Related some recent example of human virus diffusion and epidemiology is interesting to observe some facts related latitude, climate, air pollutants and other. In this work only few images are used to submit and hypothesis of work to better understand some process. Is interesting to observe that WUHAN is a region characterized by a specific air pollutants status and near two big river in a determinate latitude. Obviously, the human transmission and the relationship with animal transmission can not to be forget. But there are other factor that can act to favor the viruses diffusion? Prof. GALLO in this days introduce the concept that is not sure a diffusion of this kind of virus in south of the world. (Since now a diffusion east-west), now about no diffusion of cases in Russia. In Italy diffusion in north and in some north region (now). There are relationship with climate condition? It is also interesting to observe what happen in Wuhan region (and also in other) in periods of COVID-19 diffusion related air pollution and the evolution of the diffusion of the disease.
This industrial area is a really polluted area and this fact must to be take in consideration in the recent event. The reducing of air pollution in Wuhan region after COVID-19 is clear as showed by figure presented in this work. It is due by the stop of many industrial activity and related the measure adopted by government. In the same time after all strictly measure adopted also another fact emerged: the reducing in air pollution. Other fact is that now the diffusion of the disease in china seem to reduce highly as seen in world media information.
It is an opinion of the authors that also the measure to reduce air poisoning must to be evaluated in this kind of pathology diffusion (HYPOTESYS).
COVID-19, Mers, Sars, Flu, Epidemiology, Climate, Latitude, Air pollutants, Geography, Aerosols, Orthomyxoviridae, Infections, Disease transmission, Relative humidity, Epidemics, Atmospheric circulation, Disease models, Environment, Climate change, Viruses, Environmental toxicology, Meteorological factors, Weather conditions
With a visual method (OBSERVATIONAL) some images and figures related diffusion of SARS, MERS, FLU and air pollutants are showed: Observing also the maps related some region involved in a day by day evolution.
HYPOTESYS to be tested: To verify air pollution effect on diffusion of some virus: Consequences or relationship? In order to do this it is interesting to observe air pollution in some region with high prevalence and incidence of COVID-19 and its reducing after measure of quarantine. That stopped industrial activity. A bibliographic work complete this related to the topic under investigation. Al article come from scientific database like PUBMED. After this work a global conclusion is produced to be submitted to the researcher.
From various on line resource: (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7) and related some relevant virus diffusion: Spanish flu 1918, Asian flu 1957, Avian flu 1997, Sars 2003, COVID-19 2019-2020.
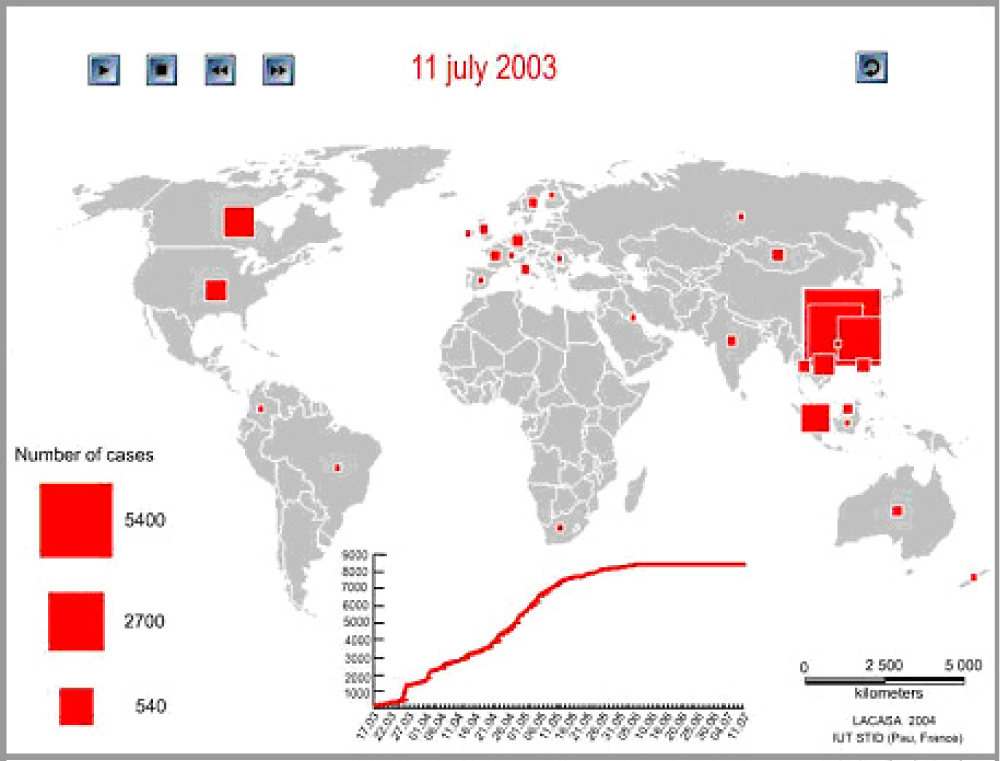 Figure 1: Sars epidemiology.
View Figure 1
Figure 1: Sars epidemiology.
View Figure 1
 Figure 2: Mers epidemiology 2015 july.
View Figure 2
Figure 2: Mers epidemiology 2015 july.
