This case report examines two rare mechanisms of acute renal failure in a patient with metastatic melanoma treated with high-dose vitamin C. The first is oxalate nephropathy, which is an uncommon but known complication of high-dose vitamin C therapy in naturopathic medicine. The second is due to melanuria and renal melanosis, which has been described in metastatic melanoma; however, acute renal failure requiring renal replacement therapy has not been reported previously.
Acute renal failure, Melanoma, Oxalate nephropathy, Vitamin C, Melanuria, Diffuse cutaneous melanosis
We report a patient with metastatic melanoma who presented to our hospital in acute anuric renal failure after receiving naturopathic treatments, including high-dose intravenous (IV) vitamin C infusions. A subsequent renal biopsy revealed both oxalate crystals and abundant melanin pigment reabsorption in the renal tubules, representing two rare mechanisms of acute renal failure.
A 54-year-old Caucasian man with a past medical history significant for metastatic malignant melanoma and a baseline serum creatinine (sCr) of 1.2 mg/dL presented to the Emergency Department in acute renal failure after outside laboratory studies demonstrated sCr of 11.4 mg/dL and serum potassium of 6.6 mmol/L. The patient was diagnosed with melanoma 10 months prior with metastatic disease to the liver and lymph nodes. He pursued naturopathic treatments, including high-dose vitamin C IV infusions (15 grams per dose). His last dose was administered 4 days prior to his presentation; however, the total number of infusions he received was unknown. Pertinent physical examination findings showed diffuse slate-gray discoloration of the skin and nails and marked hepatosplenomegaly with ascites (Figure 1).
 Figure 1: Slate gray discoloration of patient's nails, consistent with DCM.
View Figure 1
Figure 1: Slate gray discoloration of patient's nails, consistent with DCM.
View Figure 1
Laboratory studies performed in our Emergency Department revealed a sCr 9.52 mg/dL, blood urea nitrogen (BUN) 85 mg/dL, potassium 7.5 mmol/L, and phosphorus 9.1 mg/dL. Urinalysis revealed brown colored urine with specific gravity 1.018, trace leukocyte esterase, negative nitrite, grade 2 protein (protein/creatinine ratio 7.39), and pyuria. Urine culture was negative. Plasma oxalate was significantly elevated at 131.6 mcmol/L (normal < 1.6 mcmol/L). Electrocardiogram showed slightly prolonged QRS intervals. Computed tomography of the abdomen and pelvis without IV contrast revealed large areas of hypodense liver parenchyma with moderate ascites, predominantly left-sided retroperitoneal adenopathy, and no hydronephrosis. He received calcium gluconate, insulin with dextrose, and sodium bicarbonate for the acute management of hyperkalemia. The patient was admitted to the intensive care unit. A temporary dialysis catheter was placed for emergent hemodialysis in the setting of acute anuric renal failure and hyperkalemia.
A percutaneous ultrasound-guided left native renal needle core biopsy was performed. The biopsy cores were noted to have brown discoloration upon gross examination, with a dark brown speckling visible under the dissecting microscope (Figure 2). Light microscopy revealed unremarkable glomeruli. There was widespread severe tubular injury with associated oxalate casts and abundant melanin reabsorption pigment in the tubular epithelial cells and in association with the tubular calcium oxalate (Figure 3). The extensive intraluminal oxalate cast material was refractile under polarized light (Figure 4). No infiltrating cells of metastatic melanoma were identified; however, a von Kossa special stain highlighted abundant melanin pigment in association with the oxalate casts and reabsorbed within the tubular epithelium (Figure 5). Direct immunofluorescence with antibodies to IgA, IgG, IgM, C1q, C3, albumin, fibrinogen, kappa, and lambda was nonreactive. Electron microscopy studies revealed intact glomerular ultrastructure, with no evidence of immune complex deposits and intact podocyte foot processes.
