Background: Menstruation is an important constituent of a female's reproductive health and wellbeing. With the ease of access to information on the web and modern culture and practiced norms, the biopsychosocial aspects of menstrual health are changing. The objective of this study is to know the level of awareness of menstrual health among university students based in Mauritius and identify aspects that could be addressed to promote menstrual health.
Methodology: A randomized sample of 658 students (507 females, 151 males) attending the University of Mauritius, representing all faculties, were recruited to partake in a standardized questionnaire. This questionnaire was made available on a circulated Google Form, which was suited to both female and male participants. Multiple choice questions and open-ended questions were used to allow biopsychosocial exploration. The data was then analyzed quantitatively using a statistical analysis.
Results: The study shows that the tertiary students of University of Mauritius only have superficial knowledge about the concept of menstrual health. Many of the participants are unaware about common menstrual disorders; polycystic ovary syndrome (PCOS), fibroids or endometriosis. Additionally, females fail to acknowledge the actual importance of their own menstrual health, especially regarding the possibilities of suffering from menstrual disorders or the necessity of regular medical check-ups.
Conclusion: Our study highlights the importance of reinforcing Menstrual Health Awareness in Mauritius. Breaking taboo, public awareness campaigns improving sex education curriculum, and implementing proper sanitary infrastructure will ameliorate menstrual health as well as help resolve the mental and physical troubles that women face.
Menstrual health, Menstrual hygiene, Period menstruation, Obstetrics & Gynecology, Women's Health
MHM: Menstrual Hygiene Management; WASH: Collective term for Water, Sanitation, and Hygiene; WHO: World Health Organisation; UNICEF: United Nations International Children's Emergency Fund; UoM: University of Mauritius
"Code red", "Aunt Flo" or "mo pe gagne malad madam [Translation: I am having female sickness]" are just some of the many colloquial terms used by females across the world to refer to their menstruation, with the latter being used specifically in Mauritius. Despite menstruation being a natural reality of life, experienced by 1.8 billion girls of reproductive age around the world, euphemisms are still used to refer to periods, insinuating a stigma is still attached to the words 'menstruation', 'period', and the topic as a whole [1,2].
Menstrual Health, as defined by UNICEF, is considered to encompass all aspects related to menstruation, including menstrual cycle, menstrual hygiene, menstrual disorders, in addition to other social aspects like general well-being, education and gender equality.
Menstrual hygiene management is a crucial part of menstrual health, which englobes: Choice of products, sanitation facilities and knowledge about hygiene. Choice and proper use of menstrual products in turn depends on factors such as financial status, cultural beliefs, accessibility and personal choice [3]. As emphasized by Sanjay Wijesekera, preceding UNICEF Chief of WASH (Water, Sanitation & Hygiene), "Meeting the hygiene needs of all adolescent girls is a fundamental issue of human rights, dignity, and public health" [4].
In marginalized areas around the world, schools do not have proper sanitation infrastructures, thus causing female students to miss school during periods or to wear menstrual products for a long period of time, increasing their risk of urogenital infections and cervical cancer [5-8].
The Mauritian population is also impacted by menstrual health. Around 50.5% of the population is female, of which 362,379 (~42.7%) are between 10 and 49-years-old, implying that a substantial number of the female Mauritian population are menstruating [9]. The consequences of poor menstrual hygiene management (MHM) are emphasized in a newspaper by a Mauritian gynecologist, "Pendant cette periode, on peut attraper facilement des infections urinaire, vaginale et pelvienne resultant en infertilite. Dans certains cas, cela pourrait être un choc toxique." [Translation: During this period, we can easily have urinary infections, vaginal and pelvic resulting in infertility. In some cases, it can lead to toxic shock] [10].
The increased prevalence of menstrual disorders clearly suggests that menstrual health should be considered as being an important public health concern. However, it was shown that only a third of the population experiencing severe or uncomfortable menstrual symptoms sought out medical advice [11]. Women may have misconceptions that what they are experiencing is normal, they take their health for granted and don't seek advice unless it is directly related to pregnancy or conception [12].
