There is a high prevalence of, and lack of a systematic reduction in running-related injuries. Despite decades of research, there remains a lack of consensus about risk factors and solutions for running injury in the scientific literature. In response to suggestions that running injuries should be viewed from alternative conceptual frameworks, this paper has viewed running from an engineering perspective to suggest causes and solutions based on the 'fundamental principles' approach that characterises engineering. Based on this view, training error, overweight, previous injury, lack of conditioning/fatigue, age, technique and forefoot structure (prevalence of hallux valgus) are suggested to be risk factors for running injury. Engineering-based solutions including technique and footwear changes are also provided to minimise the impact of these risk factors.
"Man is a product of nature, a part of the Universe. The Universe is operated under exact natural laws. Man is a product of millions of years of evolution. He adapts himself to the laws of nature or he perishes." James Hervey Johnson
Science can be been defined as a process of observation, experiment and deduction, the object of which is the determination of general laws [1]. Engineering has been defined as the application of known laws to solve any problem with which society is confronted [2]. The runner is subject to the laws of motion that apply to every moving object, and to other natural laws that govern biological organisms. This opinion piece arguesthat adopting an engineering perspective could help understand and resolve the problem of running-related injury. The absence of a systematic reduction in Injury frequency, despite decades of research has led to suggestions that the scientific method has been unsuccessful in resolving the problem of running injuries [3-6].
Running for recreation first became very popular in the1970s [7] and was followed soon after by studies on the prevalence of injuries in runners. Results of these studies varied, with injury incidence ranging between 15% and 85% [8-27] (Figure 1). However, there seems to be noapparent systematic change in injury incidence over time.
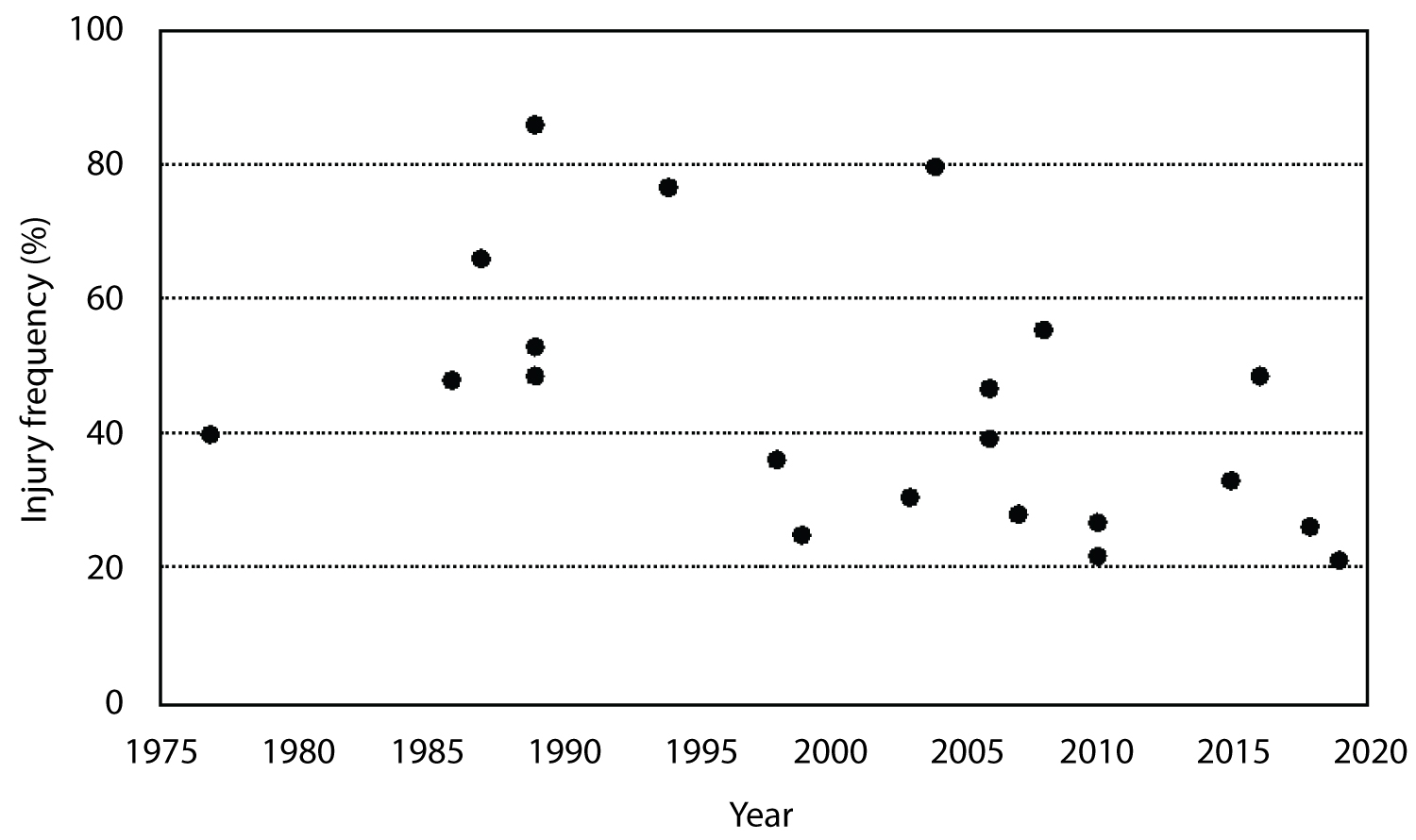 Figure 1: Summary of frequency of running injuries from 1970-present. View Figure 1
Figure 1: Summary of frequency of running injuries from 1970-present. View Figure 1
The runners in the 1970s and 1980s were different to the runners in the current millennium. The participants captured by studies performed in the 1970s and 1980s were dedicated runners, aiming to win, lean, primarily just trained by running, were mostly (75%) male [19], and were around mid thirties in age [8,12,15,19,26]. The runners in more recent studies are primarily recreational, running a marathon with the goal to simply finish, often overweight, often involved in cross-training activities in addition to running, and are around mid forties in age [9,10,24]. The majority of runners are also now female (54%). The populations studied in various epidemiological investigations also differ, with some comprising novice runners and others comprising competitive runners [10,23,24]. These differences in the populations studied confound injury frequency statistics, making comparisons between studies difficult to interpret.