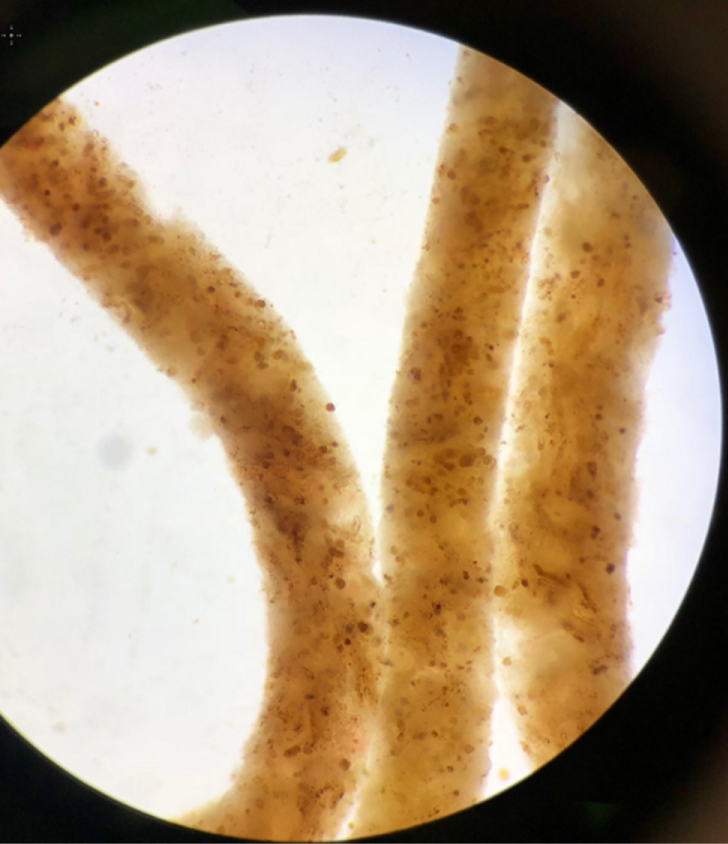 Figure 2: Dissecting microscope image showing diffuse brown discoloration of left native renal core biopsy.
View Figure 2
Figure 2: Dissecting microscope image showing diffuse brown discoloration of left native renal core biopsy.
View Figure 2
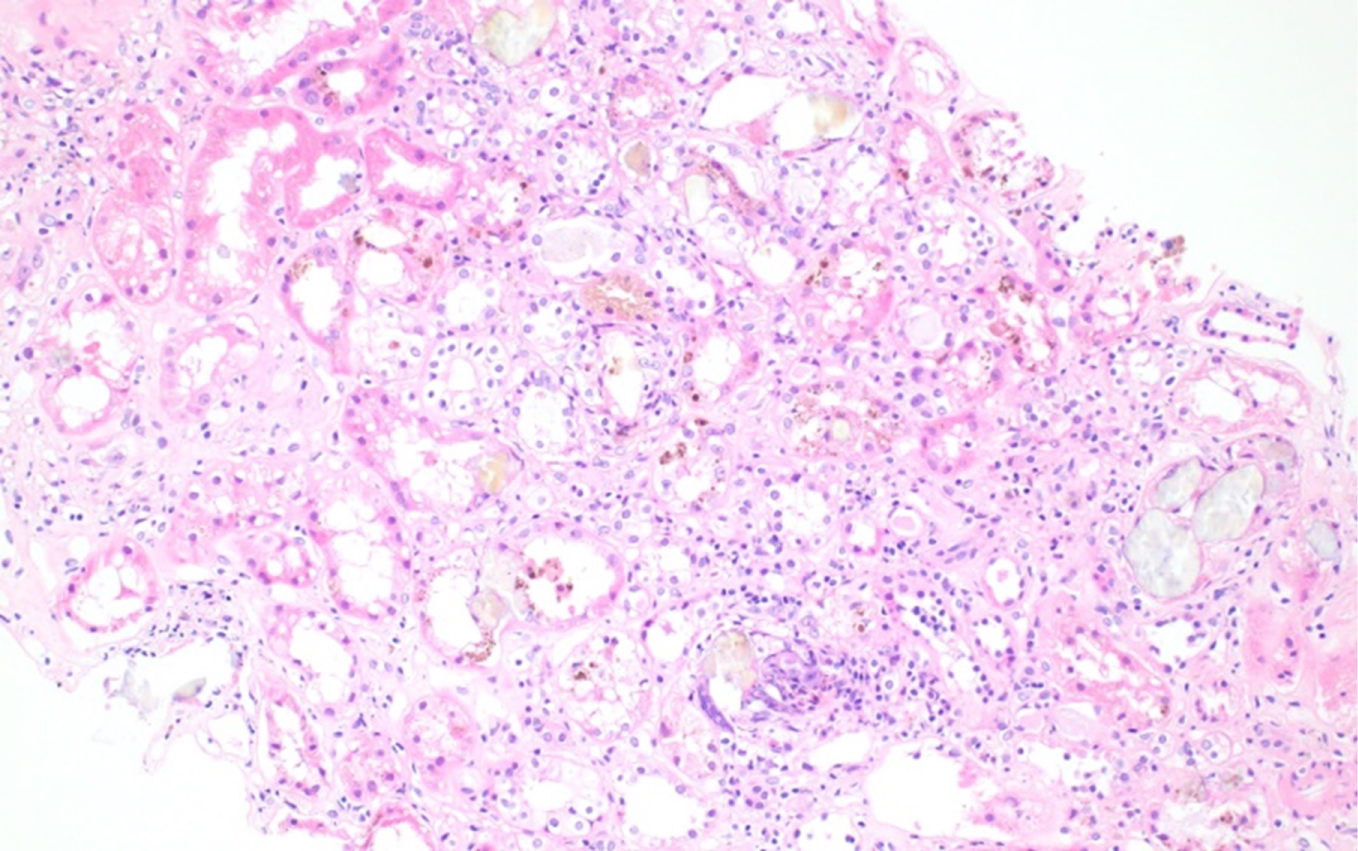 Figure 3: H&E stain with severe tubular injury and intraluminal cast material. 10x magnification.
