Fleming cancer hypothesis, FMTVDM©℗, BEST imaging©℗, Breast cancer, Breast inflammation, Theranostics, Quantification, AI, Nuclear camera quantitative calibration, Patent protected, Secondary cancers
Prior to FMTVDM/BEST Imaging, diagnostic testing was limited to looking for breast cancer either using "qualitative" imaging defining disease as being present or absent, or semiquantitative methods [1-10] which are also limited to the same yes you have breast cancer or no you don't interpretation. These imaging methods include mammography, ultrasound, CT, MRI, as well as other SPECT/Planar and PET imaging approaches and as such are associated with sensitivity and specificity problems. These tests are further limited when imaging dense breast tissue or when breast implants exist either for augmentation or following mastectomy.
The ability of FMTVDM/BEST to differentiate transitional changes in tissue, associated with regional blood flow differences (RBFDs) and increasing tissue metabolism, makes it possible for FMTVDM/BEST to measure these tissue changes across an entire spectrum of changes; recognizing a "Health-Spectrum" shown by Figure 1. The interaction between cellular genetics and environmental factors consequently influence changes in tissue resulting in transitional changes including regional blood flow differences and metabolism. At one end of the spectrum is the absence of life, which may or may not be associated with a significant accumulation of cellular debris, inter alia, calcium, which may occur prior to the actual loss of cellular "life". In order of increasing regional blood flow and cellular metabolism are what is considered to be the "normal" state of a given tissue; resulting changes occurring due to an increased signaling and consequential accumulation of an inflammatory state; sequentially followed by further changes in tissue transitioning through increasingly metabolically active tissue with increased metabolic activity and demands for increased regional blood flow, until arriving at a tissue state where the expected controls and functionality of tissue no longer exist; what has classically been defined as "cancer". Implicit in this understanding is the appreciation that this continuum across transitional states reflects the interrelationship between these various "Health-Spectrum" states, which (1) Are not defined by some arbitrary absolute cutoffs b etween tissue states, (2) Demonstrate the ability of tissues to transition in either direction towards "normalization" or towards "cancer" and (3) Allow for the absolute measurement of the affect of treatment upon any of these tissue states across the "Health-Spectrum" providing the ability to direct care at the "patient-specific" level, improving outcomes across these transitional states; saving time, money and most importantly lives.
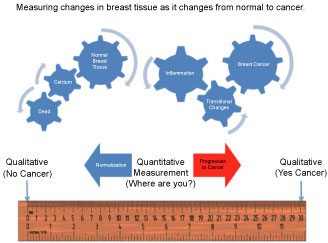 Figure 1: FMTVDM/BEST "Health-Spectrum" Measurements.
View Figure 1
Figure 1: FMTVDM/BEST "Health-Spectrum" Measurements.
View Figure 1
Because FMTVDM/BEST measures the RBFDs and metabolism of tissue and does not require tissue to compress for imaging and measurement, FMTVDM/BEST can be used to evaluate breast cancer in men as well as women.
A middle aged Caucasian woman who had previously been diagnosed with breast cancer was seen for FMTVDM/BEST evaluation and measurement. Her prior treatment had been discontinued secondary to side effects associated with chemotherapy.
Her initial BEST measurements (Figure 2) revealed an obvious cancer in her right breast with a BEST measurement of 402. The left breast had a BEST measurement of 250 associated with extreme inflammatory conditions and early cancer development. Due to limitations in the medical center she was initially seen at, there was some delay in treatment, and she was finally referred to another breast oncology center for surgical resection. Immediately before the surgery she underwent serial BEST imaging and measurement where the cancer in the right breast had grown with a BEST measurement of 447. The area within the left breast revealed the appearance of a more diffuse inflammatory process, which now measured 220. Twelve-months later a palpable mass appeared in the left breast, which revealed a BEST measurement of 373. The lump was biopsied revealing breast cancer. She deferred further treatment given her prior complications with chemotherapy.