Period poverty is a significant barrier to menstrual health. Ranging from inadequate sanitation infrastructures to inaccessible and unaffordable menstrual products, it presents a great challenge to menstruating women. Where inaccessibility is not a problem, unaffordability is. Governments across the world impose a tariff on menstrual products that are taxed as 'luxury goods' rather than 'daily necessities (Pink Tax)', with only a few countries such as Canada, India, Kenya as well as Mauritius, offering tax free sanitary products [13].
Another significant obstacle to a proper MHM is the lack of or inappropriate knowledge on the subject [14]. Even if female members of the family discuss menstruation with the younger ones, they usually communicate their own misconceptions which are passed on along generations [15].
A Global School-based Student Health Survey report from 2011 displayed students who were sexually active, and among those in Mauritius: 46.9% had sexual intercourse for the first time below the age of fourteen. In relation to contraception, the number of adolescents who used a condom in their last sexual experience was only 44%. This increased the risk of sexually transmitted infections (STI's) and unwanted pregnancies [16].
Sexual education was integrated into the Mauritian curriculum only in January 2014 [17]. Nevertheless, in the CEDAW report of 2018, it was seen that a high rate of absenteeism in schools was attributable to taboo regarding menstruation, and also a lack of comprehensive sexual education contributed to a high rate of pregnancy among school age girls. Thus, indicating that there was no significant improvement in adequacy of sexual education between 2011 and 2018 in Mauritius [18].
To evaluate the awareness of menstrual health in university students studying in Mauritius, interviews were conducted on students of every age and faculty at University of Mauritius. An Ethical Clearance application was submitted and approved by an Ethical Committee present at University of Mauritius.
The type of study conducted was an internet-based quantitative analysis, through an online google form. The ideal minimum sample size, calculated using the Krejcie and Morgan Formula, was 620.
Two gender-oriented standardized questionnaires were devised through reference to previous questionnaires retrieved and adapted from other research projects. All scientific terms were written in layman terms with the scientific term or an explanation given in brackets to allow for easy comprehension. The questionnaire geared towards the female audience was more comprehensive of personalized questions regarding their own menstrual health, while the male questionnaire only assessed their general level of awareness. Multiple choice questions and open- ended questions were used to sufficiently allow a psychosocial exploration.
The questionnaire was formatted into a Google Form sheet, shared via the online university student email account (*studentname*@umail.uom.ac.mu) as a link with the assistance of the individual faculty representatives. Thus fulfilling the criteria of all the participants exclusively being from the University of Mauritius as well as ensuring randomization of participants therefore eliminating selection bias by the group members. Additionally, it facilitated easy accessibility for the participants and guaranteeing that all information remained confidential.
Data obtained were automatically summarized in the Google Form itself and also linked to a 'Microsoft Excel' sheet. Each of the original individual responses were recorded in a huge raw data table which included all of the questions and answers. This eliminated any error of manual data retrieval, however the questions and answers were vetted after retrieval to ensure they met the requirements prior to any analysis. All questions that were quantifiable were analyzed in a tabular form, and precise graphical analysis was done through bar and pie charts using the same software.
The project ensured complete anonymity and confidentiality through the questionnaire whereby no personal identification of any sort was recorded (e.g., name, student ID, date of birth). The group members were completely unaware of any specific person who participated and any identities of students.
A basic set of inclusion and exclusion criteria were created and upheld to modulate the sample population. The inclusion criteria clearly identify the target population in a subjective and unbiased manner (Table 1).
Table 1: Inclusion and exclusion criteria. View Table 1
Results are summarized in tables with an analysis.
Table 2 gives a brief overview on the demographics of the target population. The sample size was composed of 658 students, of whom 507 (77.1%) were females and 151 (22.9%) were males with ages ranging from 18-46 years-old (mean = 22.1-years-old: sd = 2.7). Most participants are undergraduate students (n = 567, 86.17%).
Table 2: Demographics of participants. View Table 2
From Table 3, 33 (6.5%) female participants describe menstruation as a painful time of the month while 22 (14.6%) male participants also describe it as a painful process. A total of 10 out of 507 females (2.0%) and 8 of 151 males (5.3%) are unaware that menstrual blood originates from the uterus.