The definition of a running injury also varies between studies. In one study, an injury was defined as that which required medical attention [28], whereas others have defined injury by the time that running could not be performed, with the threshold duration for 'injury' often different between studies [29]. Studies have also defined a running injury simply as pain or discomfort [23]. Variation in definitions of injury will clearly impact on the injury frequencies reported and likely accounts for some of random variation and lack of a systematic change in injury frequency over the years [30,31]. Given the confounding issues, the results of studies investigating the frequency of running injury can only be interpreted as providing no evidence of change in injury prevalence over the four decades that they span.
"We are drowning in information but starving of wisdom". EO Wilson.
Scientific investigations have attempted to identify factors that are related to injury incidence or that discriminate between injured and injury free runners. By identifying risk factors, it is hoped that targeted interventions can be developed to eliminate or reduce risk of injury. The lack of change in injury prevalence suggests that attempts to explain the factors underpinning running-related injury by application of the scientific method have not been successful. Table 1 summarises risk factors identified in studies from the 1970s to present.
Table 1: Summary of risk factors for running-related injury identified from published scientific studies. View Table 1
A positive association between injury occurrence and age is a consistent feature in the literature. Factors that have been collectively described as 'training errors' also frequently appear, supporting early suggestions that training errors constitute the primary cause (60%) of running injuries [32,33]. The direction of the association between training errors and running injury appears consistent across studies (Table 1). Other factors and their association with injury are less clear, with different studies finding positive, negative and no association with injury risk for the same risk factor. Possible explanations for the lack of consensus for some risk factors include random sample variation, definition of terms, choice of measurement tool, statistical power to identify effects, and the aforementioned changes in average characteristics of the running population over the years. Without recourse to natural laws that characterise an engineering approach to problem solving, it is easy to become confused by mixed findings and to 'drown in information'. In such circumstances, science tends to make judgements based on the rigour of individual study designs (i.e. the evidence-based pyramid), but this model has been widely criticised [34-37] and has failed to progress understanding of, or provide solutions to, the problem of running injuries [6].
"Everything in biology is ultimately obedient to the laws of physics and chemistry and has arisen by evolution through natural selection" EO Wilson (1999)
Lack of progress in the understanding and prevention of running injuries in the scientific discipline of biomechanics has been recently acknowledged [5,6]. It has been suggested that alternative conceptual approaches are warranted [38-43]. A fresh view of the problem from an engineering perspective could provide a solution.
The majority of the most significant discoveries in the history of science were made by rigorous application of the scientific method, using bold hypotheses deduced from natural laws [44]. A law is a fact or fundamental principle that has never been disproven [45]. It is by applying these laws that engineering tackles problems [2]. As stated so eloquently by Harvard Emeritus Professor EO Wilson [46], humans are subject to the laws of physics and chemistry and possess traits selected by evolutionary pressures. It is through the lens of these fundamental principles that we aim to understand the available evidence on running injuries, beginning with a description of the demands of running from the perspective of Newtonian mechanics.
Running is a spring-like gait pattern characterised by a double flight phase with potential and kinetic energy in sync and the centre of mass being at its lowest point over a compressed support leg at mid stance [7]. Humans spontaneously switch from walking to running as velocity increases. Preferred transition velocity typically occurs around 2.0 m/s (7.2 km/h; 4.5 mph) [47-49]. Recent work suggest that the trigger for transitioning from walking to running is lower limb discomfort resulting from increased forces as velocity increases, i.e. the pendulum gait of walking becomes inappropriate for the forces resulting from the velocity of locomotion, and a spring-like gait is preferred [50-52]. Given that the running gait is initiated in response to increased ground reaction forces, a closer examination of how the forces are dealt with is warranted.
Figure 2 depicts a vertical ground reaction force trace typical of a rear-foot striking runner. As around 80% of runners use this landing strategy [53], the kinetics depicted here will form the basis for the rest of the discussion on running kinetics.