View Figure 2
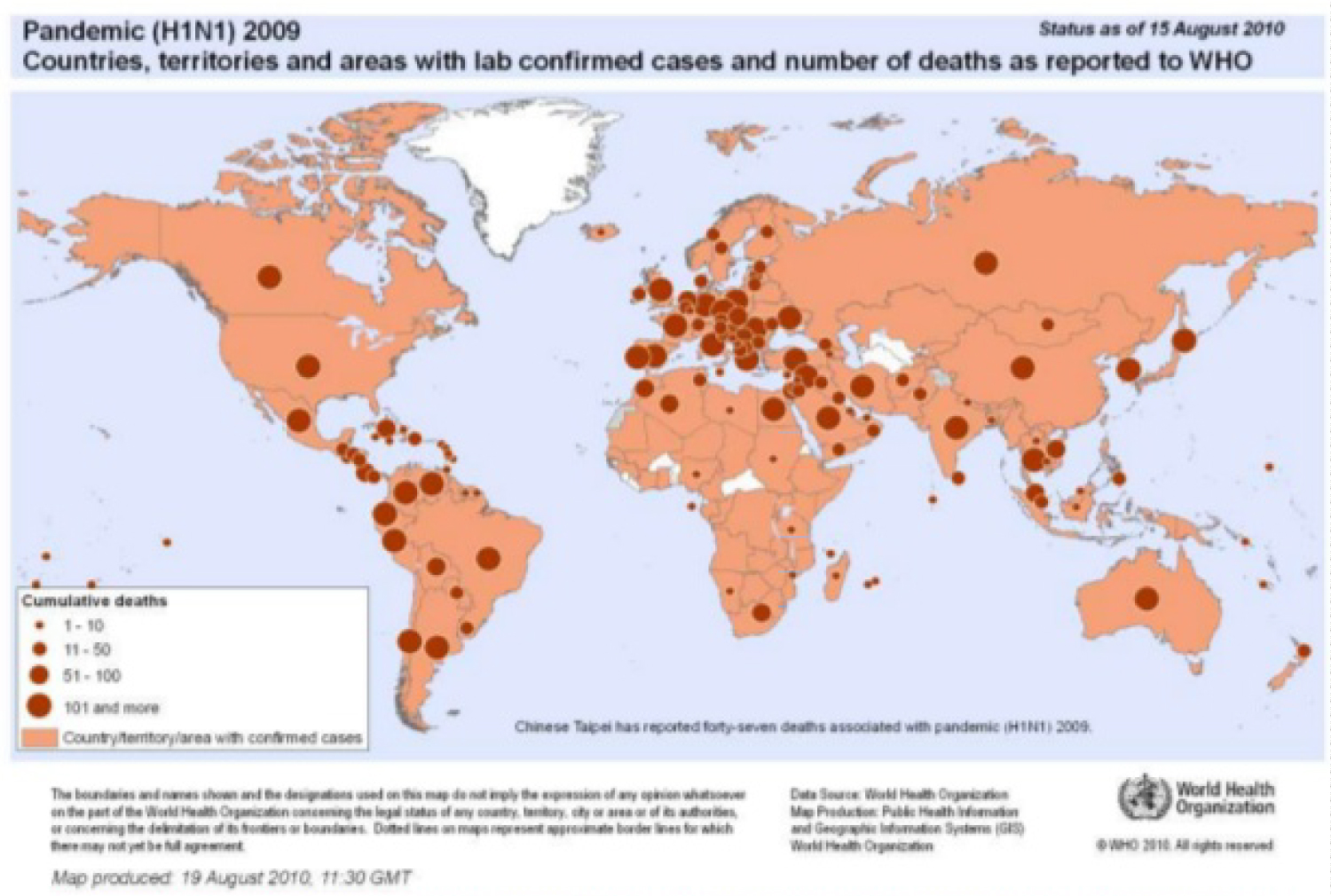 Figure 3: Pandemic (H1N1) 2009 countries, territories and areas with lab confirmed cases and number of deaths as reported to WHO.
View Figure 3
Figure 3: Pandemic (H1N1) 2009 countries, territories and areas with lab confirmed cases and number of deaths as reported to WHO.
View Figure 3
 Figure 4: Covid 19 Epidemiology.
View Figure 4
Figure 4: Covid 19 Epidemiology.
View Figure 4
 Figure 5: World air pollutants.
View Figure 5
Figure 5: World air pollutants.
View Figure 5
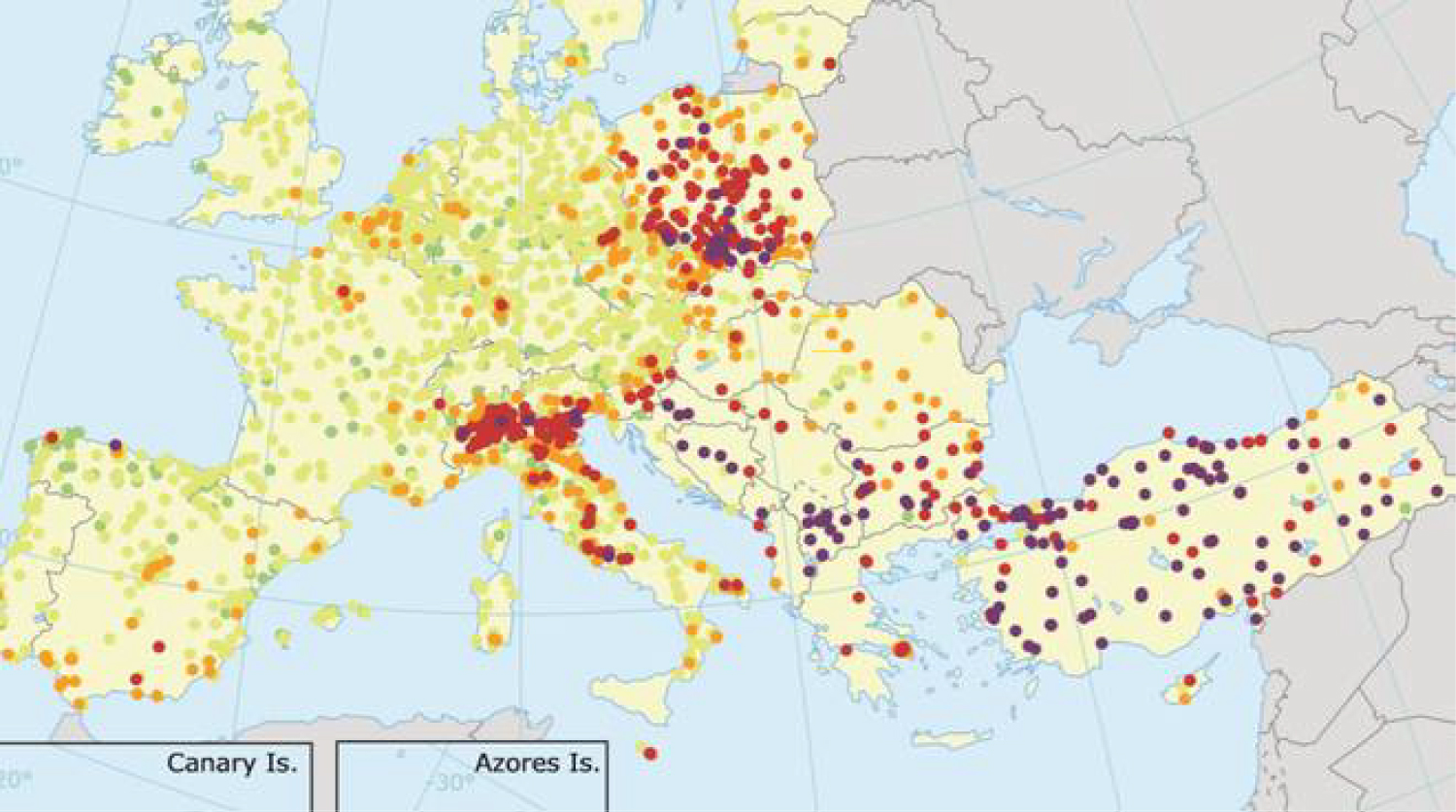 Figure 6: 2018 air pollutants Italy.