Table 3: Answers provided by both Female and Male participants on knowledge about menstruation. View Table 3
Majority of the female participants (n = 293, 57.8%) learnt about menstruation from their family, while the majority of the males (n = 62, 41.1%) learnt about menstruation from school.
The most frequently used menstrual product by the female students is purchased sanitary napkins (n = 499, 98.4%). Toilet paper is the second most commonly used product (n = 65, 12.8%). However, 114 (75.5%) male students picked tampons as one of the frequently used menstrual products, whereas in actuality 7.1% (n = 36) female students use tampons.
Among the participants, 5.3% of females and 4.0% of males think it is not important for women to visit gynecologists regularly, while 117 students (23.0%) do not know if regular visits to doctor/gynecologist are important.
The most severely experienced symptom is cramping (rate = 5, n = 162). The least experienced symptom is urinary problems (rate 1, n = 354).
Table 4 shows 31.0% (157) of the females were unaware of menstruation prior to their first period, with 52.7% (n = 267) of female students not monitoring their fertility/menstrual cycle. Many of the female students had negative reactions to their first period (56.8%) specifically; scared (n = 209, 41.2%), embarrassed (n = 52, 10.3%), disgusted (n = 12, 2.4%), surprised (n = 8, 1.6%), sad (n = 4, 0.8%) and even confused (n = 8, 1.6%).
Table 4: Menstrual health. View Table 4
With regards to choosing menstrual products, 98.4% (n = 499) of the females consider comfort as the most important factor. The most commonly experienced adverse effects of menstrual products used are itching (n = 369, 72.8%) and rashes (n = 267, 52.7%) and only 11.4% (n = 58) do not experience side effects.
Even if 75.1% (n = 381) of the females think it is important to visit a gynecologist regularly, only 36.7% (n = 186) have ever been to a gynecologist. Among the female participants, 48.9% (n = 248) had concerns about their menstrual symptoms, and of that percentage only 6.5% (n = 16) expressed their concerns to someone.
The most commonly known disorders by the students are; Dysmenorrhea (painful period), Oligomenorrhea (infrequent periods), Amenorrhea (absence of a period), and Menorrhagia (heavy bleeding). While disorders such as Fibroids, Endometriosis, and PCOS are less known. However, results showed 11 (2.2%) females suffer from endometriosis and 31 (6.1%) from PCOS.
After carrying out the internet-based quantitative questionnaire, certain trends concerning the knowledge, practice, and management of menstrual health were identified. Majority of the target population have a superficial understanding of the topics explored though discrepancies were seen in many important aspects surrounding menstrual health.
Menstruation was perceived as a painful process rather than a normal natural process of the body by a few females (6.5%) and male participants (14.6%). This could reflect the personal experience of these menstruating females themselves in addition to their source of information about the subject.
As shown in Table 3, a minority of the students do not know that menstrual blood originates from the uterus. This further indicates the inappropriate knowledge they acquired about menstruation. For instance, if the female participants believe that both urine and menstrual blood come out through the same orifice (urethra), blood in urine, which could be serious, can be mistaken for menstrual blood and make them refrain from seeking medical attention.
Family was reported as the main source of information on menstruation by the female participants (57.8%). It could be implied that the concept of menstruation is mostly based on cultural beliefs and restrictions rather than obtaining the appropriate explanation about the process and its management. Considering the mean age of participants was 22-years-old, they did not benefit from Sex Education that was implemented into Mauritian curriculums in 2014.
As for the male participants, most of them learned about menstruation from their biology class as part of the school curriculum (41%) or by relying on the internet and friends to obtain information on the topic. Five male participants even pointed out that it was only through their significant other that they were acquainted with menstruation. Mauritian families either do not find it important to educate their sons about menstrual health or refrain from having this discussion due to the taboo associated.
Table 4 illustrates, 56.8% of all females experienced negative emotions during their first period. This negative reaction could partially be justified by the fact that over a quarter of female participants were ignorant about menstruation before menarche. 41.2% of females were scared when they got their first period, accounting for those who were uninformed and informed, meaning that the information they had may not have been suitable to prepare them for menarche. This further supports the idea of existing nuances in communication about menstruation leaving young females unprepared for such a significant physical and emotional transition in their life.