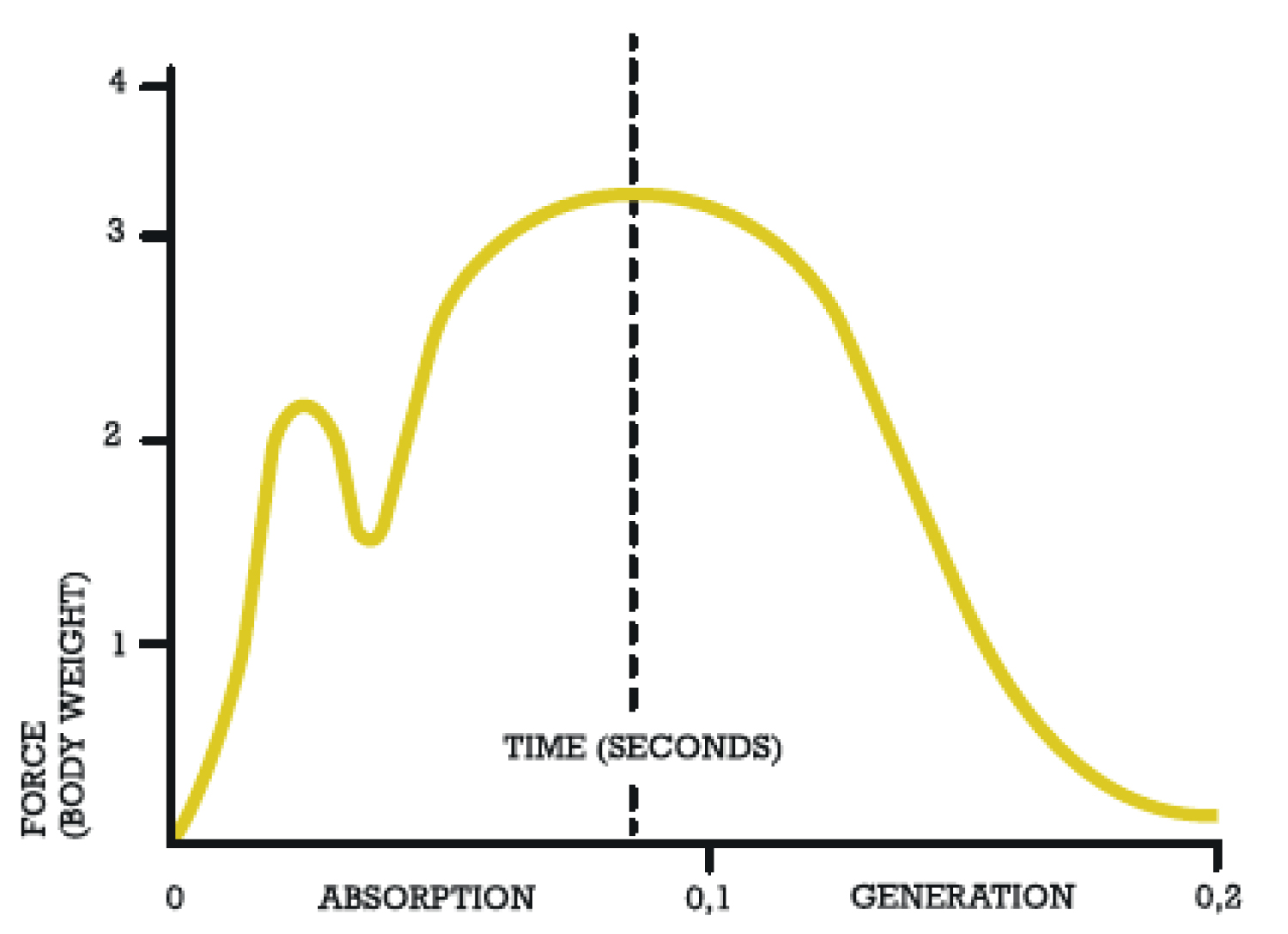 Figure 2: A typical vertical ground reaction force trace for a rearfoot strike runner. View Figure 2
Figure 2: A typical vertical ground reaction force trace for a rearfoot strike runner. View Figure 2
The first peak is a passive forcepeak or impact transient associated with the shock of contact with the ground, and a portion of the body mass suddenly decelerating. This is attenuated by footwear and landing technique (a forefoot strike pattern) [54] and modified by passive characteristics of the running surface [7]. It is generally smaller and of shorter duration than the second peak, but the rate of rise to this initial peak has been implicated in injury, specifically knee joint injury and stress fractures [55,56]. The second (active) peak is centred about mid stance and is the highest force experienced by the runner where they are essentially compressed between the vertically-oriented gravitational vector and the opposing ground reaction force. The magnitude of the active peak force has also been implicated in injury [57]. As both passive and active peaks are determined by the momentum of the runner prior to impact and the landing pattern, Newton's second law (F = ma) dictates that both peaks must be influenced by body mass, velocity and technique.
As long as the motion (velocity and trajectory) of the body's centre of mass, and the mass itself, is unchanged, footwear cannot alter the magnitude of the second peak of ground reaction force. Footwear can, however, change the pressure application to different areas of the foot, influencing the direction of ground reaction force vectors relative to joints, and thus, the resulting joint moments [58]. Footwear can also influence stability of the runner while they are absorbing the forces of impact, influencing the direction of ground reaction force vectors and joint movements [59].
The multi-articular structure of the human body allows for forces to be directed and handled in many different ways. It has been argued that the structure and function of various joints, the foot, and indeed the skeleton as a whole, results from evolutionary selective pressure to cope with and direct the forces arising from running [60]. Many of the adaptations are suggested to minimise the perpendicular distance between ground reaction force vectors and joint centres, thus reducing joint moments, muscular forces needed to counteract those moments, and therefore whole-body energy expenditure. The latter is an accepted driving force in evolutionary adaptation. Excessive joint moments, or moments about joints where either the joint or the supporting tissues (muscle, tendon, ligament) are not evolved for and/or not conditioned to deal with them, have been suggested as a source of injury [61].
As moments are the resultant of the magnitude and perpendicular distance of the ground reaction force vector from joint centres, Newtonian mechanics dictates that factors influencing kinetics (discussed in the section above) and running kinematics (joint angles/technique/footwear) must influence joint loads.
The spring-like gait pattern of running makes use of elastic properties of muscle and tendons to both absorb force and store energy in the first half of stance, and to return stored energy in the propulsive phase, minimising the energy cost of locomotion [52,60].
From an engineering perspective, tendons can be viewed as having both elastic and viscous properties. Elastic materials change length or deform by an amount directly proportional to the applied force up to their elastic limit. Viscous materials are characterised by deformations that are time-dependent and rate-of-change dependent, where the rate of deformation is directly proportional to the applied force. Elasticity and viscosity are described by Hooke's law and Newton's model of a hydraulic piston known as a dashpot [62]. Muscle tendon complexes act with both elastic and viscous properties.
Tendon overuse injuries are common in runners, are positively associated with age [63], and are more prevalent in runners over 40-years-old [18,27]. Achilles tendinopathy alone accounts for 7-11% of all running injuries [15,33,64]. As a viscoelastic material, tendon overuse injury can be understood using the laws of material fatigue from engineering.
Put simply, a material fails when its tensile strength is exceeded. In a viscoelastic material, tensile strength can be exceeded by a one-off excessive load, too many and/or too frequent repetitions of load application or combinations of these factors [65]. The relationship between load and frequency of load application can be represented by a simple material fatigue curve shown in Figure 3. Injury occurs when the material is subjected to a load/frequency combination that is above the curve, whereas injury is avoided in situations where the load/frequency combination falls below the theoretical curve.
