taken at the level of the centrum semiovale shows asymmetrical hyperintensities in the bilateral centrum semiovale and he cortex of the posterior parietal lobes in comparison with the previous study on left.
View Figure 4
Averrhoa carambola is commonly known as star fruit. Although the tree is of Asian origin, it is now grown in different regions of the world. When cut in cross section it has star shaped appearance, giving its name as star fruit. This fruit is edible usually as raw or made it into pickle, juice, jams and wine.
Averrhoa bilimbi (commonly known as bilimbi fruit) has probable origin in Southeast Asia. It is cylindrical with five rounded longitudinal lobes, produced in clusters, and turning colour from green to yellowish green when ripe. Due to its extreme acidity and sourness unripe bilimbi fruit is usually used to make vinegar, pickles, and also as a substitute for lemon in seasoning. When ripe, the fruit can be consumed fresh or cooked in the form of compote or jam.
They belong to the family Oxalidaceae. They are popular medicinal fruits in the tropical region and used as natural remedies for various diseases. Its hypoglycaemic properties are considered useful in achieving glycaemic control in diabetes. It is also recommended as an expectorant, cough suppressant and also to control hypertension, hyperlipidemia, wound healing, and various rheumatic conditions as well as in cancers [1].
These fruits are both nephrotoxic and neurotoxic. The mechanism for renal toxicity could be the accumulation of calcium oxalate crystals owing to the high oxalate content in these fruits, which causes tubular obstruction and the subsequent apoptosis of renal tubular epithelial cells. This results in acute oxalate nephropathy and leads to acute kidney injury and often kidney replacement therapy [2].
Neurotoxic effects are due to caramboxin, which is a neurotoxin present in these fruits. Through various spectroscopic techniques, the scientists were able to determine the structure of caramboxin. The main structure of the neurotoxin resembles that of the amino acid phenylalanine. In contrast to the natural amino acid, the phenol ring of the toxin is also bound to extra ether, alcohol, and acid groups [3]. This nonproteinogenic amino acid, which has an agonist effect on NMDA glutamate receptors (AMPA and kainite receptors) and also specifically inhibit the GABAergic system. It acts as an excitatory neurotoxin and results in hyperexcitability in the brain resulting in the seizures [4].
The most common symptoms of neurotoxicity include persistent and intractable hiccups, vomiting, variable degrees of altered sensorium, psychiatric symptoms, decreased muscle power, paresthesia, paresis, insomnia, seizures and death. The mortality rate after star fruit intoxication ranges as high as 20-40%. Persistent altered sensorium is suggested as being associated with poor prognosis. Seizures are present in 30% of patients with star fruit intoxication, and most patients have convulsive or non-convulsive status epilepticus. The mortality rate of patients with seizures is significantly higher than of patients without seizures. Status epilepticus is associated with poor prognosis and an unpredictable as well as potentially fatal complication of intoxication of these fruits [5].
In Brazil, the first clinical description of the toxic effects of star fruit ingestion in CKD patients on hemodialysis was by Martin, et al. in Botucatu in 1993, who reported on 8-10 patients with intractable hiccups that improved with hemodialysis [6].
Our patient, an elderly lady on regular maintenance hemodialysis who had taken only 2-3 fruits of bilimbi fruit and star fruit each, presented to the emergency room in a symptomatic state within few hours after the consumption. The strong time relationship between the ingestion of these fruits and the onset of symptoms in our patient is strongly suggestive of caramboxin intoxication. Even though the neurotoxin was told to be dialysable, our patient did not respond to dialysis, plasma exchange and her seizure was refractory to all the anticonvulsants. Being an elderly lady with significant neuronal degeneration and the lack of renal clearance of this toxin owing to severe renal failure, the neurotoxicity of these fruits could have accentuated and she succumbed despite optimal care. Even though excessive consumption of fruits in dialysis patients commonly leads to hyperkalemia, our patient did not have that complication.
Neurologists and Nephrologists should consider the possibility of star fruit and Bilimbi fruit intoxication when patients with chronic kidney disease present with seizures or other unexplained neuropsychiatric symptoms. Since these fruits are widely available in tropical countries, healthcare workers should educate their CKD patients about this fatal complication.
Star fruit and Bilimbi fruit are widely available tropical fruits. It is vital to acquaint patients, physicians and other healthcare workers about the risks of its consumption. Patients with renal dysfunction, especially those undergoing hemodialysis are the target population. They need to be educated about the potential fatal neurotoxicity even with the consumption of a couple of these fruits and the importance of its avoidance. People with normal renal function should also be educated about its potential to cause acute kidney injury and chronic tubule interstitial disease.