View Figure 3
Figure 3: H&E stain with severe tubular injury and intraluminal cast material. 10x magnification.
View Figure 3
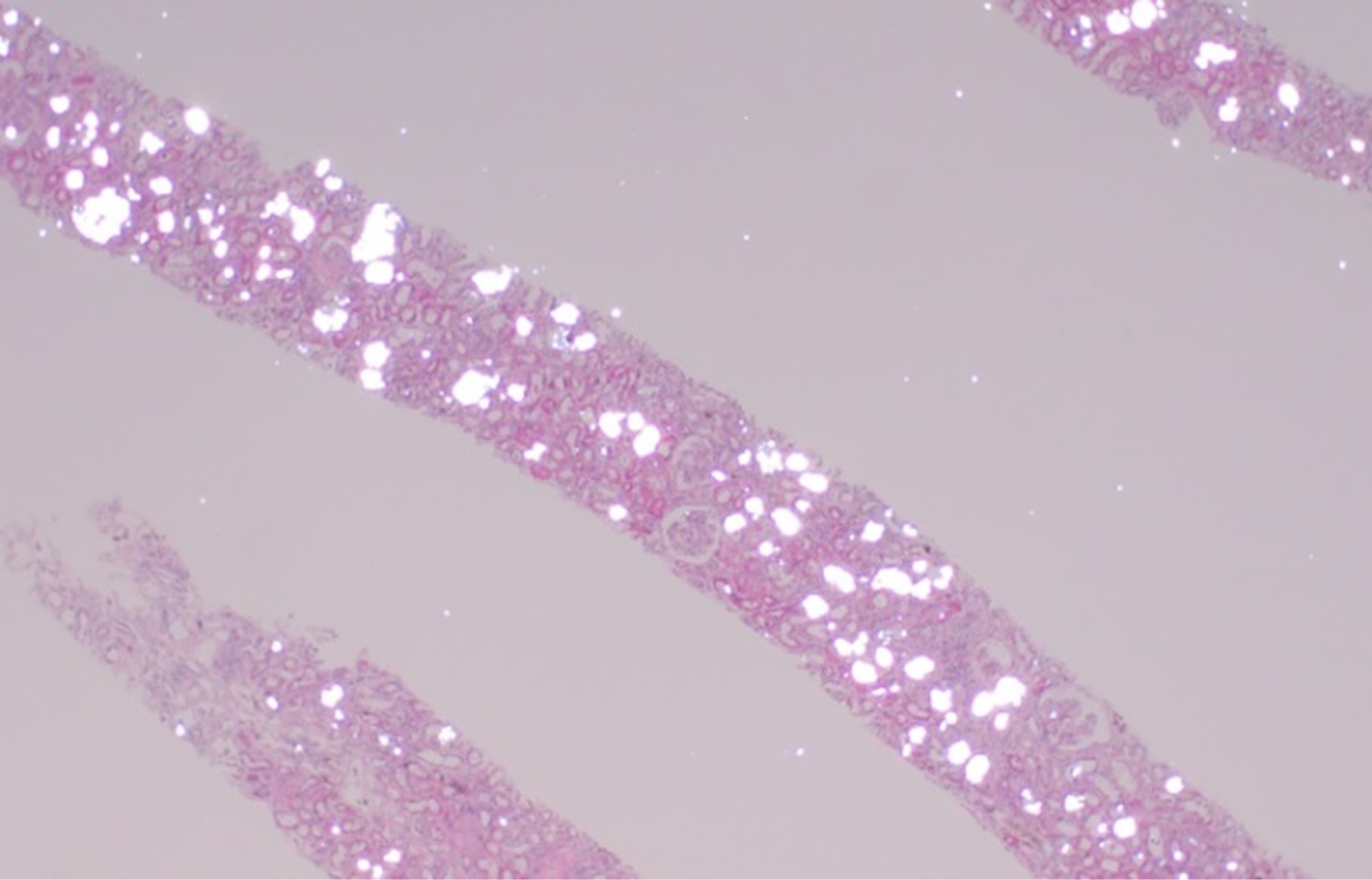 Figure 4: Numerous oxalate crystalline casts within the tubular lumens, which are refractile when viewed under polarized light. 4x magnification.