View Figure 6
Figure 6: 2018 air pollutants Italy.
View Figure 6
 Figure 7: Earth's increasing average surface temperature.
View Figure 7
Figure 7: Earth's increasing average surface temperature.
View Figure 7
According Wei Su, et al. [1]: "There is valid evidence that air pollution is associated with respiratory disease. However, few studies have quantified the short-term effects of six air pollutants on influenza-like illness (ILI). This work explores the potential-relationship between air pollutants and ILI in Jinan, China. Air pollutants, especially PM2.5, PM10, CO and SO2, can increase the risk of ILI in Jinan. The government should create regulatory policies to reduce the level of air pollutants and remind people to practice preventative/control measures to decrease the incidence of ILI on pollution days" [1].
Mao Wang, et al. [2]: "There is no evidence supporting that temperature changes COVID-19 transmission. We collected the cumulative number of confirmed cases of all cities and regions affected by COVID-19 in the world from January 20 to February 4, 2020, and calculated the daily means of the average, minimum and maximum- temperatures in January. Restricted cubic spline function and generalized linear mixture model were used to analyze the relationships. Results There were in total 24,232 confirmed cases in China and 26 overseas countries. In total, 16,480 cases (68.01%) were from Hubei Province. The lgN rose as the average temperature went up to a peak of 8.72 ℃ and then slowly declined. The apexes of the minimum temperature and the maximum temperature were 6.70 ℃ and 12.42 ℃ respectively. The curves shared similar shapes. Under the circumstance of lower -temperature, every 1 ℃ increase in average, minimum and maximum temperatures led to an increase of the cumulative- number of cases by 0.83, 0.82 and 0.83 respectively. In the single-factor model of the higher-temperature group, every 1 ℃ increase in the minimum temperature led to a decrease of the cumulative number of cases by 0.86. The study found that, to certain extent, temperature could significant change COVID-19 transmission, and there might be a best temperature for the viral- transmission, which may partly explain why it first broke out in Wuhan. It is suggested that countries and regions with a lower-temperature in the world adopt the strictest control measures to prevent future reversal" [3].
Lowen AC, et al. [4]: "Using the guinea-pig as a model host, we show that aerosol spread of influenza virus is dependent upon both ambient relative humidity and temperature. Twenty experiments performed at relative humidities from 20% to 80% and 5 ℃, 20 ℃, or 30 ℃ indicated that both cold and dry conditions favor transmission. The relationship between transmission via-aerosols and relative humidity at 20 ℃ is similar to that previously reported for the stability of influenza viruses (except at high relative humidity, 80%), implying that the effects of humidity act largely at the level of the virus particle. For infected guinea pigs housed at 5 ℃, the duration of peak shedding was approximately 40 h longer than that of animals housed at 20 ℃; this increased shedding likely accounts for the enhanced transmission seen at 5 ℃. To investigate the mechanism permitting prolonged viral growth, expression levels in the upper-respiratory tract of several innate immune mediators were determined. Innate responses proved to be comparable between the animals housed at 5 ℃ and 20 ℃, suggesting that cold temperature (5 ℃) does not impair the innate immune response in this system. Although the seasonal epidemiology of influenza is well characterized, the underlying reasons for predominant wintertime spread are not clear. We provide direct, experimental evidence to support the role of weather conditions in the dynamics of influenza and thereby address a long-standing question fundamental to the understanding of influenza- epidemiology and evolution" [5].
According A Tuck: Is it a coincidence that new viruses appear in highly polluted Chinese cities? Or in other industrialized region of the world? (North Italy?). The concentrations and relative abundances of OH, HO2, NOx and ozone are different there than elsewhere. Of course, the human population is denser too, but given that surface and interior chemistry happens in and on aerosols, is there a research problem here? COVID-19 is an airborne-transmitted pathogen? It was pointed out two decades ago in a prebiotic context that OH and HO2 would be agents of natural selection.
In article: The Role of Atmospheric Aerosols in the Origin of Life, Adrian Tuck and Surveys in Geophysics 2002:
"Recent results from the real time analysis of individual aerosol particles by laser mass-spectrometry have revived interest in the inverted micelle structure for aerosols containing organic molecules; indeed for many aerosols the organic content is high enough, for example ∼50% by mass in the tropical upper troposphere, that it is likely to be the only viable structure. It is pointed out that atmospheric -aerosols would have had many advantages as prebiotic chemical reactors, having the potential to address several key problems in a way arising naturally from the probable geophysical and chemical- environment on the prebiotic planet. Bacterial and viral size can be predicted for these structures by an equation combining atmospheric aero-dynamics and gravity, and which is therefore applicable to other astronomical -objects which are candidates for supporting life. Experimental tests and mathematical modelling of the early stages of the chemical evolution of aerosols should be possible" [6].