 Figure 3: Material fatigue curve showing theoretical relationship between stress, frequency of stress application and the effect of stress/frequency combinations on overuse injury risk. View Figure 3
Figure 3: Material fatigue curve showing theoretical relationship between stress, frequency of stress application and the effect of stress/frequency combinations on overuse injury risk. View Figure 3
Tendon load is determined by force divided by cross-sectional area, and by the elastic properties of the tendon or the 'stress-strain' relationship. The stress-strain relationship describes how much tendon is elongated under load (stiffness) and thus its ability to absorb strain energy. Fatigue [66], previous injury [67] and ageing [63] are known to impair the viscoelastic properties of muscle-tendon complexes. Tendon stiffness increases with ageing [63,65,68], accounting for the higher prevalence of Achilles tendon injury with age in runners. Loss of the spring-like properties of tendon alter how forces are absorbed and generated during the running cycle, changing kinematics and kinetics and the risk of other injury types [69].
Having viewed running and the properties of muscle and tendon using fundamental principles of engineering, it is now possible to suggest factors that are likely to increase injury risk, explain common injury patterns observed in the literature, and suggest engineering-based solutions.
From an engineering view, it can be said that all overuse injuries are training errors.
A runner that sustains an overuse running injury must have exceeded their limit of running distance, frequency and/or intensity in such a way that the stress-frequency combination results in damage to the injured structure [70]. It is a case of too much stress for the tissue capacity too often or too soon. The effect of increasing training velocity on forces is easily understood with Newton's 2nd law, whereby any increase in acceleration increases force at impact. Also from Newton's 2nd law, force is determined by the product of mass and acceleration. By deduction, high or increased body mass will increase the forces involved (both passive and active peaks). A positive association of body mass with injury risk confirms body mass to be risk factor for injury [10,19,41]. The effects of training error (i.e. increasing running velocity, fatigue from too much distance, frequency and lack of conditioning) on injury risk can be pictured on the stress-frequency curve (Figure 4).
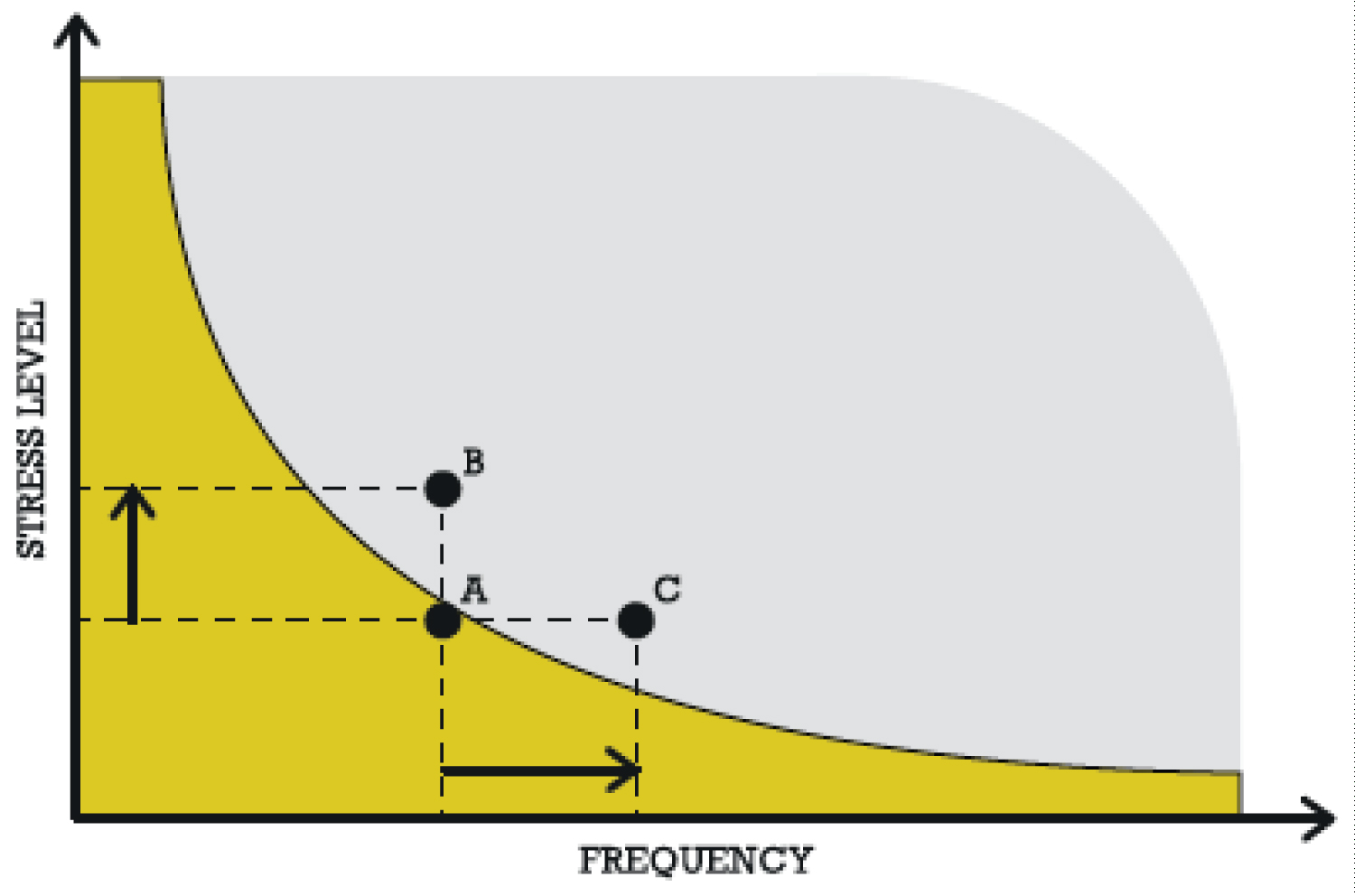 Figure 4: Increased velocity increases impact force. For a given frequency, stress increases moving the runner from A 'uninjured' to B in the 'injury' region. For a given velocity/stress, increasing distance/frequency of stress cycles moves the runner from A 'uninjured' to C in the 'injury' region. View Figure 4
Figure 4: Increased velocity increases impact force. For a given frequency, stress increases moving the runner from A 'uninjured' to B in the 'injury' region. For a given velocity/stress, increasing distance/frequency of stress cycles moves the runner from A 'uninjured' to C in the 'injury' region. View Figure 4
As dictated by Newton's 2nd law, peak braking forces and peak active forces increase with velocity [71]. For any given frequency of stress application to tissues, increased force per stress cycle has the potential to exceed tissue capacity and result in overuse injury [70]. Positive associations between running intensity and injury shown in Table 1 support this [12,15,19,22,41]. Similarly, for a given velocity/stress, increasing the frequency of stress cycles by increasing training frequency or mileage also has the potential to exceed tissue capacity and result in overuse injury. A consistent positive association between training frequency and mileage confirms this suggestion [12,15,16,26,38,40].