Around half of the female participants do not monitor their menstrual cycle. They might not recognize an irregularity in their cycle, or any other abnormal symptoms, which could potentially be due to a disorder that needs medical intervention. Besides the threat of menstrual disorders, early pregnancies can be detected, while surprise or unwanted pregnancies could be prevented by monitoring menstrual cycles.
While assessing the menstrual hygiene techniques of the female participants, it was observed that most of them adopt similar practices. As per Table 3, Sanitary napkins (98.4%) were found to be the most used products by females, and this was also supported by assumptions made by the 28.2% of males. Surprisingly, toilet paper (12.8%) was the second most commonly used product, possibly attributable to the cost of menstrual products or unexpected period owing to a lack of monitoring of the menstrual cycle. This may also be due to the absorbency of menstrual products used not being sufficient for their blood flow. Tampons (7.1%) are placed in an inferior position of use, likely because of its scarce supply in supermarkets in Mauritius, or again due to the taboo and misconceptions surrounding its use.
Table 4 illustrates that with regards to the choice of products, 98.4% of females chose comfort as the most important factor, while price (33.7%) and ease of disposability (31%) were reported as the second and third factors respectively.
In accordance with the above statements, safety (0.9%) was the least selected factor. This is quite alarming as some comfortable products can contain deodorants and other chemicals that are not always safe. Even though participants prioritized comfort over safety, it contrasted their reports on experiencing itching (72.8%) and rashes (52.7%) as the main side effects of their preferred menstrual products. Lack of knowledge on both the product and its effect could very well be the cause of participants being unable to distinguish that even though the product may be comfortable, it's not necessarily compatible with their body.
Figure 1 displays menstrual cramps rated as the most severely experienced symptoms by the female participants. Simply from what the participants ticked off, one symptom or even a combination of symptoms they experience might already be a precursor or the result of specific disorders. For instance, dysmenorrhea, the most commonly reported menstrual symptom, can be the effect of a number of menstrual disorders i.e; PCOS, endometriosis, or fibroids.