Natural selection can occur outside the human body as well as inside it. And in publication: Gibbs free energy and reaction rate acceleration in and on micro-droplets Adrian F Tuck, Physics Department, Imperial College London
Entropy 2019: "Recent observations show that many reactions are accelerated in micro-droplets compared to bulk liquid and gas media. This acceleration has been shown to feature Gibbs free- energy changes, ΔG, that are negative and so reaction enabling, compared to the reaction in bulk fluid when it is positive and so reaction blocking. Here, we argue how these ΔG changes are relatable to the crowding enforced by micro-droplets and to scale invariance. It is argued that turbulent -flow is present in micro-droplets, which span meso/macro-scales. That enables scale invariant methods to arrive at chemical potentials for the substances involved. ΔG and ΔG can be computed from the difference between the whole micro-droplet and the bulk medium, and also for individual chemical species in both cases, including separately the micro-droplet's surface film and interior, provided sufficiently fine resolution is available in the observations. Such results can be compared with results computed by quantum statistical mechanics using molecular-spectroscopic data. This proposed research strategy therefore offers a path to test its validity in comparing traditional equilibrium quantum statistical thermo-dynamic tests of micro-droplets with those based on scale invariant analysis of both their 2D surface and 3D interior fluid flows" [7].
Adrian F Tuck: "There is no widely agreed definition of entropy, and consequently Gibbs energy, in open systems far from equilibrium. One recent approach has sought to formulate an entropy and Gibbs energy based on observed scale invariances in geo-physical variables, particularly in atmospheric quantities, including the molecules constituting stratospheric chemistry. The Hamiltonian flux-dynamics of energy in macroscopic open non-equilibrium systems maps to energy in equilibrium statistical thermo-dynamics, and corresponding equivalences of scale invariant -variables with other relevant statistical-mechanical variables such as entropy, Gibbs energy, and 1/(kBoltzmannT), are not just formally analogous but are also mappings. Three proof-of-concept representative examples from available adequate stratospheric chemistry observations-temperature, wind speed and ozone-are calculated, with the aim of applying these mappings and equivalences. Potential-applications of the approach to scale invariant observations from the literature, involving scales from molecular through laboratory to astronomical, are considered. Theoretical support for the approach from the literature is discussed" [8].
And F Tuck: "This review article attempts to interpret the generalized-scale invariance observed in common atmospheric variables-wind, temperature, humidity, ozone and some trace species-in terms of the computed emergence of ring currents (vortices) in simulations of populations of Maxwellian molecules subject to an anisotropy in the form of a flux. The data are taken from ‘horizontal' tracks of research aircraft and from ‘vertical' trajectories of research drops ondes. It is argued that any attempt to represent the energy distribution in the atmosphere quantitatively must have a proper basis in molecular physics, a prerequisite to accommodate the observed long‐tailed velocity probability distributions and the implied effects on radiative -transfer, atmospheric chemistry, turbulent -structure and the definition of temperature itself. The relationship between fluctuations and dissipation is discussed in a framework of non‐equilibrium statistical- mechanics, and a link between maximization of entropy production and scale invariance is hypothesized" [9].
Other References to the generation of viruses and bacteria in parallel in reference (62 of the J Phys Chem A paper, D J Donaldson, et al. Spontaneous Fission of Atmospheric Aerosol Particles, Phys Chem Chem Phys., 3, 5270-5273 (2001).
According A Robichaud: It is possible there is a link since it has been shown that viruses can stick on diesel particles and exacerbate inflammatory response: Article Acute diesel exhaust particle exposure increases viral titre:
EPA Home » Science Inventory » DIESEL EXHAUST PARTICLES ENHANCE INFLUENZA VIRUS INFECTIVITY BY INCREASING VIRUS ATTACHMENT National Health and Environmental Effects Research Laboratory https://cfpub.epa.gov/si/si_public_record_Report.cfm?Lab=NHEERL&dirEntryId=115026&CFID=42012847&CFTOKEN=11134016 JASPERS, et al. Presented at American Thoracic Society Meeting, San Diego, 2005.
"Despite vaccination and antiviral therapies, influenza infections continue to cause large scale morbidity and mortality every year. Several- factors, such as age and nutritional status can affect the incidence and severity of influenza infections. Exposure to air pollutants, such as diesel exhaust (DE), can also affect respiratory virus infections. Previous studies have demonstrated that chronic DE-exposures enhanced influenza virus -replication in mice by decreasing interferon-dependent antiviral defense responses. However, it is not known how acute exposures affect influenza -infections. In this work we exposed differentiated human- nasal and bronchial epithelial cells, as well as A549 cells, to DE particles (DEP) for 2 hours and subsequently infected the cells with influenza A/Bangkok/1/79. Exposure to DEP enhanced influenza virus replication, as assessed by influenza hem-agglutinin (HA) RNA levels, viral protein levels, and the number of influenza-infected cells. This response was not caused by suppressed IFNb levels or IFN-dependent antiviral- mediator production, since influenza-induced mRNA levels for IFNb and MxA, an IFN-inducible antiviral mediator, were also enhanced by exposure to DEP. exposure to DEP increased influenza virus attachment within 2 hours post-infection. Exposure to DEP enhanced markers of oxidative- stress and addition of glutathione ethyl-ester (GSH-ET), reversed the effects of DEP on influenza virus replication and number of infected cells. These data suggest that oxidative -stress induced by DEP creates and cellular environment which favors influenza virus attachment and uptake. Taken together, the results presented here indicate that exposure to DE can have significant impact on influenza infections in human respiratory epithelial- cells" [10].
GW Hammond, et al.: "Current -theories of influenza viral- epidemiology have not explained the persistence, seasonality, and explosive outbreaks of virus over large geographic areas. It is postulated in this paper that atmospheric -dispersion and intercontinental scale transport of airborne- aerosolized influenza virus may contribute to the spread, persistence, and ubiquity of the disease, the explosiveness of epidemics, and the prompt region-wide occurrence of outbreaks and that seasonal- changes in circulation patterns and the dispersive character of the atmosphere may help to explain the regular annual cycle of influenza -activity" [11].