Too much mileage, too high an intensity, or training too often can induce fatigue, particularly when a runner is poorly conditioned/inexperienced or previously injured. Material fatigue in engineering is a reduced tolerance for any stress-frequency combination. Reduced tolerance can be visualised by a lowering of the injury threshold as shown in Figure 5 and is supported by the positive association of mileage, frequency, intensity and previous injury with injury risk, and the negative association of initial fitness with injury risk (Table 1).
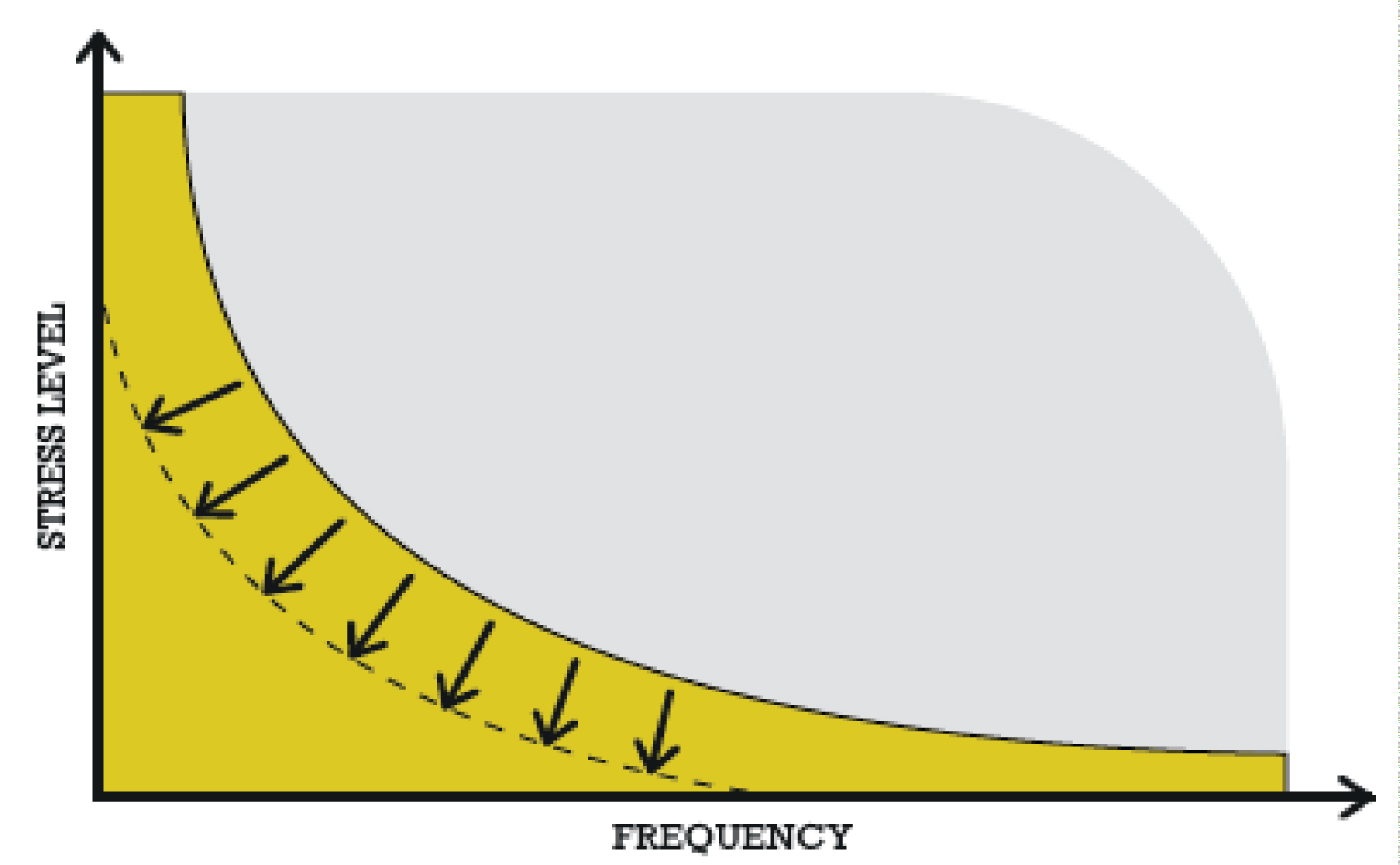 Figure 5: Reduced tolerance for any stress-frequency combination resulting from poor conditioning/fatigue/ageing lowers the injury threshold and increases the area of the injury region. View Figure 5
Figure 5: Reduced tolerance for any stress-frequency combination resulting from poor conditioning/fatigue/ageing lowers the injury threshold and increases the area of the injury region. View Figure 5
The reduced tolerance for any stress/frequency combination characteristic of fatigue and previous injury is indistinguishable from the effects of ageing. The degeneration of tendons and other soft tissues with ageing is well known [63,65,68]. The increase in injury rate (specifically lower-limb tendons) with advancing age is also well documented [15,18,27,33,64].