View Figure 4
Figure 4: Numerous oxalate crystalline casts within the tubular lumens, which are refractile when viewed under polarized light. 4x magnification.
View Figure 4
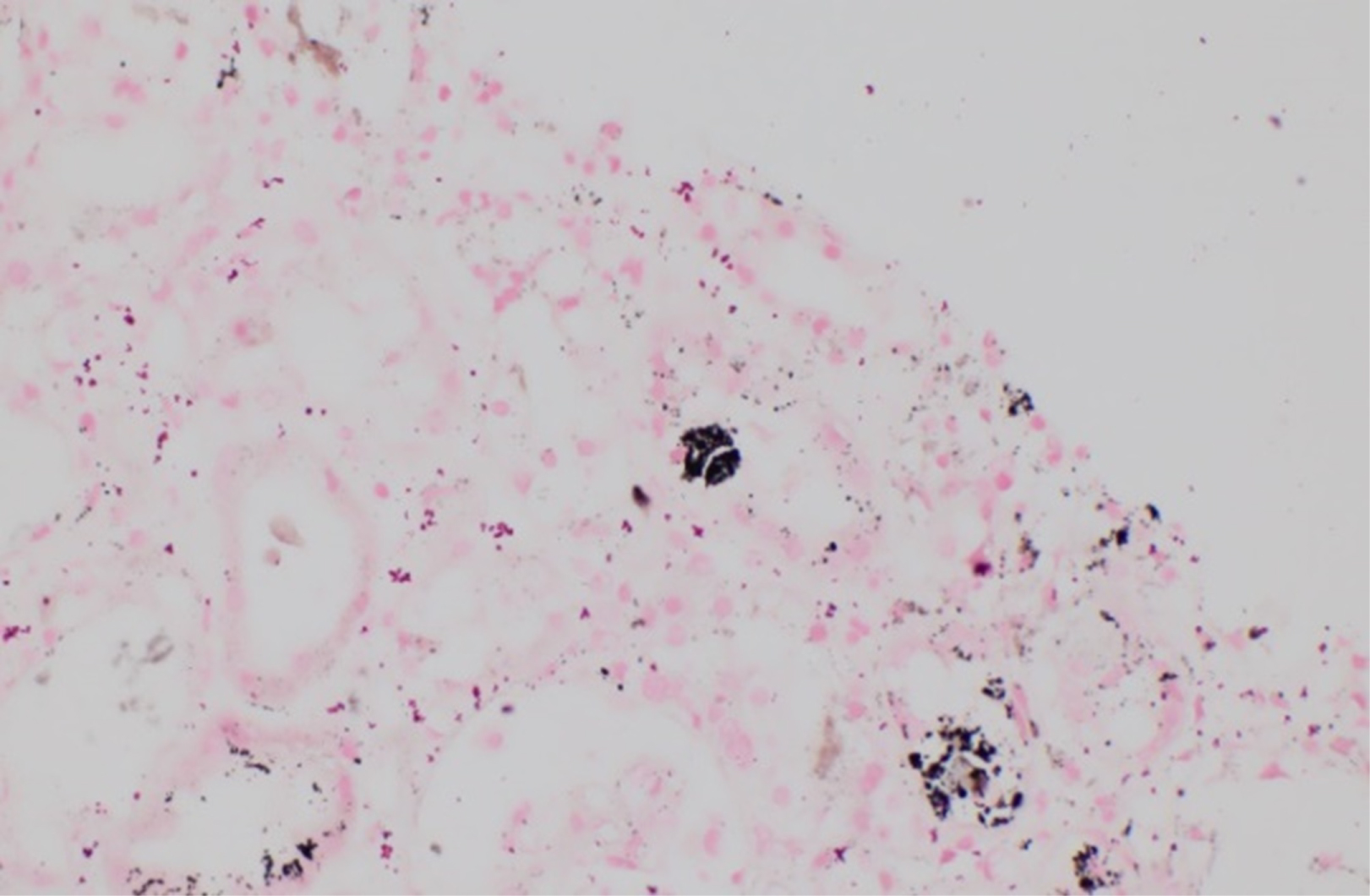 Figure 5: Fontana-Masson stain highlights abundant melanin pigment deposition in association with the tubular calcium oxalate. 40x magnification.