Current theories of influenza viral epidemiology have not explained the persistence, seasonality, and explosive outbreaks of virus over large geographic areas. It is postulated in this paper that atmospheric dispersion and intercontinental scale transport of airborne -aerosolized influenza virus may contribute to the spread, persistence, and ubiquity of the disease, the explosiveness of epidemics, and the prompt region-wide occurrence of outbreaks and that seasonal changes in circulation patterns and the dispersive character of the atmosphere may help to explain the regular annual cycle of influenza-activity. The current epidemiologic-concept of influenza viral infections parallels the measles model, in which it is believed that infections are spread by direct serial transmission from person to person, principally by the micro-scale dispersion of viral aerosols. While we recognize that direct serial person-to-person spread is likely the usual mode of transmission of influenza- virus, this theory does not adequately explain either the persistence of the virus as a human -pathogen or the seasonality of outbreaks. It also fails to account for other influenza characteristics, such as ubiquity, explosive out-breaks, the prompt region-wide occurrence of epidemics, and the relatively constant pattern of influenza epidemics over several centuries Long-range airborne spread of viral infection. Epidemiologic investigations have confirmed that the virus that causes foot-and-mouth disease has been transported by the atmosphere across the Baltic -Sea and across the English Channel. These regional -results, along with demonstrated micro-scale dispersion of certain viruses, suggest that, like air pollution, the airborne spread of pathogens may be a problem that extends from the local to the intercontinental scale. Infectivity of low-concentration viral- aerosols. Although greatly influenced by the amount of secretion in the nasal passages, a single cough or sneeze can produce accumulation-mode-sized particles that can remain airborne for extended periods. It follows that an infected populace in a region. Of the Far East could constitute a significant source of viral-aerosols. Long-range transport accompanied by atmospheric dispersion would inevitably lead to much lower downstream concentrations. Nevertheless, some relatively undiluted air parcels might make it across the Pacific Ocean, and the virulence of aerosolized influenza virus at low concentrations might still be sufficient to cause infections. Influenza studies in mice have shown a greater infectivity of airborne versus intranasal inoculation of virus. Knight demonstrated in volunteers that influenza virus is five to 10 times more infectious when introduced by the aerosol route than by the intranasal route and that adenovirus type 4 is 70 times more infectious by the aerosol route. Aerosolized influenza A virus produces illness in humans at dosages indistinguishable from one infecting particle. Measurements of aerosol concentrations and size distributions made in a pristine area of Alaska indicate that, on average, winter air masses with trajectories off the Pacific Ocean have 100 accumulation-mode-sized particles per cubic centimeter. Some of the aerosols entering North America may contain viable influenza virus. Long-term survival of aerosolized influenza virus. In one study, the mouse LD so was similar at 20 h of aging of aerosolized influenza virus at room temperature to that at earlier times, but the effect of varying the temperature was not considered. It has been shown that influenza virus is maximally stable at low relative humidity. The study of a different enveloped respiratory virus has shown a pronounced stabilizing effect of low temperatures on the survival of aerosolized human corona-virus 229E, even with a high relative humidity. The authors found that at 85% relative humidity, decreasing the temperature from 20 ℃ to 6 ℃ extended the infectious half-life of corona-virus from rv3 to 86 h. At the optimal humidity- rv500J0-nearly 20010 of the virus was still detectable after 6 d in aerosols stored at 20 ℃. The viral half-life was rv70h. Lowering the temperature to 6 ℃ stretched the half-life to > 100 h. The influence of relative humidity may be a confounding factor in assessing the stability of the infectious dose, but it appears that aerosolized corona-virus 229E-and, by implication, influenza virus-can be stable for long periods at low temperatures" [11].
Barbara Oliveiros, et al.: PREPRINT "COVID-19 is having a great impact on public health, mortality and economy world-wide, in spite of the efforts to prevent its epidemic. The SARS-CoV-2 genome is different from that of MERS-CoV and SARS-CoV, although also expected to spread differently according to meteorological- conditions. Our main goal is to investigate the role of some meteorological variables on the expansion of this outbreak. In this study, an exponential model relating the number of accumulated confirmed cases and time was considered. The rate of COVID-19 spread, using as criterion the doubling time of the number of confirmed cases, was used as dependent variable in a linear model that took four independent meteorological variables: temperature, humidity, precipitation and wind speed. Only China cases were considered, to control both cultural aspects and containment policies. Confirmed cases and the 4 meteorological variables were gathered between January 23 and March 1 (39 days) for the 31 provinces of Mainland China. Several periods of time were sampled for each province, obtaining more than one value for the rate of disease progression. Two different periods of time were tested, of 12 and 15 days, along with 3 and 5 different starting points in time, randomly chosen. The median value for each meteorological variable was computed, using the same time period; models with adjusted R square above 0.75 were selected. The rate of progression and doubling time were computed and used to fit a linear regression model. Models were evaluated using alpha = 0.05. Results indicate that the doubling time correlates positively with temperature and inversely with humidity, suggesting that a decrease in the rate of progression of COVID-19 with the arrival of spring and summer in the north- hemisphere. A 20 ℃ increase is expected to delay the doubling time in 1.8 days. Those variables explain 18% of the variation in disease doubling time; the remaining 82% may be related to containment measures, general health policies, population density, transportation or cultural aspects" [12] medRxiv not reviewed.
Yu Han Hailan Yang: "2019 novel corona-virus (SARS‐CoV‐2), which originated in Wuhan, China, has attracted the world's attention over the last month. The Chinese government has taken emergency measures to control the outbreak and has undertaken initial steps in the diagnosis and treatment of 2019 novel corona-virus infection disease (COVID‐19). SARS‐CoV‐2 possesses powerful pathogenicity as well as transmissibility and still holds many mysteries that are yet to be solved, such as whether the virus can be transmitted by asymptomatic patients or by mothers to their infants. Our research presents selected available cases of COVID‐19 in China to better understand the transmission and diagnosis regarding this infectious- disease [13].
The research includes important information regarding the transmission and diagnosis of COVID‐19. The clinical report could be very useful for clinicians. SARS‐CoV‐2 possesses powerful pathogenicity and transmissibility.
Patients with negative swabs may also be diagnosed with COVID‐19. 2019 novel corona-virus (SARS‐CoV‐2) originated in a wet market in Wuhan, China, though the market may not be the only source of the corona-virus.1 SARS‐CoV‐2 is a beta-coronavirus with a single‐stranded, enveloped RNA, belonging to the sarbeco-virus subgenus of the Corona-viridae family. Its RNA genome is 29 891 nucleotides in size, encoding 9860 amino acids.3 Moreover, 26 countries have recorded infected cases, especially in Japan, which has a maximum of 705 cases (as of February 19). Most countries lack experience in the diagnosis and management of COVID‐19. This article reviews various noteworthy cases of COVID‐19 in China for reference, and all cases were verified by local health commissions or multiple media outlets.