The loss of elastic function in tendons has important implications for ageing runners. To avoid exceeding the tensile capacity of stiffening tendons, runners over 40-yrs-old must find a way to minimise stress, frequency or the stress/frequency combination that could result in material fatigue. Engineering solutions include a decrease in velocity and or a change in technique that alters gait towards a walking/inverted pendulum-type action and away from the spring-like gait that places high demand on tendon elasticity. Direct comparisons of kinetics and kinematics between young and older runners confirm that both solutions are adopted [72]. Data also show inverse associations of peak running velocity with age, decreased peak vertical force and horizontal propulsive force, decreased ankle power and increased contact time [69]. Figure 6 illustrates the effect of increased ground contact time on peak active force. From Newton's 2nd law, the total impulse (force-time integral) comprises lower force over longer time. The increased passive impact peak force is indicative of a rearfoot strike pattern that reduces the demand on the Achilles tendon [73].
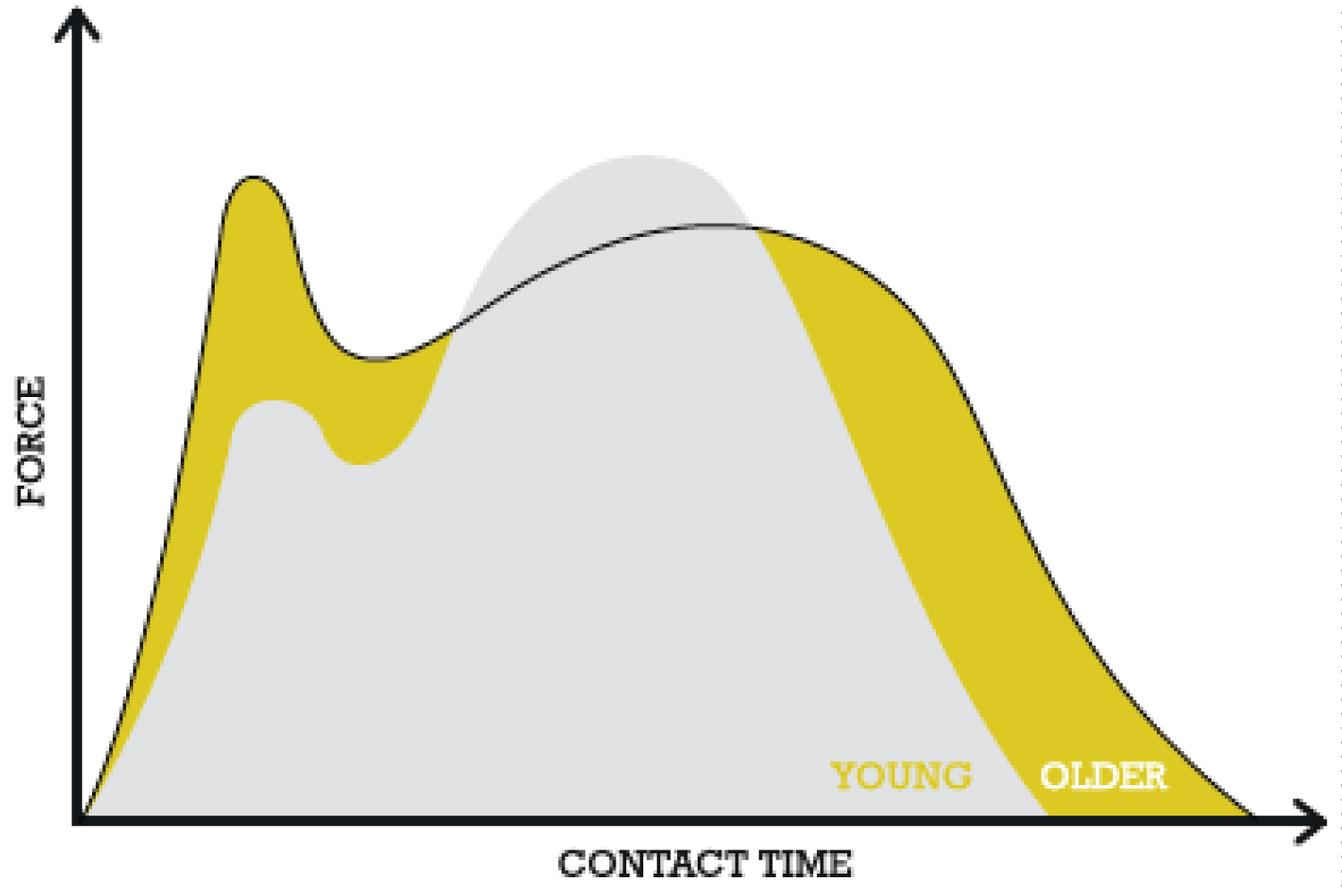 Figure 6: Comparison of average vertical ground reaction force between younger and older runners at a common speed, adapted from [72]. View Figure 6
Figure 6: Comparison of average vertical ground reaction force between younger and older runners at a common speed, adapted from [72]. View Figure 6
However, increased passive impact peak forces and loading rates increase the risk of stress-fracture and knee injury unless attenuated by rear-foot cushioning [72]. Therefore, footwear choice, especially cushioning, becomes an important consideration for runners > 40-yrs-old. The high loading rates associated with the rear-foot strategy characteristic of runners > 40-yrs-old are known to be even higher without shoe cushioning [54] further supporting the recommendation for cushioned shoes in runners over the age of 40.