View Figure 5
Figure 5: Fontana-Masson stain highlights abundant melanin pigment deposition in association with the tubular calcium oxalate. 40x magnification.
View Figure 5
The patient remained anuric and continued to require intermittent hemodialysis. He was discharged home with Oncology clinic follow-up for initiation of immunotherapy. Unfortunately, the patient was readmitted a few days following discharge for recurrent malignant ascites. After an interdisciplinary 'goals of care' discussion, the patient was discharged to hospice and expired about one month later.
In summary, our patient presented in acute anuric renal failure after receiving high-dose vitamin C infusions for treatment of metastatic malignant melanoma. Renal biopsy revealed two rare, distinct potential mechanisms of acute renal failure- oxalate nephropathy and melanuria. However, it is difficult to discern the extent of each mechanism's contribution to the renal failure of our patient.
Oxalate nephropathy from high-dose vitamin C IV infusions is an uncommon but well-documented phenomenon [1,2]. High-dose vitamin C infusions are used by Complementary and Alternative Medicine providers as treatment for various diseases and malignancies [3,4]. Ascorbic acid, a water soluble vitamin, metabolizes to oxalate and the pathogenesis of oxalate nephropathy involves the formation of calcium oxalate crystals within the renal tubules and epithelium [1]. Oxalate production and excretion from ascorbic acid metabolism may also be dose-dependent, as one study showed higher total and supplemental intake of vitamin C was associated with increased calcium oxalate kidney stone formation in men [5]. Our patient had a significantly elevated plasma oxalate level (131.6 mcmol/L) and abundant oxalate crystal casts within the renal tubules consistent with oxalate nephropathy.
In addition, our patient with metastatic melanoma and the presence of melanuria had significant melanin deposition in the renal tubules, which may represent a second rare cause of kidney injury. Abundant brown pigmentation was visualized on histopathology using a Fontana-Masson stain for melanin (Figure 5). Melanuria, which can occur in about 15% of cases of metastatic melanoma, results from urinary excretion of phenol and indole metabolites of melanin precursors that undergo auto-oxidation to melanin in air [6]. Diffuse cutaneous melanosis (DCM), as evidenced by the patient's slate-gray discoloration of the skin and nails in our patient, is associated with a poor prognosis in metastatic melanoma. The exact pathogenesis of DCM is unknown, and the mean time to death is reported to be 4-5 months after the onset of DCM [7].
The role of melanuria in acute renal failure is unclear. To our knowledge, there has been only one case report of disseminated intra-tubular melanin deposition associated with acute kidney injury. Gambichler, et al. described a patient with metastatic malignant melanoma who presented with diffuse melanosis, melanuria, and acute kidney injury with sCr 1.9 mg/dL and BUN 84 mg/dL. Renal biopsy showed disseminated intra-tubular melanin deposits; however, this patient did not require hemodialysis [6]. Santos, et al. also reported a patient with metastatic melanoma to the liver and diffuse melanosis, who presented in renal failure with melanuria. However, the etiology of the acute kidney injury in this case was determined to be due to hepatorenal syndrome given the absence of proteinuria, no red or white cells in the urine, low urine sodium, and lack of improvement with volume expansion [8].
In contrast, prior case reports have described melanuria in the absence of renal failure. Eide published a case report of a patient with metastatic melanoma who presented with diffuse melanosis and melanuria with normal renal function [9]. Subsequently, autopsy revealed pigment emboli contained within the glomeruli varying from filling a single small capillary loop to involving the entire glomerular capillary tufts; melanin casts were also visualized in the renal tubules. Similarly, Saghari, et al. described a patient with metastatic melanoma and melanuria with normal renal function but in the absence of DCM [10]. Although it is difficult to determine the degree of kidney injury caused by melanuria, it can be theorized that significant melanuria and the direct tubulotoxic effect of melanin on the tubular epithelial cells may contribute to acute renal failure in patients with concomitant renal pathology, such as oxalate nephropathy in our patient.
Thus, this is the first case report to our knowledge that describes oxalate nephropathy and melanuria as two rare mechanisms of acute renal failure in a patient with metastatic melanoma treated with high-dose vitamin C.