1 SARS‐cov‐2 possesses powerful pathogenicity and transmissibility Patient 1, a 56‐year‐old male from Zhejiang, China, was diagnosed with COVID‐19 on February 4. He had no history of exposure to outbreak areas or symptomatic- people. According to a video from the District Public Security Department, on the morning of January 23, this patient and another confirmed patient were present at the same stall for 15 seconds at a vegetable market, where both of them did not wear masks.
Patients 2 and 3, a husband and wife couple from Zhejiang, China, were also confirmed to have the disease on January 25 and 27. Similar to Patient 1, the couple had no history of epidemiological contact. According to a video from the District Public- Security Department, on the afternoon of January 22, Patient 2 and a confirmed individual were at the same clinic for 50 seconds, where both of them did not wear masks.
SARS‐CoV‐2 possesses powerful pathogenicity and transmissibility, being more infectious than SARS‐CoV and MERS‐CoV. Encountering a confirmed patient and being close for 15 or 50 seconds is not the only route of infection, though it is the most likely route in the above two cases. Being infected within a very short exposure time is possible in the absence of masks. The powerful infectivity of SARS‐CoV‐2 may be explained by the latest findings reported by Wrapp D, et al. 8 which showed that the SARS‐CoV‐2 S binds to angiotensin‐converting enzyme 2 (ACE2) receptors with a higher affinity than SARS‐CoV S. Another underlying reason was reported by Zou L et al in that the shedding pattern of viral nucleic -acid in patients infected with SARS‐CoV‐2 is similar to that in patients with influenza and appears to be different from that in patients infected with SARS‐CoV.
SARS‐CoV‐2 often causes cluster transmission, especially within family clusters. In some cities, cases involving cluster transmission accounted for 50% to 80% of all confirmed cases of COVID‐19.Human‐to‐human transmission of SARS‐CoV and MERS‐CoV occurred mainly through nosocomial transmission, and transmission between family- members only occurred in 13% to 21% of MERS cases and 22% to 39% of SARS cases.
SARS‐CoV‐2 can be transmitted by droplets and contact. A study in South Korea showed that many environmental surfaces of patients with MERS were contaminated by MERS‐CoV, and virus RNA was detected from environmental surfaces within 5 days after the last positive PCR of patients' respiratory samples. Guangzhou CDC also found SARS‐CoV‐2 in the house of a confirmed patient, which serves as evidence of contact transmission. live viruses have been found in the feces of patients with COVID‐19, however, the fecal‐oral transmission of the virus has not been shown. Studies have shown that SARS‐CoV may be detected in the feces of most SARS patients, and the virus within feces could survive at room temperature for at least 1 to 2 days. It is possible but infrequent for SARS‐CoV to spread via the fecal‐oral route. In patients with MERS, feces and urine samples also yielded viral RNA. Given the evidence of fecal contamination of SARS‐CoV and MERS‐CoV as well as their ability to survive in feces, it is possible that SARS‐CoV‐2 may also be transmitted through the fecal‐oral route. Additionally, in regard to the expression of ACE2 in the intestine and kidney, SARS‐CoV‐2 may infect these tissues and enter the feces, allowing its potential spread via fecal‐oral route.
The Lancet also reminded doctors not to ignore SARS‐CoV‐2 transmission via ocular surfaces as infected droplets and bodily fluids may easily contaminate the human conjunctival epithelium. Guangfa Wang, a member of the National Health Commission of the People's Republic of China (NHC) expert panel on pneumonia, was exposed to a fever clinic in Wuhan with only his eyes unprotected. He then demonstrated symptoms of conjunctivitis in his left lower eyelid 2 days before the onset of COVID‐19.
On February 19, the NHC published the 6th edition of Guideline on diagnosis and treatment of COVID‐19 (the 6th Guideline for COVID‐19). This document asserted that the transmission of SARS‐CoV‐2 mainly occurs via large droplets and contact. The virus may spread in an unventilated environment with high levels of viral aerosols.
Researchers claimed the spread of SARS‐CoV‐2 could be characterized by super‐spreading events. There is no evidence of super‐spreading events in any medical institution that treats patients suffering from COVID‐19. And a study in South Korea showed that for transmission of MERS‐CoV non-isolated in‐hospital days was the only factor which tended to be higher in super‐spreaders than usual‐spreaders. Whether there are super‐spreaders or not, early isolation is necessary to reduce the size of the outbreak of SARS‐CoV‐2" [13].
Denise R Silva, et al.: "Respiratory viral infections (RVIs) are the most common causes of respiratory infections. The prevalence of respiratory- viruses in adults is under-estimated. Meteorological variations and air pollution are likely to play a role in these infections.
"The objectives of this study were to determine the number of emergency visits for influenza-like illness (ILI) and severe acute respiratory infection (SARI) and to evaluate the association between ILI/SARI, RVI prevalence, and meteorological factors/air pollution, in the city of Porto Alegre, Brazil, from November 2008 to October 2010.
Eleven thousand nine hundred and 53 hospitalizations (adults and children) for respiratory symptoms were correlated with meteorological parameters and air pollutants. In a subset of adults, naso-pharyngeal aspirates were collected and analyzed through IFI test. The data were analyzed using time-series analysis.
Influenza-like illness and SARI were diagnosed in 3698 (30·9%) and 2063 (17·7%) patients, respectively. Thirty-seven (9·0%) samples were positive by IFI and 93 of 410 (22·7%) were IFI and/or PCR positive. In a multivariate logistic regression model, IFI positivity was statistically- associated with absolute humidity, use of air conditioning, and presence of mold in home. Sunshine duration was significantly associated with the frequency of ILI cases. For SARI cases, the variables mean temperature, sunshine duration, relative humidity, and mean concentration of pollutants were significant.
At least 22% of infections in adult patients admitted to ER with respiratory complaints were caused by RVI. The correlations among meteorological variables, air pollution, ILI/SARI cases, and respiratory- viruses demonstrated the relevance of climate factors as significant underlying contributors to the prevalence of RVI" [14].