It has been shown that a forefoot strike running style reduces passive impact peaks and loading rates [54]. It has also been argued that this technique, performed in minimally-cushioned shoes, might be a strategy to reduce common running injuries [74]. For runners over 40-yrs-old, and from an engineering view, this is a recipe for disaster. The elongated contact time and rear-foot strike pattern characteristics of the older runner are protective changes in gait strategy to compensate for the loss of elasticity and capacity of tendons to absorb high loads [69]. Achilles tendon and ankle loading is greatly increased in forefoot strike running [73,75] which is likely to overload tendons compromised by age. Engineering principles suggest that runners over 40 yrs avoid minimal footwear and forefoot strike running techniques to avoid high elastic demands on tendons with compromised elastic properties.
The rear foot landing strategy adopted by most recreational runners, and characteristic of the runners over 40 yrs of age, results in a passive impact peak in vertical ground reaction force caused by a portion of the runner's mass rapidly decelerating [54]. The rate at which this force is absorbed has been implicated in injury, particularly at the knee joint [55,56]. Moreover, the knee joint is the most injured site, comprising 42.1% of all running injuries [23,38]. The magnitude of moments at the knee is a causative factor in knee injury and pain [76].
Newtonian mechanics and the basic principles of levers that underpin joint moments dictate that the magnitude of the braking force, and the subsequent moment at the knee joint, can be altered by the landing position of the foot relative to the knee and the hip. These relative positions have been termed 'overstride' and are closely related to stride length. Studies confirm that landing with an extended leg increases braking forces and sagittal plane joint moments at the knee [77,78], and that reducing overstride lowers knee joint loading [79].
Basic principles of levers and joint moments suggest that adopting a technique that reduces stride length and overstride could reduce risks of injury to the knee. Increasing stride frequency is one element of technique that reduces stride length and overstride and, therefore, loading and stress at the knee joint [80]. The effect of stride length on knee joint moment is illustrated in Figure 7.
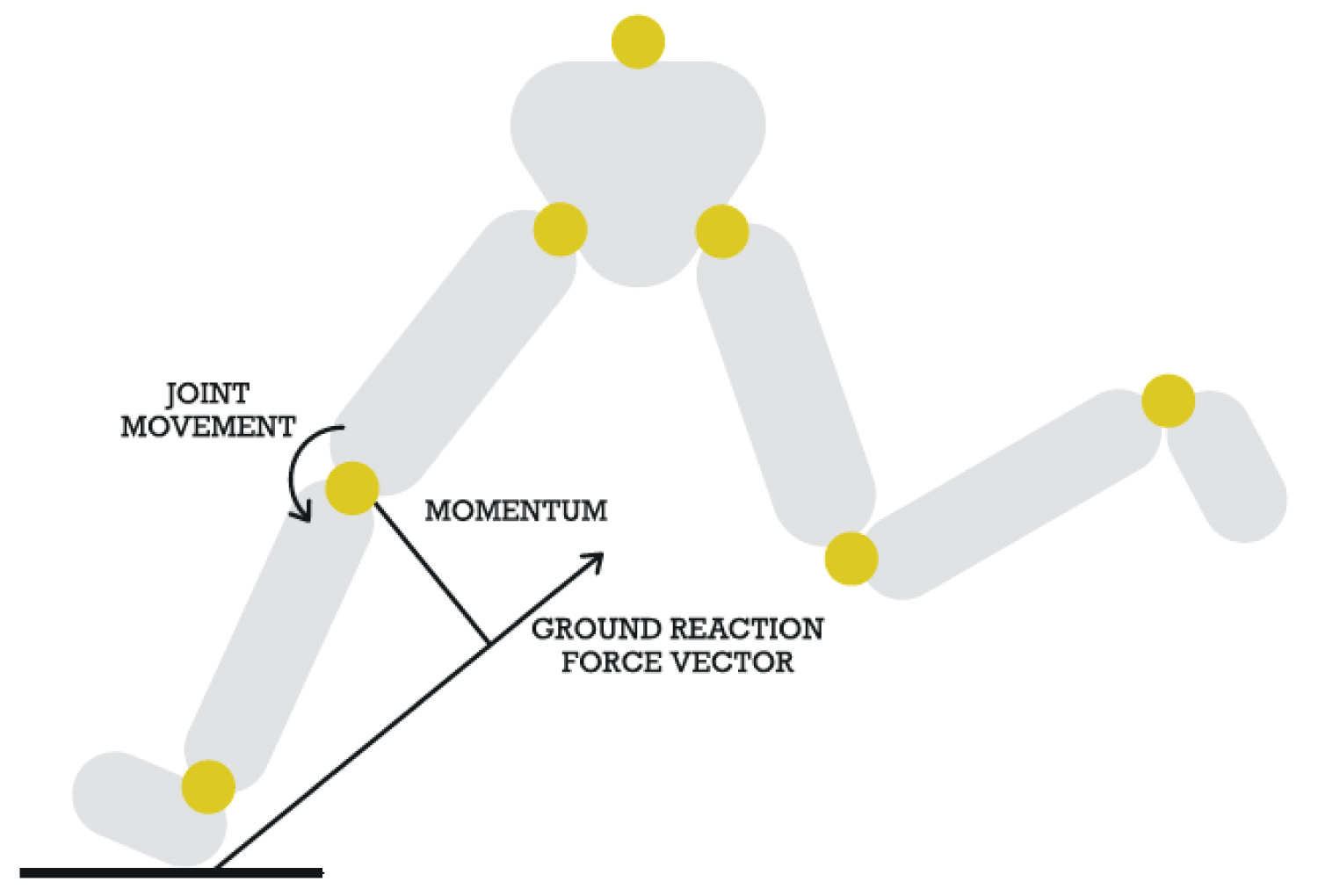 Figure 7: The effect of over striding on the direction of the vertical ground reaction force vector, moment arm length and knee joint moment. View Figure 7
Figure 7: The effect of over striding on the direction of the vertical ground reaction force vector, moment arm length and knee joint moment. View Figure 7
Leonardo DaVinci wrote that the foot is a masterpiece of engineering and a work of art.