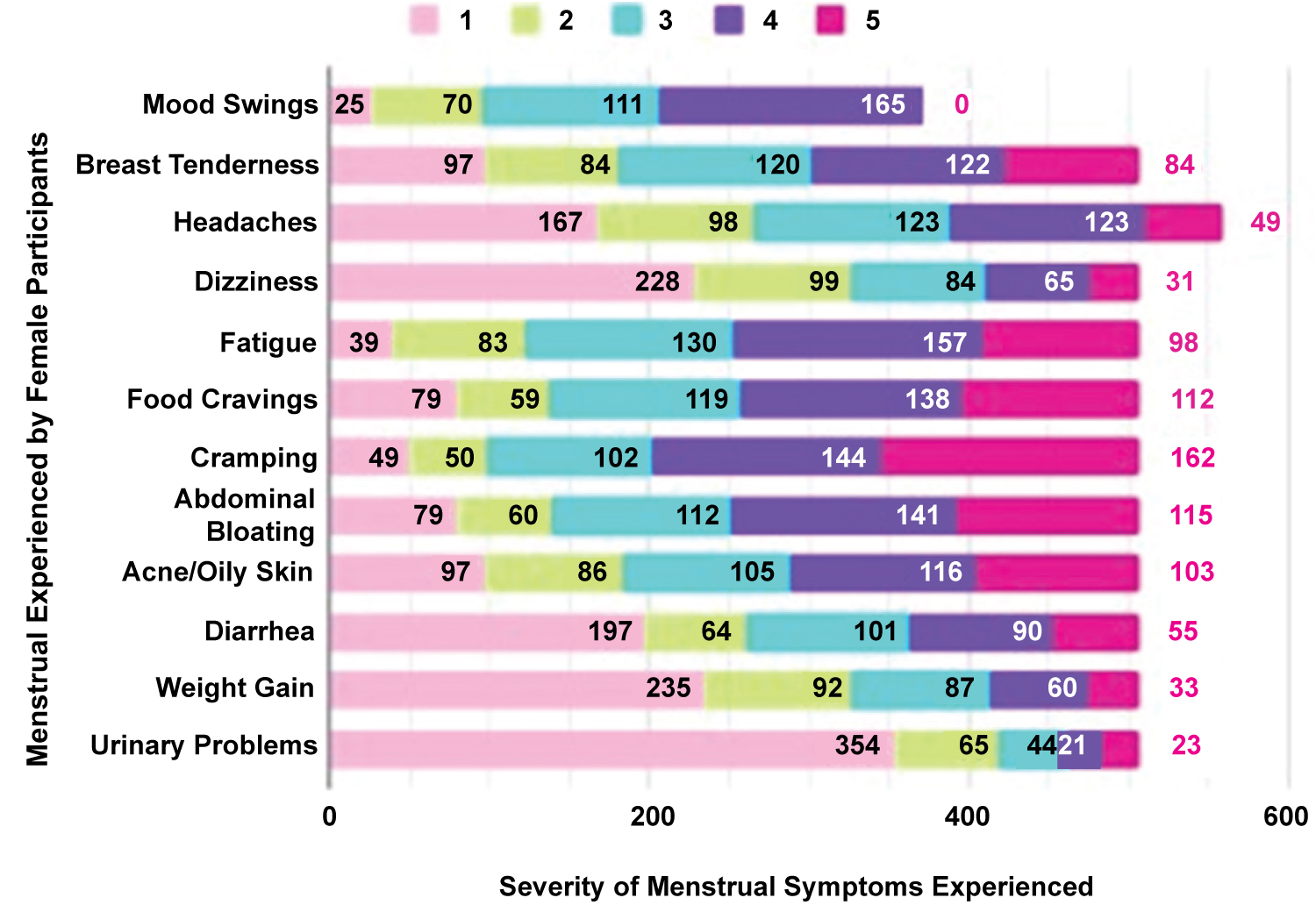 Figure 1: Severity of Menstrual Symptoms Experienced by female students The severity of menstrual symptoms experienced was assessed using a simple scale of 1 to 5. (1: Does not experience symptoms; 2: Tolerable experience; 3: Mild experience; 4: Moderate experience; 5: Severe experience).
View Figure 1
Figure 1: Severity of Menstrual Symptoms Experienced by female students The severity of menstrual symptoms experienced was assessed using a simple scale of 1 to 5. (1: Does not experience symptoms; 2: Tolerable experience; 3: Mild experience; 4: Moderate experience; 5: Severe experience).
View Figure 1
It was also found in Table 5 that a significant number of both female and male participants were unaware of menstrual disorders such as fibroids, endometriosis, and PCOS. Unfortunately, this is disquieting as these disorders are increasing in frequency and affecting women all around the world, including those that participated in this study. From the study population, 11 participants (2.2%) were diagnosed with endometriosis, while 31 participants (6.1%) suffered from PCOS.
Table 5: Female participants' awareness of menstrual disorders. View Table 5
With regards to regular check-ups to a gynecologist, 19.5% of female participants do not know if it is important to visit and 5.3% simply do not believe that it is important. This is further showcased by the fact that 63.3% of female participants have never been to a gynecologist. It was alarming to observe that even among the 48.9% participants who reported experiencing symptoms, and who claimed to be concerned, only 6.5% sought out help by either expressing their concerns to others or by consulting a gynecologist. This is a huge gap as the majority of the participants who had concerns did not express it to anyone. In essence, this could potentially mean more cases remaining undiagnosed or with delayed diagnoses, leading to complications later in life. Specifically with regards to fertility, people may be unaware for extended periods and may require major interventions to treat. There may even be cases where the damage is irreversible. Quality of life may be impacted which could have been prevented if further advice, investigations and treatment were initiated, as close monitoring and follow up could prevent progression of the disease in certain cases, eliminating major interventions.
After extensive exposure to the issues surrounding menstrual health, compiled with the views gathered from participants, a non-exhaustive list of recommendations has been formulated. The responses obtained from both male and female participants summed up four key ideas: breaking taboo, public awareness campaigns, improvement in education, and sanitary infrastructure.