Jonathan Ciencewicki, et al.: "Despite current regulations, which limit the levels of certain air pollutants, there are still a number of adverse health effects that result from exposure to these agents. Numerous epidemiological -studies have noted an association between the levels of air pollution and hospital admissions for a variety of different health reasons, including a number of respiratory diseases, as well as increased morbidity and mortality associated with various respiratory conditions and diseases. Because of the large impact respiratory- virus infections have on morbidity and even mortality, it is important to understand whether and how exposure to common air pollutants could exacerbate the susceptibility to and severity of respiratory virus infections. This review focuses on current epidemiological and experimental studies, which have examined the association between and effect of air pollutants and respiratory viral infections, as well as potential mechanisms associated with these effects. Examined in this review are U.S. Environmental Protection Agency (EPA) "criteria" pollutants nitrogen dioxide (NO(2)), ozone (O(3)), and particulate matter (PM), as well as indoor pollutants such as environmental tobacco smoke (ETS) and combustion products of biomass fuels. Although a number of studies indicate associations between exposure to air pollutants and increased risk for respiratory- virus infections, potential mechanisms mediating these effects are largely unexplored. Additional studies, both epidemiologic and mechanistic, are necessary to increase our understanding of how exposure to air pollutants could affect respiratory- virus infections, especially in populations already at risk of developing significant morbidity/mortality after infections with respiratory-viruses [15].
Sarah L Warnes, et al.: "The evolution of new and reemerging historic virulent strains of respiratory-viruses from animal reservoirs is a significant threat to human health. Inefficient human-to-human transmission of zoonotic strains may initially limit the spread of transmission, but an infection may be contracted by touching contaminated surfaces. Enveloped viruses are often susceptible to environmental stresses, but the human coronaviruses responsible for SARS and MERS have recently caused increasing concern of contact transmission during outbreaks. We report here that pathogenic human coronavirus 229E remained infectious in a human lung cell culture model following at least 5 days of persistence on a range of common non-biocidal surface materials, including poly-tetra-fluoro-ethylene (Teflon; PTFE), polyvinyl chloride (PVC), ceramic tiles, glass, silicone rubber, and stainless steel. We have shown previously that noro-viruses are destroyed on copper alloy surfaces. In this new study, human coronavirus 229E was rapidly inactivated on a range of copper alloys (within a few minutes for simulated fingertip contamination) and Cu/Zn brasses were very effective at lower copper concentration. Exposure to copper destroyed the viral genomes and irreversibly affected virus morphology, including disintegration of envelope and dispersal of surface spikes. Cu (I) and Cu (II) moieties were responsible for the inactivation, which was enhanced by reactive oxygen species generation on alloy surfaces, resulting in even faster inactivation than was seen with non-enveloped viruses on copper. Copper alloy surfaces could be employed in communal areas and at any mass gatherings to help reduce transmission of respiratory- viruses from contaminated surfaces and protect the public health.
"Respiratory viruses are responsible for more deaths globally than any other infectious agent. Animal coronaviruses that "host jump" to humans result in severe infections with high mortality, such SARS and, more recently, MERS. We show here that a closely related human coronavirus, 229E, which causes upper respiratory tract infection in healthy individuals and serious disease in patients with co-morbidities, remained infectious on surface materials common to public and domestic areas for several days. The low infectious dose means that this is a significant infection risk to anyone touching a contaminated surface. However, rapid inactivation, irreversible destruction of viral RNA, and massive structural damage were observed in coronavirus exposed to copper and copper alloy surfaces. Incorporation of copper alloy surfaces in conjunction with effective cleaning regimens and good clinical practice could help to control transmission of respiratory corona-viruses, including MERS and SARS" [16].
Asmaa Altamimi, et al.: "Our understanding of climate factors and their links to the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) outbreaks is incomplete. This study aimed to estimate the monthly incidence of MERS-CoV cases and to investigate their correlation to climate factors.
The study used aggregated monthly MERS-CoV cases that reported to the Saudi Center for Disease Prevention and Control from the Riyadh Region between November 1, 2012 and December 31, 2018. Data on the meteorological situation throughout the study period was calculated based on Google reports on the Riyadh Region (24.7136°N, 46.6753°E). The Poisson regression was used to estimate the incidence rate ratio (IRR) and its 95% confidence -intervals (CI) for each climate factor.
A total of 712 MERS-CoV cases were included in the analysis (mean age 54.2 ± 9.9 years), and more than half (404) (56.1%) MERS-CoV cases were diagnosed during a five-month period from April to August. The highest peak timing positioned in August 2015, followed by April 2014, June 2017, March 2015, and June 2016. High temperatures (IRR = 1.054, 95% CI: 1.043-1.065) and a high ultraviolet- index (IRR = 1.401, 95% CI: 1.331-1.475) were correlated with a higher incidence of MERS-CoV cases. Low relative humidity (IRR = 0.956, 95% CI: 0.948-0.964) and low wind speed (IRR = 0.945, 95% CI: 0.912-0.979) were correlated with a lower incidence of MERS-CoV cases.
The novel coronavirus, MERS-CoV, is influenced by climate conditions with increasing incidence between April and August. High temperature, high ultraviolet index, low wind speed, and low relative- humidity are contributors to increased MERS-CoV cases. The climate factors must be evaluated in hospitals and community settings and integrated into guidelines to serve as source of control- measures to prevent and eliminate the risk of infection" [17].
And related COVID-19 effect on the air pollution in some world region: what implications?According CNN Digital Expansion 2017. James Griffiths "China has made major progress on air pollution. Wuhan protests show there's still a long way to go" CNN Digital Expansion 2017. James Griffiths Updated 0556 GMT (1356 HKT) July 11, 2019
According A Robichaud: "An interesting fact: I believe that COV-19 virus overall will turn to kill less people in the world than in absence of the virus. Here my thinking: each year air pollution kills 5-9 million people in the world. By slowing down transportation, industries (due to the virus and quarantine, etc.) air- pollution decrease substantially. For example the figure attached is for China taken from satellite and showing very strong decrease of NO2 measured. The air pollution literally vanished. Each year, about 1.1 million premature deaths are attributed to air pollution in China and costing 267 billion yuan (37 billion American dollars) Ref: https://www.scmp.com/news/china/science/article/2166542/air-pollution-killing-1-million-people-and-costing-chinese. On the other hand, corona virus has killed about 6000 so far in China in about 3-4 months, this is much less than that would do air pollution (about 250,000 people). This is may be one of the few good news about the virus. A similar situation is likely to happen in other countries as well but to a smaller scale" (Figure 8 and Figure 9).