The purpose of the foot is to support and control the direction of the body weight as it falls forwards during the stance phase of locomotion, necessitating stability [81-83].
Given the magnitude of the forces that must be controlled and directed during stance, an unstable base poses a potential injury risk. As previously stated, the knee is the most injured joint in runners. Patellofemoral Pain Syndrome (PFPS) is the most common running-related knee injury, followed closely by Iliotibial Band Syndrome (ITBS) [23]. Altered frontal plane hip and knee joint movements, and pronation of the foot during the stance phase of running have been linked to these injury types, and differentiate injured from uninjured runners [84-86]. Knee abduction, femoral internal rotation, tibial external rotation, and foot pronation, have been theoretically linked to injury in a population of patients with PFPS [87]. This is unsurprising given the knee is a sagittal plane joint. Interventions to normalise/reduce excessive frontal plane motion at the knee by increasing hip abduction and external rotation strength do not decrease hip or knee frontal plane peak joint angles or joint excursions during the stance phase of running [88-90]. Moreover, associations between hip strength and frontal plane hip and knee peak angles and joint excursions while running and jumping are weak [88,91]. Studies exploring the distal end of the kinetic chain have utilised barefoot and minimal footwear, and foot muscle strengthening interventions to reduce surrogate metrics associated with injury at the knee and other sites [92,93]. Injury rates, however, remain unchanged. Despite the foot being the base of support, the influence of foot structure on pronation and knee joint kinematics in running has received little attention, and the few studies examining links between metrics of foot structure and injury risk in running have mixed findings (Table 1).
With fundamental principles of physics in mind, an engineering view suggests a larger base of support (i.e. the effective area of the supporting foot), that is widest at the front, would best provide the necessary stability for the control and direction of bodyweight. It has been claimed that mother nature is an engineer, in that natural selection appears to produce the simplest solutions to functional problems [94]. Unsurprisingly, comparisons of habitually-unshod with habitually-shod populations consistently report wider (particularly at the front) feet in unshod populations, in agreement with that predicted by fundamental principles governing stability [95-99]. Observational studies on habitually-barefoot populations also demonstrate the benefits of a wide forefoot in the form of more uniform distribution of pressure through the entire plantar surface of the supporting foot during walking [95], and reduced peak pressure and pressure-time integral under the forefoot when running [100]. Given that pressure is force divided by area of contact, these observations support the natural selection of a wide forefoot to serve a support function.
Of importance to forefoot width and the stabilisation role of the foot is the position and function of the great toe. The notable spread and abducted position of this toe from the others characterises habitually-barefoot populations [95,96,99]. Increased thickness and an abducted position of the great toe in humans are evolved-functional adaptations providing directional stability in bipedal locomotion [100]. These adaptations are important considering that direction of ground-reaction forces (and the resulting joint moments created) contribute to injury [101-103]. The importance of a wide and stable forefoot cannot be overstated, as instability here has consequences for the structure of the arch and foot function in general. The twisted plate model [104] is generally accepted as the most accurate model of foot function explaining the shock absorbing, stabilising and propulsive characteristics of the foot during the gait cycle, as well as the development of pathological high-rigid and flat-collapsed arches. Arch height is determined by rotation of the rear foot on the forefoot [104,105] which, in turn, is determined by the ability of musculature to compensate for forefoot instability. A high-rigid arch (overly twisted foot plate) occurs when lower-limb musculature compensates for forefoot instability, creating external rotation of the hip, supination of the rear foot on the forefoot and a high-rigid arch. Supination of the rear foot on the forefoot locks the subtalar joint and limits ankle range [106]. This inflexible foot and ankle is a poor shock absorber and stress fractures and lateral ankle sprains are common consequences [107]. Associations of arch height and forefoot instability with injury have been previously reported [14,27]. With age and/or increased bodyweight, muscles lose the strength to compensate for the instability of the forefoot and the rear foot and entire lower kinetic chain collapses inwards. Over time, this excessive pronation of the rear foot on the forefoot breaks down the soft tissues of the foot resulting in a dysfunctional collapsed/flat arch (overly twisted foot plate) and knee injuries [107]. A recent study showing a strong correlation of great toe valgus angle with pronation and frontal plane knee movement [59], and the previously reported positive association of navicular drop with running injury [10] support this link.
Instability of the forefoot, secondary to a squashed great toe position (hallux valgus) is a common affliction affecting 23% of 18-60 year-olds and over 36% over 60 [108]. Moreover, a recent robust prospective longitudinal study of monozygotic twins showed the development of the condition to be solely due to years of wearing narrow shoes [109]. That compressive forces alter foot structure is in accordance with Wolff's law of bone adaptation to imposed forces [110], and highlights the importance of shoes that respect the anatomical shape of the human foot.
This paper has highlighted the prevalence of, and lack of a systematic reduction in running-related injuries, and the lack of consensus about risk factors for injury in the scientific literature, despite decades of research. In response to suggestions that running injuries should be viewed from alternative conceptual frameworks, this paper has viewed the mechanics and demands of running from an engineering perspective. Based on this view, we suggest training error, overweight, previous injury, lack of conditioning/fatigue, age, technique and forefoot structure (prevalence of hallux valgus) are risk factors for running injury.
To minimise the impact of these risk factors the following solutions are recommended:
• Lose excess body mass before commencing a running programme.
• Adhere to the principle of progressive overload.
• Runners > 40-yrs-old should choose shoes with adequate cushioning to protect against high impact loads associated with the rear foot strike strategy that evolves naturally with age to safeguard ageing tendons.
• Runners > 40-yrs-old should avoid minimal footwear and gait retraining aimed at encouraging a forefoot strike pattern.
• Runners should avoid overstriding. Increasing cadence is a simple means to achieve this.
• Runners should choose running and everyday shoes that respect the anatomical shape of the human foot to avoid and reverse the development of forefoot deformity.