Posterior rib stress fractures may infrequently occur in baseball pitchers at the first or second rib. Lower thoracic rib stress fractures, however, are a rare phenomenon with only a few cases described at the collegiate or professional level. We present the unique case of a 16-year-old male, right-handed, high school baseball pitcher who presented with a few months of worsening right upper back pain. Physical exam was notable for tenderness to palpation at the T7 level between the spine and the scapula with an otherwise normal cervical and shoulder exam. Initial x-ray imaging of the shoulder was negative, but subsequent magnetic resonance imaging of the chest wall illustrated a stress fracture in the posterior right 7th rib. He underwent 4-5 weeks of rest followed by 4-6 weeks of targeted physical therapy. He returned to play after completion of his rehabilitation with resolution of his symptoms.
Posterior rib stress fracture pitcher
Posterior rib stress fractures are rare injuries that may occur in the overhead athlete, most commonly at the first or second rib level in collegiate or professional players. The purpose of this article is to present the unique case of a lower thoracic posterior rib stress fracture in a high school pitcher, as well as to describe the clinical presentation, diagnosis, and management of this condition.
A 16-year-old right-handed male baseball pitcher presented with right-sided upper back pain located deep to the scapula. He stated the pain had been intermittently present for the past three years but that there was significant progression over the past few months. He described the pain as mild during throwing or exercise but with significant worsening after completion of these activities. His pain was not worse during any particular phase of his throwing cycle. On initial evaluation, he described his right upper back pain as 6/10 in severity, as well as sore, tender, tingling and cramping. Symptoms worsened with twisting of the shoulder and improved with standing upright. He also endorsed a "crunching" sensation when moving the right shoulder. Review of systems was otherwise negative.
On physical examination, he was a healthy appearing male in no acute distress. Focused exam of the right shoulder showed no gross instability, atrophy or effusion. He displayed full and painless range of motion in the spine with no instability or crepitus noted. There was tenderness to palpation at the T7 level between scapula and spine. There was minimal scapular asymmetry with shoulder range of motion or wall push-ups. Strength and sensation were grossly intact.
Initial x-ray of the right shoulder was negative for fracture or dislocation. It revealed a prominent right C7 transverse process. Magnetic Resonance Imaging (MRI) was obtained of the chest wall (without contrast) and the right shoulder (without contrast). MRI chest wall illustrated a focus of marrow edema in the posterior right 7th rib, medial to the inferior aspect of the scapula (Figure 1). No findings of scapular bursitis were present. No labrum or rotator cuff pathology was identified.
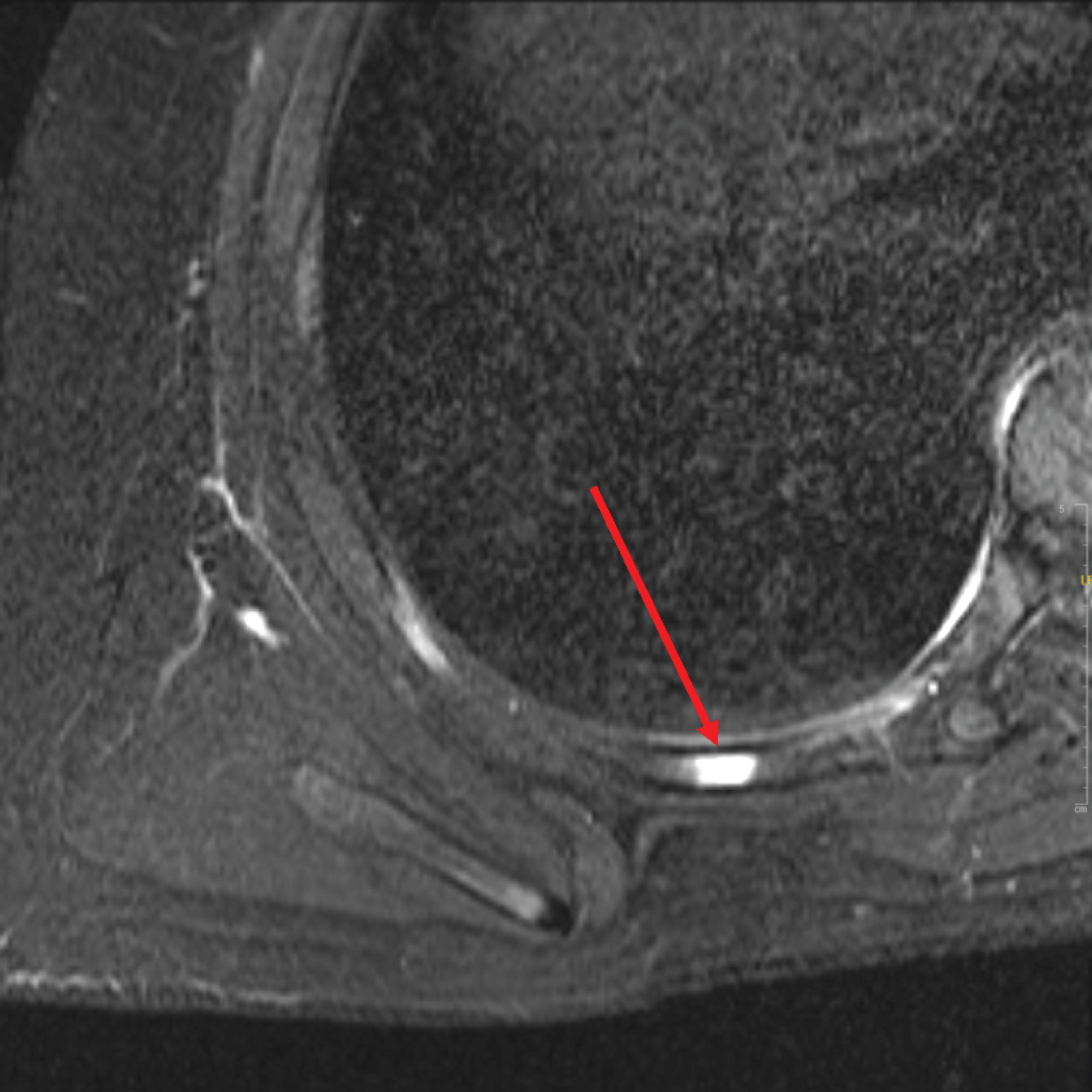 Figure 1: MRI chest without contrast shows a focus of marrow edema signal (red arrow) in the posterior right 7th rib, medial to the inferior aspect of the scapula concerning for stress injury or fracture.
View Figure 1
Figure 1: MRI chest without contrast shows a focus of marrow edema signal (red arrow) in the posterior right 7th rib, medial to the inferior aspect of the scapula concerning for stress injury or fracture.