 Figure 8: Pollutant drops in Wuhan-Does not Rebound, unlike 2019, No2 levels in 2020 did not rise after the Chinese New Year.
View Figure 8
Figure 8: Pollutant drops in Wuhan-Does not Rebound, unlike 2019, No2 levels in 2020 did not rise after the Chinese New Year.
View Figure 8
 Figure 9: Effect of PM10 concentration in 2012.
View Figure 9
Figure 9: Effect of PM10 concentration in 2012.
View Figure 9
Wei Su, et al.: "There is valid evidence that air pollution is associated with respiratory disease. Few studies have quantified the short-term effects of six air pollutants on influenza-like illness (ILI). This study explores the potential relationship between air pollutants and ILI in Jinan, China. There are still several limitations in our study. One limitation was the ILI case data. In the study, we only analyzed the ILI counts data from three influenza surveillance sentinel hospitals, instead of all hospitals, which may be reduce the effects of air -pollutant on ILI or influenza. The three hospitals continues to monitor the change of ILI, the data has a certain coherence and consistency, and can represent perfectly the influenza trend of Jinan recognized by National Health Commission and WHO, which can be used to exploit the correlation between air- pollutants and ILI. The second is that the simple daily averaging method might result in measurement errors for pollutants that have a correspondingly large spatial variability with different air pollutant concentrations among 28 surveillance locations. If the surveillance location and surveillance method did not change systematically with time, the exposure measurement data collected can perfectly reveal the association based on territory-wide time-series data of both influenza and air pollutants. The third is that the data were collected from Jinan and over two years, which may not perfectly illustrate the association between air pollutants and ILI; thus, the long-term data and more cities would be added for further study.
Despite these limitations, our results still illuminated that short-term exposure to ambient pm2.5, PM10, SO2 and CO may increase the occurrence of ILI and O3 can decrease the incidence of ILI in Jinan City, China. Further investigation is needed to expand to other areas in Shandong Province, which can further provide more evidence to explain the association between air- pollutants and ILI, build an early warning information system and conduct health risk assessment, and help people take essential measures to protect their health in time.
A total of 81,459 ILI counts were collected, and the average concentrations of PM2.5, PM10, O3, CO, SO2 and NO2 were 67.8 µg/m3, 131.76 µg/m3, 109.85 µg/m3, 1133 µg/m3, 33.06 µg/m3 and 44.38 µg/m3, respectively. A 10 µg/m3 increase in concentration of PM2.5, PM10, CO at lag0 and SO2 at lag01, was positively associated with a 1.0137 (95% confidence interval (CI): 1.0083-1.0192), 1.0074 (95% CI: 1.0041-1.0107), 1.0288 (95% CI: 1.0127-1.0451), and 1.0008 (95% CI: 1.0003-1.0012) of the relative risk (RR) of ILI, respectively. While, O3 (lag5) was negatively- associated with ILI (RR 0.9863; 95% CI: 0.9787-0.9939), and no significant association was observed with NO2, which can increase the incidence of ILI in the two-pollutant model. A short-term delayed impact of PM2.5, PM10, SO2 at lag02 and CO, O3 at lag05 was also observed. People aged 25-59, 5-14 and 0-4 were found to be significantly susceptible to PM2.5, PM10, CO; and all age groups were significantly susceptible to SO2; People aged ≥ 60 year, 5-14 and 0-4 were found to be significantly negative-associations with O3.
"Air-pollutants, especially PM2.5, PM10, CO and SO2, can increase the risk of ILI in Jinan. The government should create regulatory policies to reduce the level of air-pollutants and remind people to practice preventative and control- measures to decrease the incidence of ILI on pollution days" [3].
Papadogeorgou G, et al.: "Fine particle (PM2.5) levels have been decreasing in the USA over the past decades. Our goal was to assess the current literature to characterize the association between PM2.5 and adverse health at low exposure levels. We reviewed 26 papers that examined the association between short- and long-term exposure to PM2.5 and cardio-respiratory morbidity and mortality. There is evidence suggesting that these associations are stronger at lower- levels. There are certain methodological and interpretational limitations specific to studies of low PM2.5 levels, and further methodological development is warranted. There is strong agreement across studies that air pollution effects on adverse health are still observable at low concentrations, even well below current US- standards. These findings suggest that US standards need to be reevaluated, given that further improving air quality has the potential of benefiting public health" [3].
Jonathan O Anderson, et al.: "The WHO estimates that particulate matter (PM) air pollution contributes to approximately 800,000 premature deaths each year, ranking it the 13th leading cause of mortality worldwide. Many studies show that the relationship is deeper and far more complicated than originally thought. PM is a portion of air pollution that is made up of extremely small particles and liquid droplets containing acids, organic chemicals, metals, and soil or dust particles" [5].
It is clear by science the role played by air pollution related some relevant respiratory disease and related toxicology and death related. The same is clear that in COVID-19 diffusion in some industrial area it induced the stop of great part of industrial activity with high reduction of air pollutants release as easily seen in the figure in this work. It is also interesting the diffusion of some virus disease like COVID-19 in other region whit high level of air pollution. (North Italy). After observing the figure presented in this work and PROF. GALLO thinking is possible to notice that there are latitude relationship. Also the air pollution relationship tell us something related. The reducing of air pollution in Wuhan region after COVID-19 is clear as showed by figure presented in this work. It is due by the stop of many industrial activity and related the measure adopted by government.
In the same time after all strictly measure adopted also another fact emerged: The reducing in air pollution. But now the diffusion of the disease in china seem to reduce highly as seen in world media information. It is an opinion of the authors that also the measure to reduce air poisoning must to be evaluated in this kind of pathology diffusion (HYPOTESYS).
None.
This work is produced without any diagnostic or therapeutic intent only to produce new research hypothesis to be evaluated.