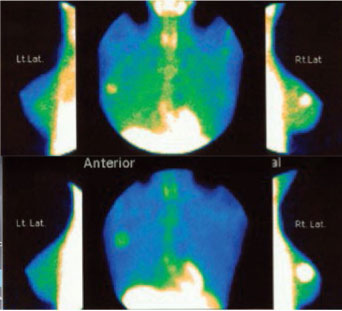 Figure 2: Unmasking Hidden Recurrent Cancers using FMTVDM/BEST.
View Figure 2
Figure 2: Unmasking Hidden Recurrent Cancers using FMTVDM/BEST.
View Figure 2
Serial FMTVDM/BEST Imaging and measurements revealed a cancer in the right breast. The top row of BEST imaging shows the initial results with an obvious breast cancer in the right breast with BEST measurement of 402. The left breast does not reveal an obvious tumor, although the BEST measurement was 250 seen with extremely "inflammatory" conditions and early cancer development. The second study performed nine months later showed an increasing tumor mass in the bottom panel in the right breast with a BEST measurement of 447. The left breast showed a reduction in BEST measurement values to 220 (Figure 2).
Considerable debate exists as to the underlying causes for recurrent breast cancers. Are they truly recurrent or do they represent new primary cancers. The ability to "quantify" changes in breast tissue using FMTVDM/BEST imaging not only offers us the unique capacity to monitor changes in tissue and treatment responses but it now provides an insight into that fundamental question.
The increased growth of cancers requires that the cells present in that tissue, to meet their increased metabolic demands, increase blood flow to themselves. This process of angiogenesis is the result of several angiogenic (stimulatory) compounds including inter alia miR-20a, CD34, and ATK3 kinase, which are released by the cells as they transition into cancerous tissue. It has been established that FMTVDM/BEST imaging and measurement, measures regional blood flow differences (RBFDs) and metabolism seen across the "spectrum" of tissue changes, which are a consequence of this angiogenesis.
All tissues/cells additionally release "inhibitory" compounds, which control the growth and metabolic function of cells, maintaining the tissues expected state of "normal" including inter alia growth rate, metabolism and vascularity. These inhibitors undoubtedly have greater effect upon less metabolically active tissue. As cancerous tissue grows, the ratio of stimulatory to inhibitor compounds increase, where the inhibitory compounds being released have their greatest effect upon other tissue with lesser quantities of stimulatory compounds.
The FMTVDM/BEST imaging measurements of this woman revealed inhibition (250 to 220) of the early cancerous tissue developing in the left breast, while the more angiogenic and metabolically active cancer (402 to 447) in the right breast continued to grow, influenced more by the stimulatory than inhibitory compounds being released by the cancer.
Once the primary or largest cancer was removed, the release of its inhibitory compounds ceased and the suppressed cancer in the left breast was free to grow uninhibited. Since she chose to receive no additional chemotherapy or radiation therapy given her concerns associated with prior consequences, there was nothing to inhibit the growth of the cancer in the left breast which made itself known 12-months later.
Not only does FMTVDM/BEST imaging demonstrate the transitional changes measurable by FMTVDM/BEST as well as the ability to measure treatment outcomes; it also provides evidence of the hypothesis that larger cancers through the release of the larger primary cancers inhibitory compounds inhibit smaller cancers.
The Fleming Cancer Hypothesis not only explains why secondary cancers may only be seen (qualitative) months to years after the primary cancers are removed; cancers which are not detected using the "qualitative" imaging tools of mammography, ultrasound, CT, MRI, etc.; but it also offers insight into new potential treatments for cancers - viz. the harvesting of inhibitory compounds from the removed primary cancers, which were clearly effective at self-treating the smaller secondary cancers, thereby depriving the smaller cancers of increased angiogenesis, while the larger primary cancers increase angiogenesis to meet their increased metabolic demands, necessary for the primary cancers own survival [11,12].