View Figure 1
The patient was advised to rest from pitching, batting or other upper body straining activity for approximately 4-6 weeks. He was allowed to begin physical therapy at approximately 4-weeks to improve scapular kinetics, balance, and work on strengthening. He was counseled on activity modifications for all other activities and workouts.
He was evaluated 5-weeks later and had refrained from pitching, throwing, batting, or upper extremity sports. He reported 60% improvement in his pain and symptoms. He was held from baseball activities for another 4-6 weeks while continuing physical therapy. It was recommended that once cleared to throw, he focus on throwing biomechanics and continue exercises learned during physical therapy. He returned to play after complete resolution of symptoms. He did not require medications, bracing, injections, or further imaging.
Posterior rib stress fractures are rarely seen in overhead athletes. No epidemiologic data is available given the low incidence and prevalence of these injuries. Multiple case reports have described first and second rib posterior stress fractures as a result of overhead throwing or rowing in collegiate and professional athletes [1-8]. Even fewer cases are present that describe lower rib stress fractures in baseball and softball pitchers. To our knowledge, only four such cases have been reported [9,10]. However, no cases have been reported in high-school athletes. It is important to identify these injuries early as they may result in prolonged symptom courses with increased time before full return to play.
The pathophysiology of these injuries is complex but thought to be secondary to pathology of the serratus anterior and external oblique muscles. Repetitive, high-stress forces may be translated to the ribs, particularly when coupled with inadequate core strength and poor thoracic mobility [10]. Another theorized etiology is secondary to opposing contractions of the latissimus dorsi and external oblique muscles [9,10]. Patients may present with point tenderness medial to the scapula at a particular thoracic level. Pleuritis may be present and pain may worsen with inspiration.
Onset of these injuries is generally insidious and without the result of focal injuries or insult [9]. Most commonly, these injuries occur on the dominant side [9]. Diagnosis is first guided by physical examination. Symptoms may appear similar to intercostal muscle strains, which can make the diagnosis challenging, particularly given the high prevalence of abdominal and thoracic muscle strains in pitchers [10]. Plain films should be done next to assist with the diagnosis but may be negative early in the disease course. If indeterminate, bone scans or MRI can be done to confirm the diagnosis. MRI may illustrate marrow edema (Figure 1), displacement of the bone, or a discrete fracture line at the posterolateral ribs [9,10].
Management includes pain control, rest, activity modification, physical therapy with scapular and thoracic focus, and evaluation of throwing mechanics (4-6 weeks). Athletes may then gradually return to play by 8-10 weeks [9,10]. Non-Steroid Anti-Inflammatory Drugs (NSAIDs) have been used but may negatively influence the healing process. Special attention should also be paid to vitamin D levels, as low levels of serum 25-OH-vitamin D have been shown to correlate with stress fractures [10].