The social, cultural, and educational environment in which a girl is nurtured greatly shapes their experience and knowledge about menstruation. Hence, some existing beliefs or myths perpetuate stigmas and taboo, which ostracize menstruating women and young girls from social, domestic, and educational activities. In order to improve the menstruation experiences of women across the world, a coordinated effort of policymakers, private sectors, and women's rights activists are required. In various parts of the world, organizations such as Flo Health's Charity Campaign, UNICEF, Women Strong International, and others are working to bring menstruation out of the shadows. In Mauritius, family members are on the front lines in educating their children about the topic, talks could be organized for parents at schools to provide them with the proper knowledge to support and educate their children. Another strategy to break the taboo is to provide a healthy platform where menstruating individuals can discuss sensitive topics with personnel equipped with the right training to provide emotional support.
Lack of education is one of the main factors which fuels myths and misconceptions, leading to taboo and restrictions while also being a big hindrance to proper Menstrual Health management.
Providing sex education at the appropriate age will help adolescents understand their body and provide them with the necessary information for safely and hygienically managing their menstruation.
Authorities should update their protocol about the age and the ways of delivering the information to the adolescents since the age of onset of menarche is much earlier for a significant number of females.
The opposite gender's role should not be neglected in the promotion of menstrual health as educating them will help normalize menstruation and allow them to understand, support, and respect their menstruating friends or family members. One strategy would be to use young males as leaders or teachers to help conduct gender-based workshops which would improve boys' perception of menstrual health while also implementing social and behavioral changes.
Given that nowadays we are all easily connected through media, propagating the message to improve menstrual health should not be a barrier. Public awareness campaign should be organized more often in universities, colleges, or shopping malls to not only break the taboo around menstruation but to equip women with the right knowledge to maintain good menstrual health. Gynecologists should be given the opportunity to have their say via radio, ads, or even in schools to educate the population on proper menstrual health management to prevent infections and disorders so that they understand the importance of seeking medical attention when needed.
Maintaining proper MHM is not only a woman's responsibility but requires a community- based approach involving schools, health centers, governmental and non-governmental organizations.
Women should be provided with the proper sanitation infrastructures in all public places consisting of WASH facilities, proper disposal facilities such as bins with lids or incinerators, and safely locked toilet doors. Menstrual products should be made available in vending machines in toilets at an affordable cost or free, as is being implemented in Scotland and Australia.
In Mauritius, more NGOs like the Ripple Project are required in order to bring light to solving period poverty as menstrual products are part of the basic needs of a woman, thus raising more funds will help those in need to manage their menstrual health safely and in a dignified manner. Training people in making safe reusable pads also reduces the environmental burden of sanitary napkin disposal.
The students of University of Mauritius are cognizant of the general concept of menstrual health. Nevertheless, multiple misconceptions remain. Females don't seem to acknowledge the importance of their own menstrual health, especially regarding the possibilities of suffering from menstrual disorders or the necessity of regular medical check-ups.
This study emphasizes that more steps should be taken toward reinforcing Menstrual Health Awareness in Mauritius. Breaking taboo, organising public awareness campaigns, improving sex education curriculum, and implementing proper sanitary infrastructure may, therefore, aid to ameliorate menstrual health as well as help resolve the multitude of mental and physical troubles that women face daily.
This study explored menstrual health in a psychosocial manner and was conducted through a self reported study where social desirability bias may have occurred. The participants were mainly young university students. Their level of awareness may differ from the general population which includes the elderly, uneducated people and others. The Google Form questionnaire could not guarantee participants filling out the form by themselves with no outside help or use of the internet. Menstrual experiences and knowledge are subjective thus it is difficult to use data obtained to make direct data comparison or summary statistical analysis by data aggregation. The study had to be adapted to the COVID-19 pandemic.
Considering the discrepancies in proportion of females and males, comparative analysis was challenging.
The authors are grateful to all the students who generously took the time to participate in the study. We deeply appreciate and thank Dr. Mahesh Rughooputh, our project supervisor, and Dr. Meera Manraj, our program coordinator, for their unconditional support and guidance. We also extend warm regards to our fellow classmates Mokshadha Shibnarain and Shehzad Yousouf Elaheebucus for their assistance and contribution.
All authors contributed equally to this manuscript.